
















Abstract
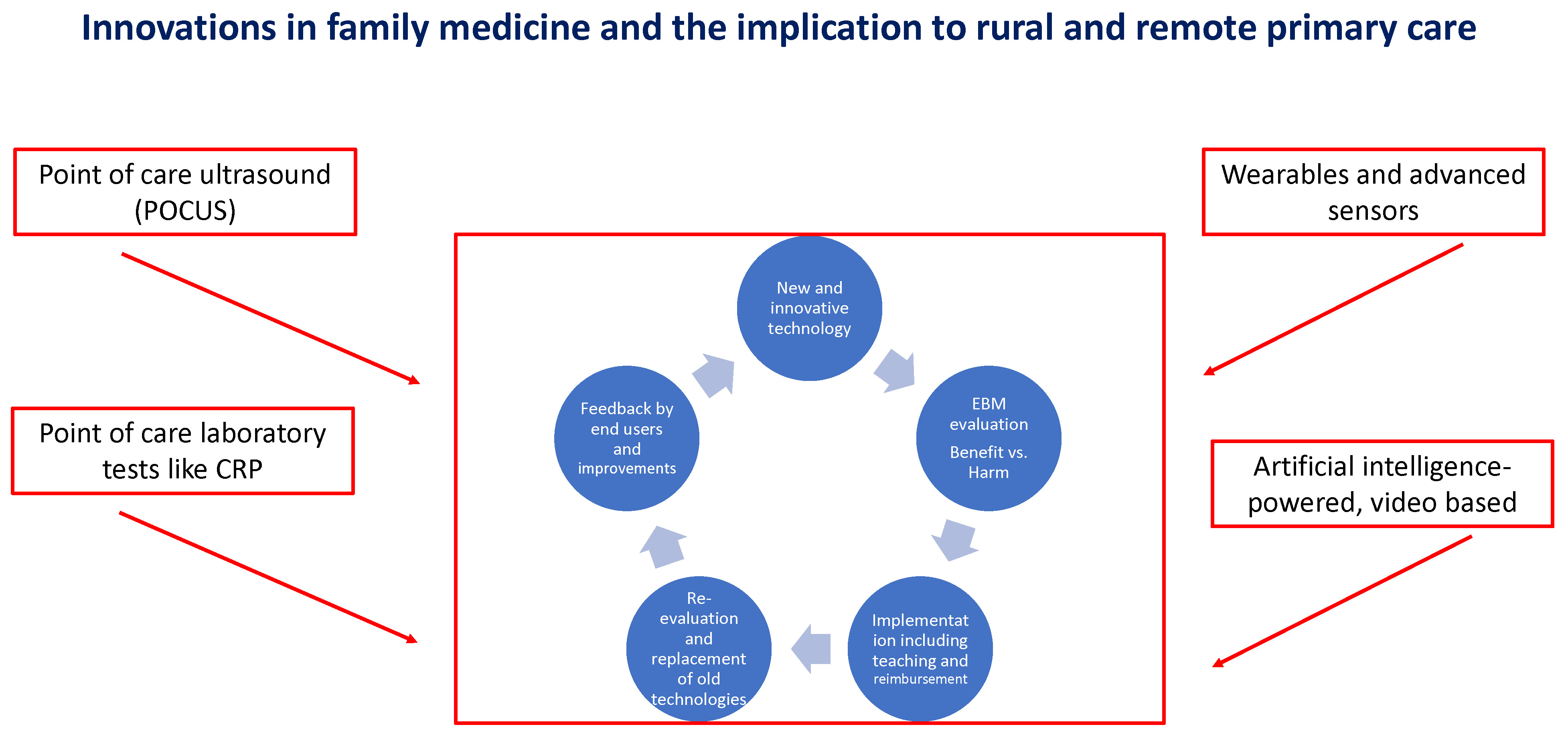
Modern medicine is characterized by introducing new innovative medications specially designed after understanding the mechanisms of diseases. Such process revolutionized the management of many diseases, but is usually more relevant to secondary and tertiary care. However, in parallel, we are observing an emerging wave of new technologies, devices and applications with particular relevance to primary care and significant implications for rural and remote areas. The approval processes by regulatory authorities all around the world are more flexible and less demanding in comparison to the approval of new medications. This process may lead to innovative treatments where the balance between benefit and harm is not clear and well documented in the conventional way of prospective randomized clinical trials. On the other hand, these technologies are adopted by the patients, in the case of free-of-charge applications or “on the shelf” devices, or by authorities, for example in the case of remote and telemedicine consultations.
In such a way, disciplines that ignore these technologies or are too cautious and slow in adaptation can find themselves trailing behind. Family medicine and especially remote and rural medicine can benefit a lot. We should be on the frontline in the considerate adoption of relevant technologies, and in this way improve our patients’ health and keep family medicine attractive to the young generation of physicians. This editorial is aimed to serve as a window to this new era with the presentation of some of these technologies.
Key words: C-reactive protein, point-of-care ultrasound, point-of-care laboratory tests, medical applications, rural medicine
Point of care ultrasound
Point of care ultrasound (POCUS) is an example of a technology that had been adopted by other disciplines as complementary to or replacing the physical examination. In a meta-analysis evaluating 34 studies, the overall pooled sensitivity for lung auscultation was 37% and specificity was 89%. Likelihood ratios (LRs), and area under the curve (AUC) of auscultation for congestive heart failure, pneumonia and obstructive lung diseases were low.1 The authors summarize “Lung auscultation has a low sensitivity in different clinical settings and patient populations, thereby hampering its clinical utility. When better diagnostic modalities are available, they should replace lung auscultation. Only in resource-limited settings, with a high prevalence of disease and in experienced hands, lung auscultation has still a role”. The editor of Chest had an opposite point of view and in an editorial, he answers the question (Should point-of-care ultrasound examination be routine practice in the evaluation of the acutely breathless patient?) by a clear “No”.2 These 2 different points of view may represent different clinical scenarios, case-mix and interpretations of the scientific evidence, but clearly represent the need to discuss the place of the stethoscope compared to POCUS in evaluating patients with respiratory symptoms in primary care.
Point-of-care ultrasound will not replace the specialist in imaging. It is complementary to the traditional physical examination and maybe even superior in specific cases. For example, in the case of hepatomegaly, we can better estimate its size and cause using POCUS. On suspicion of pneumonia, we can make the diagnosis faster and without using radiation. Using POCUS will improve the diagnosis and may even save time during the visit.
In another systematic review, the authors evaluated the use of POCUS by family physicians.3 They included a total of 51 full-text articles. The POCUS was applied for a variety of purposes, with the majority of scans focused on abdominal and obstetric indications. Focused POCUS scans were reported to have higher diagnostic accuracy and be associated with less harm than more comprehensive scans or screening scans. In the cited systematic review, the length of a focused POCUS procedure and its accuracy had been evaluated – and for example, it would take 5–12 min to have an abdominal POCUS with a specificity of 99% and sensitivity of 82% while evaluating the kidneys.
In conclusion, POCUS has the potential to be an important tool for the family physician and may possibly reduce healthcare costs, especially in remote and rural areas. It is time for the wide implementation of POCUS in family medicine. The plan should be multidimensional, focusing on training, reimbursement, and continuousevaluation and research.
Point-of-care C-reactive protein test
Several systematic reviews evaluated the place of point-of-care laboratory tests in primary care.4, 5, 6 There are many such tests relevant in primary care. Their utilization is variable according to availability, costs, reimbursement plans, alternative traditional laboratory tests availability, the complexity of performance, and accuracy, among many other considerations. They may be especially useful in remote and rural areas where the availability of laboratories is lower, and on-the-spot results may narrow the differential diagnosis and spare the need for referral to the emergency room or other specialists that may request costly and complicated evacuation.
One such attractive test is the point-of-care C-reactive protein (CRP) test. C-reactive protein point-of-care testing (POCT) may reduce diagnostic uncertainty and enhance antibiotic stewardship. In primary care, respiratory tract infections (RTIs) are the most common reason for inappropriate antibiotic prescribing, which is a major driver for antibiotic resistance.
The impact of CRP-POCT on antibiotic prescribing for RTIs in primary care has been evaluated in a systematic review.7 Thirteen studies comprising 9844 participants met the inclusion criteria. Meta-analyses showed that CRP-POCT significantly reduced immediate antibiotic prescribing at the index consultation compared with usual care (risk ratio (RR): 0.79, 95% confidence interval (95% CI): 0.70–0.90, p = 0.0003, I2 = 76%) but not during 28-day follow-up. The immediate effect was sustained at 12 months. In children, CRP-POCT reduced antibiotic prescribing when CRP (cutoff) guidance was provided. Meta-analyses showed significantly higher rates of re-consultation within 30 days. Clinical recovery, resolution of symptoms and number of hospital admissions were not significantly different between CRP-POCT and usual care, which points to the safety of the test. The authors concluded that CRP-POCT can reduce immediate antibiotic prescribing for RTIs in primary care (number needed to (NNT) for benefit = 8) at the expense of increased re-consultations (NNT for harm = 27).
In conclusion, CRP-POCT is highly available at a reasonable cost and should be adopted in primary care. Other useful tests that should be considered for widespread use are troponin, D-dimer and specific tests for various infectious diseases (viral, bacterial and fungal).
Telemedicine and teleconsultations
A quick PubMed search will yield more than 50,000 publications about telemedicine, and narrowing the search to primary care and family medicine will yield around 10,000 papers. Further narrowing the search to rural and remote settings will give us around 1000 publications, most of them from recent years, especially published during the COVID-19 pandemic.
Petrazzuoli et al. concluded that telemedicine can be used as an effective tool among disadvantaged populations and may reduce inequities, but care must be taken to avoid it as a tool to cut or replace services in rural and remote areas.8 This had been stated at the World Heath Organization (WHO) Europe 70th Regional Meeting by World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians (WONCA) Europe and European Rural and Isolated Practitioners Association (EURIPA). It seems that phone consultations gained more popularity in Europe than video consultations.9 It is beyond the scope of this editorial to discuss the benefits, challenges and obstacles of telemedicine in remote and rural settings, and it is time to perform a systematic review and evaluation to give us insights into the post-pandemic era.
Software solutions for remote measurement of physiological parameters
In the past, we used laboratories to evaluate physiological parameters. But for decades we have been moving to portable devices that are easy to wear and use, and the evaluations are been performed in ambulatory and primary care settings. A few examples are portable 24-hour blood pressure monitoring, loop recorders to detect rhythm abnormalities, and sleep tests for the diagnosis of sleep apnea, among many others.
New wereable devices can detect rhythm abnormalities, and their accuracy had been evaluated in a systematic review.10 Nine observational studies (n = 1581) assessing the sensitivity and specificity of wrist-worn wearables in detecting AF in patients with and without a history of AF were included. In patients with a history of AF, the overall sensitivity was high. Specificity significantly differed between the devices. Wrist-worn wearable devices demonstrate promising results in detecting AF in patients with paroxysmal AF. However, more rigorous prospective data are needed to understand the limitations of these devices in regard to varying specificities that may lead to unintended overdiagnosis and overtreatment.
Other wearable devices are used to measure steps, energy expenditure and heart rate, and their accuracy had been evaluated in 2 systematic reviews.11, 12 They concluded that commercial wearable devices are accurate for measuring steps and heart rate in laboratory-based settings, but this varies by manufacturer and device type.11 However, none of the tested devices proved to be accurate in measuring energy expenditure.12
There are new and promising technologies that use artificial intelligence (AI)-powered, video-based, 100% software solution that easily integrates into any app or workflow to allow measurement of a wide range of physiologic parameters, using only the end user’s smartphone, tablet or laptop.13 With this technology, blood pressure, O2 saturation, respiratory rate, and heart rate can be assessed. After regulatory approval, using these technologies can be easily applicable in remote and rural areas for distance monitoring of patients and in aiding the clinical decision-making about treatment, management and referrals for emergency room or specialist consultation.
Conclusion
In this short editorial, I gave a few examples of new and innovative technologies that should be considered for widespread use in primary care and especially in remote and rural settings. Rural primary care should not take it as a threat, but rather as an opportunity to introduce advanced modalities of care without the need for secondary and tertiary expensive and hard-to-attend healthcare facilities. It can be used to empower family physicians and primary care providers and to reduce the inequity between the peripheral and central areas all around Europe. Each of these new technologies deserves deep discussions and research about their utility and effectiveness in primary care, as well as the ways to introduce them, teach the patients how to use them, and develop mechanisms of the reimbursement of the time and costs spent on the specific technology. However, these considerations should not delay the implementation – otherwise, the outlined solutions will be adopted, for example, as home-based tests with remote or application-derived interpretation, and such implementation will bypass the family physician.