
















Abstract
Background. Malnutrition rates in pediatric celiac disease (CD) patients range from 20.2% to 67.3%.
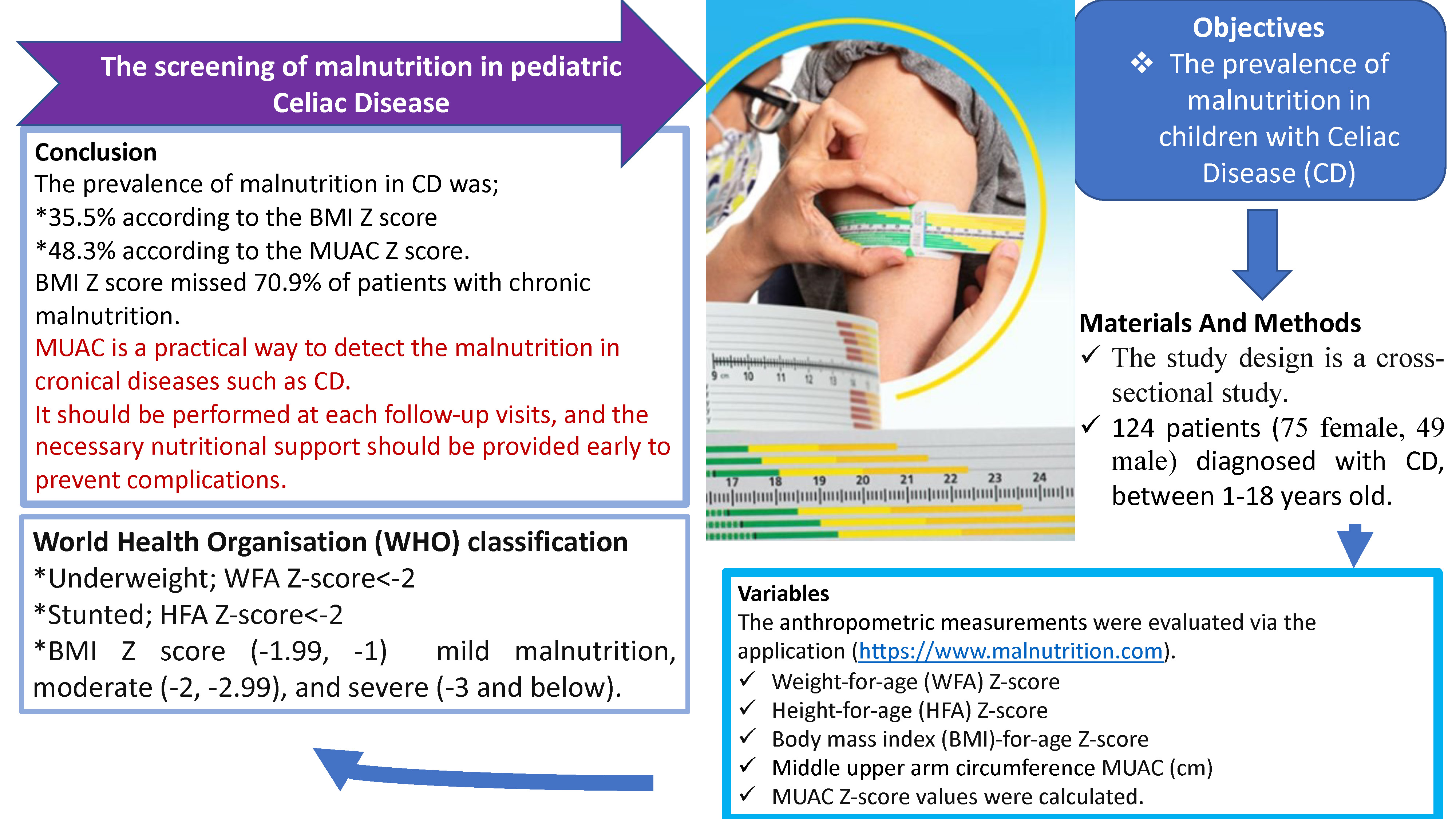
Objectives. To investigate the prevalence of malnutrition in pediatric CD patients in Turkey using different anthropometric measurements, including mid-upper arm circumference (MUAC).
Materials and methods. This prospective study included 124 patients aged 1–18 years with a diagnosis of CD, admitted to the Pediatric Gastroenterology Outpatient Clinic of Adana City Training and Research Hospital, Turkey. The anthropometric measurements, including weight-for-age (WFA) Z-score, height-for-age (HFA) Z-score, body mass index (BMI)-for-age Z-score, MUAC [cm], and MUAC Z-score were calculated.
Results. The study analyzed 75 female (60.5%) and 49 male (39.5%) patients with a mean age of 9.83 ±4.1 years. While 44 patients (35.5%) had malnutrition according to their BMI Z-scores, 60 patients (48.4%) had malnutrition based on their MUAC Z-scores. The number of patients with stunting (HFA value below −2) was 24 (19.4%), and the WFA value was below −2 in 27 (21.8%) patients. Furthermore, the BMI Z-score failed to identify chronic malnutrition in 70.9% of patients. There was a positive linear correlation (r = 0.396) between the BMI value and the MUAC value (p < 0.001). However, the degree of agreement between the BMI Z-scores and MUAC Z-scores was weak (κ: 0.300).
Conclusions. The MUAC Z-score successfully detected acute and chronic malnutrition and should be included in standard anthropometric measurements at follow-up nutritional assessments in CD patients.
Key words: pediatric, malnutrition, celiac disease, mid-upper arm circumference (MUAC)
Background
Celiac disease (CD) is a chronic autoimmune gastrointestinal tract disease characterized by villus atrophy and malabsorption triggered by gluten in genetically susceptible individuals.1 It is one of the most common genetic diseases, with the global prevalence of 1% in children.2 Inadequate nutrient, vitamin and mineral absorption in the villi due to ongoing mucosal damage causes severe nutritional deficiencies in CD.3 Patients with CD may also present with underlying complications such as failure to thrive and weight loss, although 10% of CD patients can be obese, and they should not be overlooked.4 Furthermore, CD can present with various gastrointestinal complaints, such as diarrhea, cramping, bloating, flatulence, and nausea, along with other non-classical symptoms, such as iron deficiency anemia, elevated transaminases, constipation, ataxia, lethargy, osteoporosis, and dyspepsia.5 Other complications include developmental delay, stunting, delayed puberty, weight loss, and loss of muscle mass. Due to this wide spectrum of clinical presentations in CD, there can be some delay in its diagnosis, with underdiagnoses increasing the malnutrition risk of patients. Therefore, the malnutrition status of all patients should be assessed at the first presentation and in the follow-up period.
Studies show that malnutrition rates in CD pediatric patients range from 20.2% to 67.3%,6, 7, 8 and malnourished patients, especially those with severe malnutrition, have a higher mortality rate from childhood diseases such as diarrhea and pneumonia.9 Therefore, accurate and timely diagnosis of children suffering from malnutrition, or those at risk, is essential in all chronic diseases, especially CD. Indeed, it is possible to protect such patients from the deleterious and irreversible effects of undernutrition on growth10 in order to reduce the 9-fold increased risk of mortality in this population.11
Various anthropometric measurements have been used to identify high-risk cases of chronic diseases such as CD. Mid-upper arm circumference (MUAC) is an easy and cheap anthropometric measurement used to identify malnutrition and is a good predictor of survival in children.12 Since 2009, the World Health Organization (WHO) has recommended using MUAC as anthropometric criterion for admission to nutrition programs.13
Objectives
The study aimed to investigate the prevalence of malnutrition in children with CD in Adana, Turkey, and to compare different anthropometric measurements with MUAC.
Materials and methods
Study design
The prospective study assessed the height and weight of each patient with a Harpenden Portable Stadiometer model 603VR (Holtain Ltd, Crymych, UK) and the same healthcare professional performed each measurement. Three measurements of the MUAC of the left arm were simultaneously measured by the same physician using inflexible MUAC bands, and the mean values were used for the analysis.14
Study setting
A total of 124 patients diagnosed with CD and aged between 1 and 18 years were followed up at the Pediatric Gastroenterology Outpatient Clinic of Adana City Training and Research Hospital between September 18, 2017 and November 30, 2022.
Participants
A pediatric gastroenterology specialist conducted the follow-up of CD patients, who had to be diagnosed according to the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) criteria using biopsy for inclusion. Patients or legal guardians gave written informed consent to participate in the study, and patient files provided data on age, gender, age at CD diagnosis, disease duration, and laboratory parameters.
Variables
The measured height and weight parameters of the patients were evaluated using the 6D malnutrition awareness application (s://www.malnutrition.com), and weight-for-age (WFA) Z-score, height-for-age (HFA) Z-score, body mass index (BMI)-for-age Z-score, MUAC [cm], and MUAC Z-score values were calculated and recorded.15, 16 Taking into account the recommendations of the WHO, those with a WFA Z-score below −2 were considered underweight, and those with an HFA Z-score below −2 were considered stunted. According to the BMI Z-score, malnutrition was classified as mild malnutrition (from −1 to −1.99), moderate malnutrition (from −2 to −2.99) or severe malnutrition (−3 and below).
Data sources and measurement
The study used 2 versions of the MUAC band, patented in 2019, to determine the MUAC Z-score. One band was designed for infants aged 2–59 months, and the other for children aged 5–18 years. The bands contain markings for different ages, including 5, 5 1⁄2, 6, 6 1⁄2, 7, 7 1⁄2, 8, 8 1⁄2, 9, 9 1⁄2, 10, 10 1⁄2, 11, 12, 13, 14, 15, 16, 17, and 18 years, which indicate malnutrition using colors.17
Study size
We assumed that a mean effect size of 0.3 would be accepted as a difference in the mean of the parameters, and the sample size was calculated as 124 patients (95% power analysis) at an α significance level of 0.05. The Ethical Ethics Committee of Adana City Training and Research Hospital approved the study (approval No. 2286 issued during meeting No. 117), which adhered to the principles of the Declaration of Helsinki.
Statistical analyses
Statistical analysis of the data was performed with the IBM SPSS v. 25.0 package (IBM Corp., Armonk, USA). The Shapiro–Wilk test was used to determine whether the parameters evaluated in the study showed a normal distribution. Categorical measurements were summarized as numbers and percentages, and continuous measurements as mean ± standard deviation (M ±SD; median and quarters when the data distribution differed from normal). The χ2 test compared categorical expressions, and Cohen’s κ coefficient evaluated the differences between MUAC and BMI values. Meanwhile, Spearman’s rho correlation test determined the relationship between continuous measurements. A value of p < 0.05 was considered statistically significant for all tests.
Results
The study included 124 patients, 75 female (60.5%) and 49 male (39.5%), which is in line with the literature on CD predominance in females.18 The mean age of the patients was 9.83 ±4.1 years, the mean age at diagnosis was 6.39 ±3.7 years and the mean follow-up period was 41.1 ±24.5 months. Forty-four (35.5%) of the patients were malnourished based on BMI Z-score, and 60 (48.4%) had malnutrition according to their MUAC Z-score (Table 1). Furthermore, the number of patients with stunting (HFA Z-score below −2) was 24 (19.4%), and 27 (21.8%) patients obtained WFA Z-scores below −2. Table 2 presents anthropometric measurements of the patients. Twenty-five (20.2%) patients had comorbidities. Guided by the anamnesis and celiac antibody titers, it was noted that 88 patients (71%) showed complete adherence to the celiac diet.
The analysis of the correlation between malnutrition parameters revealed a significant moderate positive linear correlation (r = 0.396) between BMI and MUAC (p < 0.001) (Figure 1). The degree of agreement between the Z-scores of BMI and MUAC was weak (κ: 0.300) (Table 3), although the positive linear correlation between HFA Z-score and MUAC values was moderate (r = 0.268) and significant (p = 0.003). Also, the WFA Z-score and MUAC values showed a moderate positive linear correlation (r = 0.318, p < 0.01) (Figure 2, Figure 3).
The analysis between laboratory values and the MUAC value showed a positive correlation between hemoglobin (Hb) (r = 0.572) and mean corpuscular volume (MCV) (r = 0.387) (both p < 0.01). However, there was no correlation between the malnutrition rate and gender, according to the MUAC Z-score (p = 0.933).
Discussion
This study determined the prevalence of malnutrition in pediatric CD patients using various anthropometric measurements, with malnutrition detected most frequently using the MUAC (48.3%). The malnutrition parameters revealed a significant moderate positive correlation between BMI and MUAC, although WFA, BMI and HFA did not recognize many malnourished patients.
The clinical manifestations of CD are diverse, and there has been an increase in the diagnosis rate of patients presenting with subtle clinical findings due to clinicians’ awareness. In patients with CD, malabsorption results from damaged villi of the small intestine and constitutes the primary cause of extraintestinal findings.19 The majority of patients develop malnutrition due to the prolonged time to diagnosis or failure to ensure the necessary protein, vitamin and calorie intake when on a strict celiac diet.20 The prevalence of malnutrition in children with CD varies by country, but is still high. Indeed, the rate of patients with a WFA Z-score below −2 was 22.4% in an Iranian study,5 while another study reported low WFA in 30.8% and stunting in 21.5% of patients.21
There is no standard anthropometric measure to define malnutrition in the pediatric population older than 5 years, and the classifications proposed by Waterlow and Gomez et al. were not considered during the study design, as they are historical.22, 23 The most commonly used measurement methods in this group of children are WFA, HFA and BMI, which are plotted on standard percentile curves and classified according to the population. However, SD values have been used more recently as they better indicate deviation from the general child population. In 2007, the WHO recommended using the BMI-for-age Z-score, as it is considered the best indicator for identifying malnutrition in school-age children and adolescents.24 Despite being recommended, it does not seem possible to implement this method for every patient in a standard outpatient setting, since calculating BMI and evaluating BMI Z-scores impose an additional burden on healthcare personnel. Therefore, MUAC has been used to screen for childhood malnutrition and nutritional status, as it is a more rapid and easily measurable parameter, and it was approved as an independent diagnostic criterion for malnutrition in 2007.25 Indeed, the American Society for Parenteral and Enteral Nutrition (ASPEN) panel determined MUAC to be a more sensitive prognostic indicator for mortality than weight-for-height parameters in malnourished pediatric patients, and recommended that MUAC measurements be part of a full anthropometric assessment.
Previous studies have shown a close relationship between MUAC and BMI values in this age group.26 Arm measurements such as MUAC and triceps skinfold thickness are better predictors of body composition and malnutrition than WFA, HFA and BMI, which do not make a distinction between muscle and fat mass.27 The current study is the first to examine malnutrition in children with CD using the MUAC Z-score. However, the frequency of malnutrition detected using MUAC was only 48.3%. Similarly to studies in other patient groups, it was determined that the MUAC value had a moderate positive correlation with the WFA, HFA and BMI Z-scores.28, 29
Chronic malnutrition in children is recognized using the duration of the symptoms and the HFA Z-score, with a score below −2 considered stunting by the WHO. Evaluation of the HFA Z-score in the current study showed a non-negligible incidence of stunting, as it was found in 24 patients (19%). Stunting is common in patients with CD, although its reasons remain unclear. According to several hypotheses, malnutrition, growth hormone resistance or low levels of insulin-like growth factor 1 (IGF-1) are responsible for stunting.30, 31, 32 An Iranian study found stunting in 10% of patients, based on the WHO criteria. In the current study, patients with comorbidities were not excluded, with 25 patients (20.2%) presenting comorbidities, 10 (41.6%) of whom had stunting, which may explain the increased incidence of chronic malnutrition. Nonetheless, only 7 (29.1%) patients considered to have chronic malnutrition were malnourished according to the BMI Z-score, while 14 (58.3%) were malnourished according to the MUAC Z-score. As such, both measures appear insufficient for defining chronic malnutrition, although it appears that using the MUAC Z-score will lead to better rates of chronic malnutrition diagnosis.
Considering the parameters for classification of malnutrition demonstrate a moderate agreement between the MUAC measurment and BMI Z-scores. But the calculation of the MUAC Z score is weakly correlated with BMI Z scores. (Table 3). This discrepancy is likely due to the fact that the Z-score calculations use American children for reference.14
Limitations
Study limitations include the lack of MUAC Z-score percentiles of the Turkish population and the absence of most nutritional laboratory parameters. Also, as the study center is a tertiary hospital, CD patients included in the study may have been in worse health condition, which may have skewed the sample.
Conclusions
The prevalence of malnutrition in patients with CD was 35.5% according to the BMI Z-scores, while it was 48.3% according to the MUAC Z-scores. In addition, 19% of the patients had chronic malnutrition based on the HFA measurements, and BMI Z-score failed to identify chronic malnutrition in 70.9% of patients. For this reason, in the group of patients at high risk of malnutrition, nutrition should be evaluated in detail at each follow-up. Moreover, multiple anthropometric measurements should be performed, and the necessary nutritional support should be provided early to prevent complications.
Supplementary data
The supplementary files are available at https://doi.org/
10.5281/zenodo.7725284. The package contains the following files:
Supplementary File 1. SPSS data.
Supplementary File 2. Supplementary test of normality and Shapiro–Wilk tests.


