Abstract
Background. Achillotendinopathy is reported as an overuse disorder and/or degeneration change of the tendon. The diagnosis of tendinopathy is not always easy through imaging modalities. The B-mode grayscale sonography and power Doppler are well-established methods aimed at visualising tendon structure, but have limited sensitivity and lack conventional sonographic characteristics in symptomatic patients. Shear wave ultrasound elastography quantitatively assesses tissue stiffness.
Objectives. To compare the diagnostic accuracy of shear wave ultrasound elastography to that of standard ultrasound (combined B-mode grayscale sonography and power Doppler) for diagnosis of achillotendinopathy, considering clinical symptoms as the reference standard.
Materials and methods. Standard questionnaires regarding medical history and the Chinese version of a Victorian Institute of Sports Assessment – Achilles Questionnaires (VISA-AC) score were evaluated for a total of 14 treatment-naïve patients with complaints of localized swelling, and reduced force and/or flexibility of the Achilles tendon(s). The irregular thickening around the Achilles tendon, heterogeneity of echotexture of the tendon and calcification of the calcaneal attachment were considered incidences of tendinopathy in B-mode grayscale sonography. Tendinopathies were considered if tendons were >0.60 cm thick in power Doppler. Shear wave elasticity <350 kpa (10 m/s) was considered tendinopathy.
Results. A total of 28 conditions of both sides were evaluated through standard ultrasound examinations. Eighty-four tendons were assessed using shear wave ultrasound elastography. Asymptomatic tendons were visible as red and symptomatic (VISA-AC score <80) tendons were visible as blue or turquoise in the images. The rigidity of symptomatic tendons was lower than that of asymptomatic tendons (p < 0.0001). Sensitivity and accuracy for standard ultrasound were increased by the addition of shear wave ultrasound elastography for both symptomatic and asymptomatic tendons. The VISA-AC score was strongly correlated with the elasticity values (p = 0.000, Kendall’s tau-beta (τβ) = 0.71) of Achilles tendons.
Conclusions. Shear wave ultrasound elastography augments diagnostic confidence of standard ultrasound for the treatment of tendinopathies of Achilles tendons.
Key words: power Doppler, Achilles tendon, B-mode grayscale sonography, shear wave ultrasound elastography, tendinopathies
Background
Achilles tendinopathy (achillotendinopathy) is an orthopedic injury reported due to overuse of lower extremity, especially among athletes (overuse disorder) and elderly people (degeneration change of the tendon).1 Achilles tendinopathy leads to chronic tendon pain, chronic tendon injury and/or accumulation of subclinical microdamage.2 To overcome rupture of a tendon, chronic pain and severe injuries of a tendon, and to provide effective treatment, early diagnosis of tendinopathy is necessary.3 Etiology and pathology of Achilles tendinopathy are not fully understood.4 Therefore, it is difficult to choose an appriopriate treatment.
Achillotendinopathy is a huge clinical problem and better diagnostic tools would be beneficial for the follow-up of patients with Achilles tendinopathy. The diagnosis of tendinopathy is not always easy using imaging modalities5 because 3 different muscles contribute to the Achilles tendons.6 The B-mode grayscale sonography and power Doppler are well-established ultrasound techniques, and magnetic resonance imaging (MRI) is used to visualize tendon structure7 because heterogeneous echogenicity or hypoechogenicity and increased tendon thickness correlates with tendon functions.8 However, their utilization in Achilles tendinopathy diagnosis is controversial9 because their sensitivity is limited and Achilles tendinopathy lacks conventional sonographic characters in symptomatic patients.10
Shear wave ultrasound elastography allows to quantitatively assess tissue stiffness, but is used less often in tendinopathy diagnostics. It is well-established for visualization of stiffness of liver,11 breast,12 prostate,13 thyroid,14 shoulder tendons,15 and tongue muscle16 lesions. It is also regarded as a promising tool for the diagnosis of Achilles tendinopathy and patellar tendons in routine clinical practice.17
Objectives
The objectives of the retrospective analysis of a cross-sectional study were to compare the diagnostic accuracy of quantitative shear wave ultrasound elastography to that of a standard ultrasound (combined qualitative B-mode grayscale sonography and quantitative power Doppler) for diagnosis of Achilles tendinopathy in treatment-naïve patients, considering clinical symptoms as the reference standard.
Materials and methods
The designed protocol of the study was approved by the ethics committee of the Chongqing Jiulongpo District Second People’s Hospital (approval No. CJSPH2123 dated April 20, 2020). The study protocol adheres to Chinese law and the 2008 Declaration of Helsinki. All studied patients have signed during hospitalization an informed consent form regarding radiological examinations, biochemical tests and publication of anonymized information in the form of a scientific article (1 or more).
The inclusion criteria were as follows: patients from a diabetes clinic with complaints of pain in the Achilles unilateral or bilateral tendon(s), diffuse or localized swelling, reduced force, and/or reduced flexibility of the unilateral or bilateral tendon(s) in the last 6 months.
Patients who had undergone treatment for their clinical symptoms, like physical therapy or medication (systemic, and/or topical) with nonsteroidal anti-inflammatory drugs, were excluded from analysis because symptoms should persist at the time of ultrasound examinations. Patients with tendon rupture or surgery were also excluded from analysis.
Clinical assessment
Standard questionnaires regarding medical history, sports activity and tendon pain (in rest, movement and pressure) were evaluated for all studied patients before ultrasound examinations were performed by orthopedic surgeons. The Chinese version of a Victorian Institute of Sports Assessment – Achilles Questionnaires (VISA-AC) score was used for the evaluation of pain in tendons.18 The score ranges from 100 to 0, in which 100 means no pain or no impairment in physical activity and 0 means maximum pain or maximum impairment in physical activity. Glycated hemoglobin (%HbA1C), cholesterol, serum triglycerides, fasting blood glucose, and urine albumin levels were evaluated through pathological examinations. Tendons with a VISA-AC score less than 80 were considered symptomatic.3
Ultrasound examinations
All studied patients underwent a bilateral multimodal ultrasound that included B-mode grayscale sonography, power Doppler ultrasound and shear wave ultrasound elastography. Aixplorer (SuperSonic Imagine, Aix-en-Provence, France) ultrasound equipment with 15 MHz linear transducer (SuperLinear SL15-4; SuperSonic Imagine) and 256 bandwidths from a 5–14 MHz range were used. Wall filter, alias threshold and other standardized setting parameters were the same in all studied patients. A gel (Sonogel®; Sonogel Vertriebs GmbH, Bad Camberg, Germany), a cushion delay block (length: 100 × 100 mm) and a 20 mm delay distance between transducer and skin were used to improve docking. All ultrasound examinations were performed by radiologists (blinded to the patients’ symptoms) with minimum 5 years of experience.
The Achilles tendons were examined in a relaxed state, in prone position, with foot hanging freely beyond the examination couch.
Standard ultrasound examination
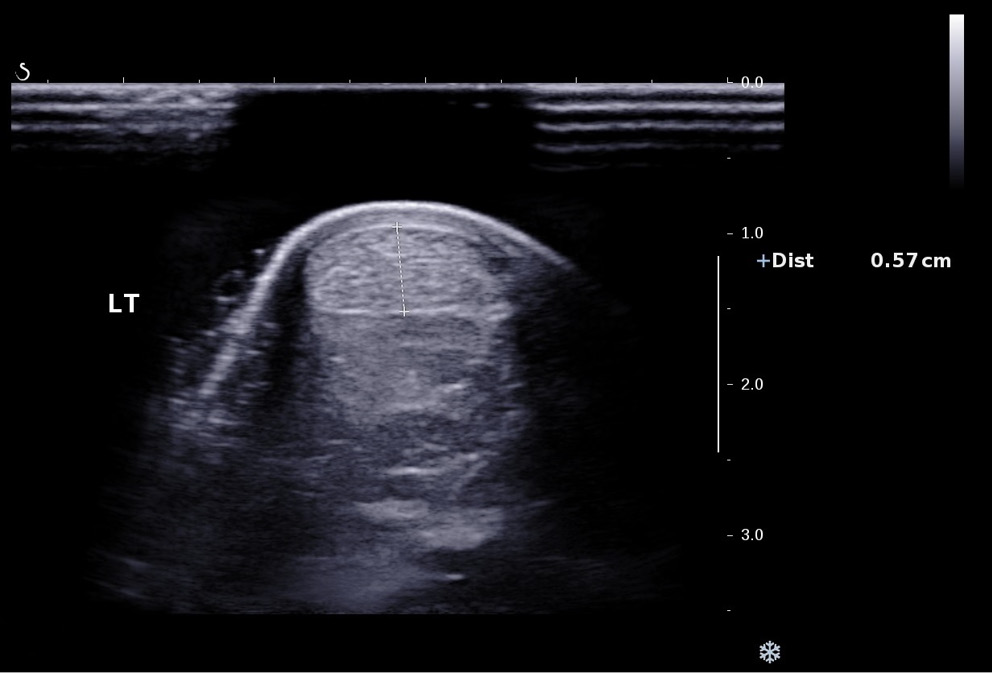
B-mode grayscale sonography in the longitudinal and axial planes was performed. Conditions of the area around the left and right Achilles tendons were evaluated. The irregular thickening around the Achilles tendon, heterogeneity of echotexture of the tendon and calcification of the calcaneal attachment were considered incidences of tendinopathy.3 Then, power Doppler of the whole tendons was performed, and the thickness of the left and right Achilles tendons was evaluated. Achilles tendinopathy was considered if tendons were more than 0.60 cm thick.19 The representative image for power Doppler of the tendon is presented in Figure 1.
Shear wave ultrasound elastography
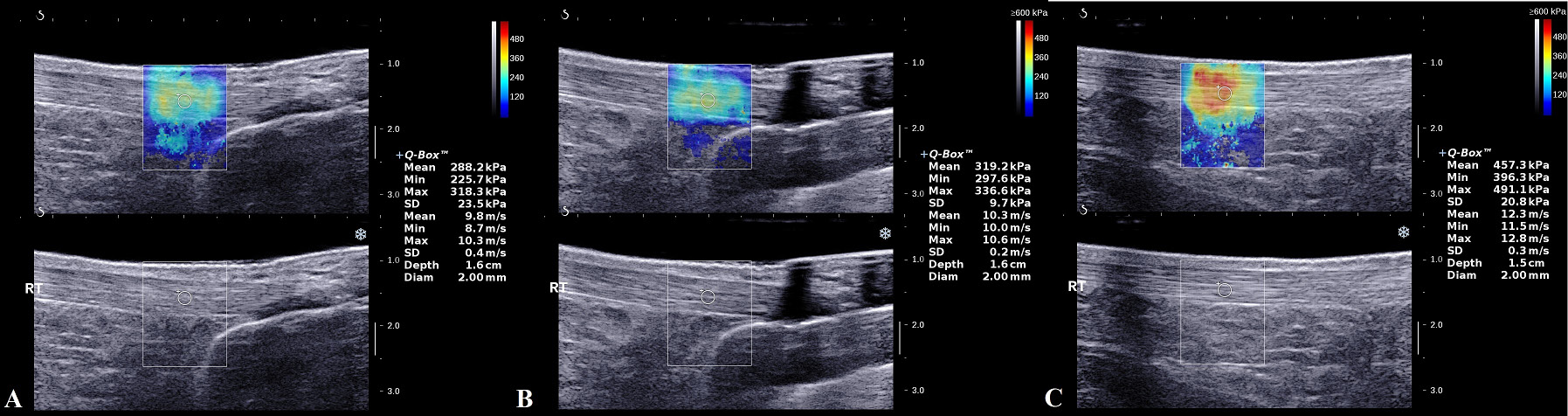
Shear wave ultrasound elastography was performed for the upper left Achilles tendon, middle left Achilles tendon, lower left Achilles tendon, upper right Achilles tendon, middle right Achilles tendon, and lower right Achilles tendon. It was performed for the most suspicious area detected with the B-mode grayscale sonography. The results were analyzed based on color images (semi-quantitatively) and by rigidity of tissue in the region of interest (ROI; quantitatively). The meaning of the colors is: blue – low rigidity, turquoise – intermediate rigidity, yellow to red – high rigidity. The Young’s modulus was used for a quantitative assessment of shear wave ultrasound elastography. The maximum speed of the shear wave was 500 kPa/13 m/s with 2 cm depth. In the ROI, mean and maximum rigidity and shear wave speed were evaluated. A total of 2 mm was the standard diameter of the ROI.3 The representative images for B-mode grayscale sonography and shear wave ultrasound elastography are presented in Figure 2. The characteristics of the most auspicious area in the B-mode grayscale sonography were: the irregular thickening around the Achilles tendon, heterogeneity of echotexture of the tendon and calcification of the calcaneal attachment. Shear wave elasticity less than 350 kpa (10 m/s) was considered tendinopathy.
Beneficial score analysis
Working area for treatment of tendinopathy was decided based on Equation20:
where
TPdet – true positive tendinopathy detected;
FNdet – false negative tendinopathy detected;
Tnumb – total number of tendons evaluated;
LDC – level of diagnostic confidence above which treatment for tendinopathy can be initiated or continued.
Diagnostic parameters
Sensitivity and accuracy were evaluated as in Equations:
,
where
TP – true positive tendinopathy;
FN – false negative tendinopathy;
TN – true negative tendinopathy;
Tnumb – total number of tendons evaluated.
Statistical analyses
The IBM SPSS v. 26.0 software (IBM Corp., Armonk, USA) was used for statistical analyses. The Mann–Whitney test was performed for continuous data. The Fisher’s exact test was used for categorical data. The Kendall’s tau-beta correlation was developed between VISA-AC score and the ultrasound characteristics of Achilles tendons at 95% confidence interval (95% CI). The Kendall’s tau-beta correlation coefficient (τβ) was interpreted as: 0 – no correlation, 0.1–0.39 – weak correlation, 0.4–0.69 – moderate correlation, 0.7–0.89 – strong correlation, and ≥0.9 – perfect correlation.21 All results were considered significant if the p-value was less than 0.05.
Results
Study population
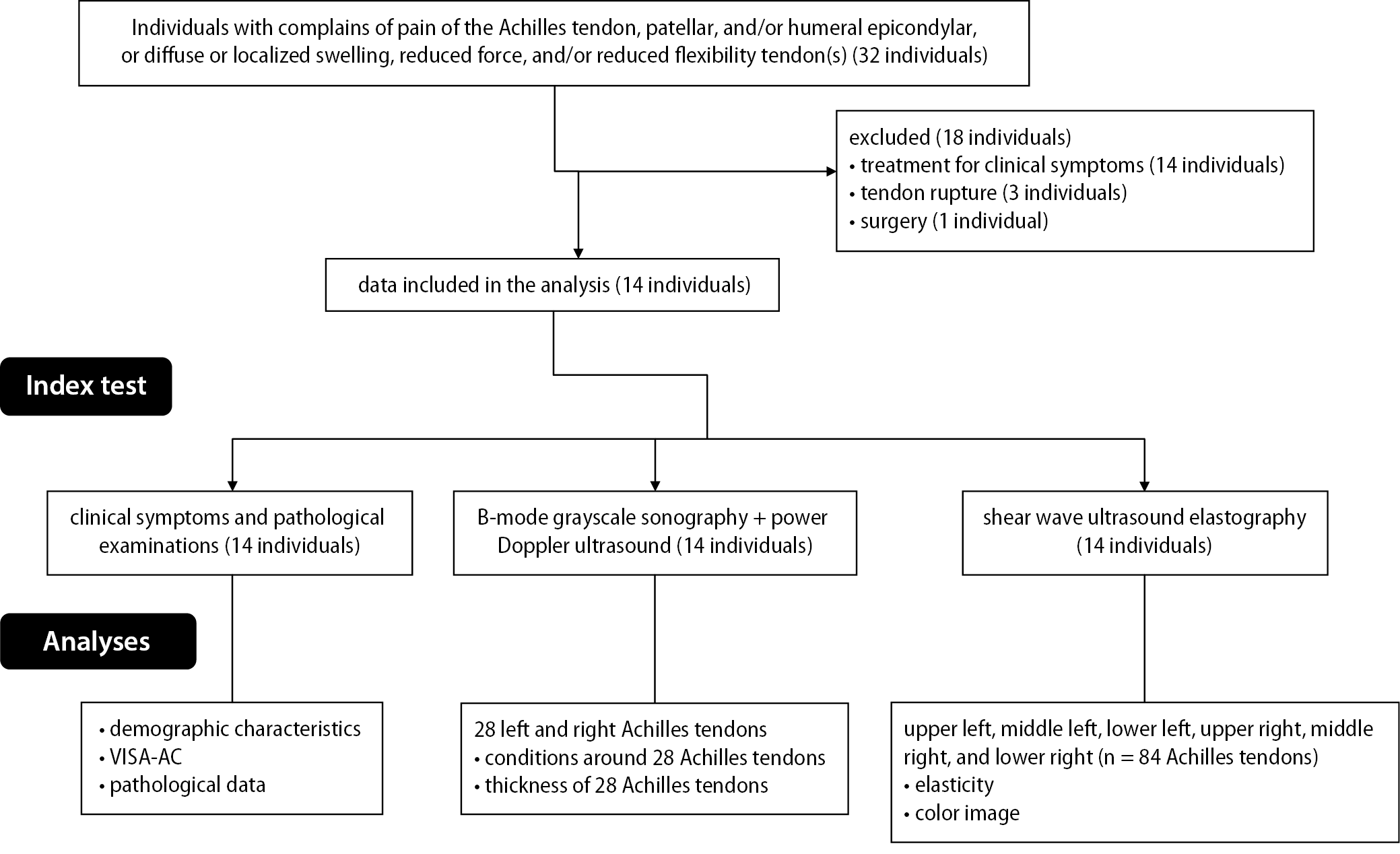
From April 21, 2020 to May 1, 2021, 32 individuals with complaints of pain, diffuse or localized swelling, reduced force, and/or reduced flexibility of the Achilles tendon(s) were enrolled at the Department of Orthopedics of the Chongqing Jiulongpo District Second People’s Hospital, Chongqing, China, and the Chongqing Red Cross Hospital, People´s Hospital of Jiangbei District, Chongqing, China. Among them, 14 patients had undergone treatment for their clinical symptoms, 3 patients had tendon rupture and 1 patient had undergone surgery. Therefore, data of these patients (n = 18) were not included in the analysis. Data on clinical symptoms, pathological examinations, B-mode grayscale sonography, power Doppler ultrasound, and shear wave ultrasound elastography of 14 patients were retrospectively included in the analysis after obtaining written approval from the respective institutions, as it was a retrospective study. The flow diagram of retrospective analysis of the study is presented in Figure 3.
Clinical symptoms
Clinical symptoms of 14 patients were analyzed. The details of their clinical symptoms are presented in Table 1. Among these 14 patients, 4 had bilateral tendons and 10 had unilateral tendons. A total of 84 tendons were analyzed. Among them, 11 (13%) were symptomatic and 73 (87%) were asymptomatic.
Standard ultrasound examination
Standard ultrasound examination was performed at left and right Achilles tendons. A total of 28 conditions (left and right) were evaluated using standard ultrasound examination and 14 (50%) of them were reported as tendinopathies. The remaining 14 conditions were diagnosed using ultrasound as asymptomatic.
Shear wave ultrasound elastography
Asymptomatic tendons were visible as red (high rigidity) and symptomatic tendons as blue (low rigidity) or turquoise (intermediate rigidity) images. Tendon rigidity of symptomatic tendons were lower than that of asymptomatic tendons. Shear wave ultrasound elastography results for Achilles tendons was reported in Table 2. According to these measurements, 39 (46%) out of 84 tendons had tendinopathies. Among them, 29 (34%) were asymptomatic and 10 (12%) were symptomatic. The elasticity values of the symptomatic tendons were lower than those of the asymptomatic ones (p = 0.044, Mann–Whitney test).
Correlation between pain symptoms and ultrasound examinations
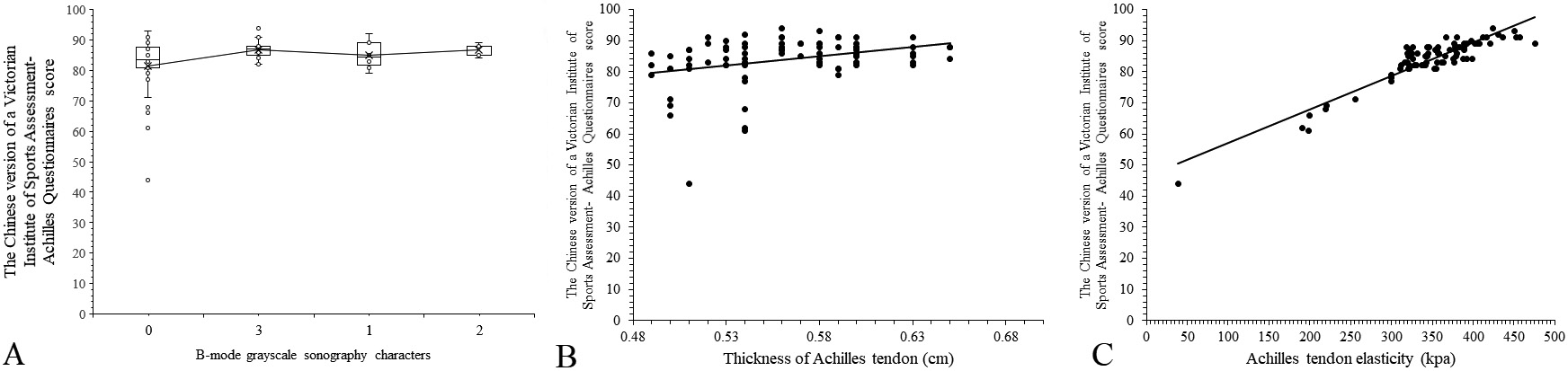
The VISA-AC score had weak correlation with standard ultrasound characteristics (τβ = 0.31, degrees of freedom (df) = 83, p = 0.5467) and with power Doppler characteristics (τβ = 0.38, df = 83, p = 0.1051) of Achilles tendons, but that was strongly correlated with the elasticity values (p = 0.0001, df = 83, τβ = 0.71) of Achilles tendons. The details of the correlation between pain symptoms and ultrasound examinations are reported in Figure 4.
Diagnostic parameters
All studied patients had mild to moderate complaints about each tendon, and therefore, tendinopathy was clinically considered in all tendons. Sensitivity for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for symptomatic tendons were 0, 1 and 1, respectively. Accuracy for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for symptomatic tendons were 0, 1 and 1, respectively. Sensitivity for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for asymptomatic tendons was 0.58, 0.38 and 0.78, respectively. Accuracy for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for asymptomatic tendons was 0.58, 0.38 and 0.78, respectively. Sensitivity for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for all Achilles tendons (symptomatic and asymptomatic) was 0.5, 0.46 and 0.81, respectively. Accuracy for standard ultrasound, shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography for all Achilles tendons (symptomatic and asymptomatic) was 0.5, 0.46 and 0.81, respectively. The details of diagnostic parameters for index tests are reported in Table 3.
Beneficial score analysis
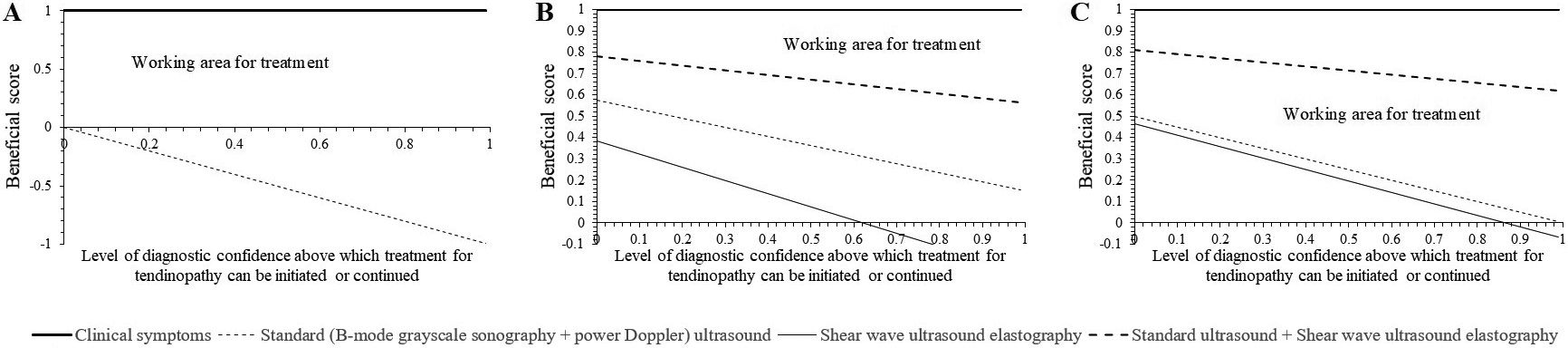
Working areas for the treatment of tendinopathies of symptomatic Achilles tendons for shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography were 0–1 diagnostic confidence/tendon (Figure 5A). Working areas for the treatment of tendinopathy of asymptomatic Achilles tendons for standard ultrasound (B-mode grayscale sonography + power Doppler), shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography were 0–1 diagnostic confidence/tendon, 0–0.61 diagnostic confidence/tendon and 0–1 diagnostic confidence/tendon, respectively (Figure 5B). Working areas for the treatment of Achilles tendinopathy of all Achilles tendons (symptomatic plus asymptomatic) for standard ultrasound (B-mode grayscale sonography + power Doppler), shear wave ultrasound elastography and standard ultrasound plus shear wave ultrasound elastography were 0–0.98 diagnostic confidence/tendon, 0–0.86 diagnostic confidence/tendon and 0–1 diagnostic confidence/tendon, respectively (Figure 5C).
Discussion
The study found that sensitivity and accuracy for standard ultrasound plus shear wave ultrasound elastography were higher for both symptomatic and asymptomatic tendons than those of standard ultrasound. The results of the measurements of diagnostic parameters of the current study are consistent with those of a prospective study3 and a cross-sectional study,17 but are not consistent with that of another prospective study.5 Different study populations are the probable reason for contradictory results. There is a noticeable change in shear wave elasticity values between healthy and diseased tendon(s).9 Shear wave ultrasound elastography augments diagnostic confidence for treatment of Achilles tendinopathy.
A study by Visnes et al. reported that standard ultrasound had a higher rate of false negative findings. Also, shear wave ultrasound elastography is not yet standardized to the level of elimination of false negative cases. In clinically symptomatic patients, standard ultrasound often cannot find sonographic features.10 Also, inter-observer correlation is an issue for qualitative evaluations of standard ultrasound,22 while shear wave ultrasound elastography provides quantitative information, which has lower inter-observers’ variabilities.3 The B-mode grayscale sonography and power Doppler provide limited information on Achilles tendinopathy.
In the present study, the results demonstrated that the pain is strongly correlated to the elasticity of the Achilles tendon but weakly correlated with standard ultrasound. The detected correlations between VISA-AC score and imaging parameters of Achilles tendons of the current study are consistent with those presented in prospective studies3, 5, 23 and a cross-sectional study.17 Tendon degradation occurs due to loss of fiber, which causes the softening of Achilles tendons, and consequently the patient feels pain.9 It is possible to use elasticity as an index to evaluate the pain degree of the patient.
This study found that the elasticity values of symptomatic Achilles tendons were lower than those of the asymptomatic ones. The elasticity values measured in the current study are consistent with a prospective study.3 The possible reasons for parallel results are that the comparisons of the elasticity values of symptomatic and asymptomatic tendons in the current study were performed for individuals in the full age range (28–65 years). The prospective study3 was also performed for individuals in a full age range (mean ± standard deviation (SD) 42 ±13.4 years, range: 20–71 years).3 The close correlation between the elasticity values of Achilles tendons and clinical symptoms is less pronounced in elderly individuals.3 The tissue rigidity of Achilles tendons is correlated with clinical symptoms in treatment-naïve patients.
Working areas for the treatment of Achilles tendinopathy for standard ultrasound plus shear wave ultrasound elastography were equal to that of clinical symptoms for symptomatic and asymptomatic tendons. Shear wave ultrasound elastography with standard ultrasound can be useful for initiation of treatment for Achilles tendinopathy or monitoring treatment for the same.
In the article, the 3 parts of the tendons assessed using shear wave elastography are considered as 3 different tendons and 14 tendons with both sides are finally considered as 84 tendons. The possible justification is that the elasticity of different parts and sides of tendons are dissimilar and not correlated with each other. Therefore, it is possible to consider the parts of the tendons as different tendons.
Limitations
The main limitation of this study is that it is a retrospective analysis and not a prospective study. A small sample size (only 14 study patients with 18 painful tendons) led to the type I error. Inter- and intraobserver variabilities were not evaluated (the study was performed by several doctors and the standardization of the study was not performed). The patients’ degree of pain was used as the gold standard. However, patients can have symptoms referable to the Achilles tendon but it does not necessarily mean that the patient has Achilles tendinopathy. Pathological diagnostic tests can also be used for diagnosis of tendinopathy and the patient may be asymptomatic early on.
Conclusions
Shear wave ultrasound elastography augments diagnostic confidence for treatment of Achilles tendinopathy. The B-mode grayscale sonography and power Doppler provide limited information for Achilles tendinopathy. The elasticity values of Achilles tendons are correlated with pain. Shear wave ultrasound elastography with standard ultrasound can be useful for initiation or monitoring of treatment of Achilles tendinopathy.