Abstract
Background. The miR-21 has been implicated in the process of neuroinflammation as well as neuropathic pain.
Objectives. To explore the relationship between the plasma and local expression of miR-21 with disease severity of lumbar disc herniation (LDH) patients with sciatic pain.
Materials and methods. Ninety-two LDH patients with sciatic pain and 25 scoliosis patients as painless controls were enrolled in the current study. Samples from nucleus pulposus (NP), annulus fibrosus (AF) and soft tissues around nerve root (STANR) were obtained. The plasma and local expressions of miR-21 were detected with quantitative reverse transcription polymerase chain reaction (qRT-PCR). The visual analogue scale (VAS) for lumbar pain and leg pain, and Japanese Orthopedic Association (JOA) score were selected to evaluate the clinical severity. The degree of disc compression on nerve was evaluated using the Pfirrmann grade based on the magnetic resonance imaging (MRI) findings. For the convenience of analysis, LDH patients with sciatic pain were classified into a severe pain (SP) group (VAS ≥ 6) and a mild-moderate pain (MP) group (VAS < 6). Receiver operating characteristic (ROC) curve analysis was performed to detect the potential diagnostic power of miR-21 with regard to the Pfirrmann grade.
Results. There were no significant differences in serum miR-21 expressions among SP LDH patients, MP LDH patients and scoliosis painless controls. Local expressions of miR-21 in STANR, AF and NP were all drastically upregulated in the SP group in comparison with the MP group and scoliosis painless group. Local NP and STANR miR-21 expressions were positively associated with the Pfirrmann grade. Local miR-21 expressions in STANR and AF were positively associated with VAS score and negatively related to JOA score. The ROC curve analysis indicated that both STANR and AF miR-21 expressions may serve as significant diagnostic factors for the Pfirrmann grade.
Conclusions. Increased local miR-21 expressions are linked with clinical severity of LDH in patients with sciatic pain.
Key words: miR-21, lumbar disc herniation, sciatic pain, clinical severity
Background
Among the degenerative abnormalities of the lumbar spine, lumbar disc herniation (LDH) has been the most common diagnosis and reason for spinal surgeries in adults.1 Around 2–3% of the world population was affected by LDH, bringing great social and economic burden as well as experiencing impaired life quality. The prevalence of LDH was 4.8% in men and 2.5% in women over 35 years of age.2 Sciatica is the most important symptom of LDH. It causes radiating leg pain that follows a dermatomal pattern, along with the distribution of sciatic nerve into the foot and toes.3 Coughing can make the pain worse, and patients may experience a variety of symptoms such as sensory symptoms, gait deformity, unilateral spasm of the paraspinal muscles, as well as limited forward flexion of the lumbar spine.4
So far, it has been acknowledged that sciatica in the LDH was a direct result of nerve root compression. Nevertheless, LDH has different mechanisms which were hard to be simply explained by mechanical compromise.5 In recent years, studies have demonstrated the biological activity of the herniated tissue in the expression of inflammatory mediators.6 Besides, it has been shown that the protruded nucleus pulposus (NP)-induced neuroinflammatory response was pivotal for radicular pain.7 Neuroinflammation, due to periphery-to-central nervous system (CNS) cross-talk through proinflammatory mediators, could result in chronic pain in LDH patients.8 The herniated NP also resulted in the autoimmune-mediated inflammatory response, involving multiple cytokines, such as tumor necrosis factor alpha (TNF-α) and interleukin (IL)-6.9
As a class of small non-coding RNAs, microRNAs (miRNAs) play critical roles in regulating gene expression and essential physiological and pathological processes. Even though they represent just 1–3% of the human genome, it has been found that miRNAs have the ability to regulate around 30% of the protein-encoding genes in humans.10, 11, 12 Recent works have shown that miRNAs could promote or suppress the inflammatory process, and either exacerbate or attenuate the pathological results of uncontrolled neuroinflammation.13 For example, miR-210 could induce microglial activation and regulate microglia-mediated neuroinflammation in neonatal hypoxic-ischemic encephalopathy.14 The miR-146a negatively regulates neuroinflammation in neurons, microglia and astrocytes.15 The miR-124 acts as a key negative regulator of neuroinflammation by reducing inflammatory mediators and restricting microglia to an inactive state.16 Studies found that the maladjustment of miRNAs expressions is related to the occurrence and development of LDH and sciatica. For example, miR-223 in exosome-like vesicles is related to a decreased risk of persistent pain in LDH patients.17 Increased circulating miR-17 expressions are correlated with the intensity of lumbar radicular pain (LRP) in LDH patients.18 The miR-124-3p could alleviate neuropathic pain in a chronic sciatic nerve injury model.19
The miR-21 is one of the most widely studied miRNAs and is highly present in many cell types. The miR-21 expression is also upregulated in many disease status including cancer, cardiovascular disease, inflamed tissue, etc.20 In active immune cells, including macrophages, neutrophils, mast cells, as well as T cells, miR-21 is highly expressed.20 In the injured dorsal root ganglion (DRG) neurons, miR-21 is specifically upregulated and causally involved in the late phase of neuropathic pain.21 It has been also demonstrated that the delivery of miR-21 derived from neurons to macrophages polarizes these cells into a proinflammatory or pronociceptive phenotype.22 In addition, silencing miR-21 expression in sensory neurons could prevent both the development of neuropathic allodynia as well as the macrophage recruitment in the DRG.22 As a fibrosis-associated miRNA, miR-21 promotes the inflammation in ligamentum flavum tissues by the activation of IL-6 expression, leading to ligamentum flavum fibrosis, hypertrophy and final spinal canal stenosis.23 These findings implicate that miR-21 may play an important role in lumbar-related disease. On the other hand, the rupture of the annulus fibrosus (AF) can lead to a foreign body reaction resulting from NP that guides neovascularization,24 which is accompanied by macrophage infiltration. The subsequent macrophage infiltration is believed to aggravate pain symptoms and sciatica through the production of various cytokines.25 In contrast, macrophage infiltration may also have a positive effect on relieving symptoms through inducing a phagocytic resorption process, mediated by anti-inflammatory cytokines.26 Previous studies found that miR-21 could promote macrophage infiltration under various conditions.27, 28
Objectives
All the abovementioned studies indicated that miR-21 may serve as an important promoter for facilitating the sciatica in LDH patients. However, there were no studies illustrating the relationship between miR-21 expression and LDH severity. Therefore, this study was designed to detect whether circulating or local miR-21 expressions are related to the clinical severity of LDH patients with sciatica.
Materials and methods
Study patients
From May 2020 to May 2021, 92 LDH patients who received discectomy were enrolled in the study. All LDHs were confirmed with magnetic resonance imaging (MRI) with unilateral sciatica, regardless of lumbar pain existence. Inclusion criteria were determined as follows: 1) definite lower level and single segment (L4~L5 or L5~S1) disc herniation on MRI, consistent with related clinical signs, as well as symptoms of LRP (straight leg raising (SLR) < 60°) with either a short-term (2–4 weeks) severe or long-term (4–12 weeks) moderate leg pain; 2) patients did not receive nonsteroidal anti-inflammatory drugs (NSAIDs) or nerve nutrition drugs for at least 1 week before the surgery. Exclusion criteria were as follows: 1) patients with serious functional diseases in multiple organs, including the heart, lung, liver, kidney, etc.; 2) patients with blood system diseases, cancer or other systemic diseases; 3) patients with incarcerated, central, free, or giant LDH; 4) patients with foot drop or cauda equina syndrome; 5) patients with spondylolisthesis or spinal stenosis. At the same time, 25 scoliosis patients, without any signs of lumbar and radicular pain or degenerative disc disease were recruited as controls. All the controls did not have any signs of LDH identified using MRI. This study protocol was approved by the ethics committee of Maoming People’s Hospital and conducted according to the Declaration of Helsinki. Patients provided an informed consent before any study-specific procedures were performed.
Laboratory examination
Venous blood was extracted from all participants before 9 AM after an overnight fast, and placed at room temperature for 2 h, followed by centrifugation for 20 min at 1900 × g. The miRNeasy Serum/Plasma Kit (Qiagen, Hilden, Germany) was used to isolate the total RNA from 200 μL of serum, according to the manufacturer’s instructions. Up to the present, there was no housekeeping miRNA available that is normalized for the miRNA expression in serum/plasma. Hence, the samples were treated with U6 RNA (5 nmol/L) as the spiked-in RNA, after the addition of miRNeasy.
For tissue examination, total RNA was extracted from NP, AF and soft tissues around nerve root (STANR) using a Trizol kit (Thermo Fisher Scientific, Waltham, USA). The extracted RNA was then reversely transcribed into complementary DNA (cDNA), using PrimeScript™ II 1st Strand cDNA Synthesis Kit (TaKaRa Bio Inc., Kusatsu, Japan). The relative expression of miR-21 was determined using a TaqMan™ MicroRNA Assay (GeneCopoeia, Guangzhou, China) and SYBR® Premix Ex Taq™ kit (TaKaRa Bio Inc.). The fold change relative to internal reference was computed based on the relative quantitative 2−ΔΔCt method: ΔΔCt = ΔCt (target gene) − ΔCt (internal reference). The U6 was adopted as an internal reference of miR-21. The primers were listed as below: miR-21 forward primer: 5’-GTGCAGGGTCCGAGGT-3’, reverse primer: 5’-GCCGCTAGCTTATCAGACTGATGT-3’; U6 forward primer: 5’-CTCGCTTCGGCAGCACA-3’, reverse primer: 5’-AACGCTTCACGAATTTGCGT-3’.
Definition of compression degree
According to the Pfirrmann grade,29 the compression degree was evaluated through an axial cut MR image at the level of maximal disc herniation, to grade the unilateral traversing nerve root compromise due to the herniating disc: grade 0 (normal) – no compromise of the root is seen; grade 1 (contact) – there is a visible contact of disc material with the nerve root, and the normal epidural fat layer between the two is not evident, while the nerve root has a normal position and there is no dorsal deviation; grade 2 (deviation) – the nerve root is displaced dorsally by disc material; grade 3 (compression) – the nerve root is compressed between disc material and the wall of the spinal canal (it may appear flattened or be indistinguishable from the disc material). Only patients with Pfirrmann grade ≥1 were enrolled in the study. The image findings were assessed by 2 experienced radiologists, and the kappa value was computed to examine the consistency of the results. As recommended by Landis and Koch,30 the kappa value was graded as following: 0–0.20: slight agreement; 0.21–0.40: fair agreement; 0.41–0.60: moderate agreement; 0.61–0.80: substantial agreement; 0.81 or higher: excellent agreement; 1.00: absolute agreement.
Assessment of clinical severity
The degree of pain was determined using the visual analogue scale (VAS) score, whereas the functional ability was determined with Japanese Orthopedic Association (JOA) score. The VAS scale was presented as a line segment with a length of 10 cm, representing 10 points in total (1 cm for 1 point): 0 points indicates no pain and 10 points indicates an extremely severe pain. The higher the score, the more severe the pain.31 Since the number of cases in our study was comparatively small, the median number of 0–10, 5.5 (rounding up to 6) was used to categorize the severity of pain. Besides, lumbar pain, numbness or pain of lower limbs, SLR test, walking ability, esthesia, activities of daily living (ADL), muscle strength, as well as bladder function were all assessed using JOA score. The score of JOA ranges from 0 to 29 points, where higher scores indicate less pain and better function.32 Both VAS and JOA scores are widely used in the evaluation of pain and function states in many diseases.
Statistical analyses
Statistical analyses were carried out using IBM SPSS v. 21.0 software (IBM Corp., Armonk, USA). The statistical graph was created using Prism 8.0 (GraphPad, San Diego, USA). Data were described as mean ± standard deviation (SD) or median (interquartile range (IQR)). The distribution data of miR-21 expressions was tested using Kolmogorov–Smirnov test. The statistical analysis showed that the data of miR-21 expressions were normally distributed. The Student’s t-test was carried out to compare the differences between the groups. One-way analysis of variance (ANOVA) was applied to statistically test the differences among ≥3 groups, followed by Dunn’s post hoc tests. The Spearman’s correlation analysis was used to examine the association of miR-21 expression with VAS and JOA scores. Area under the curve (AUC) was tested for statistical analysis, with regard to receiver operating characteristic (ROC) curve analysis. The values of p < 0.05 were considered statistically significant.
Results
Demographic data
There were significant differences in age (p < 0.001). Besides, there were no significant differences in disease duration between severe pain (SP) and mild-moderate pain (MP) groups (median 6.3 compared to 6.0, p > 0.05). Demographic characteristics are listed in Table 1.
Serum and local miR-21 expressions
in LDH patients and controls
Based on the degree of pain, LDH patients with sciatica were divided into the SP group (VAS ≥ 6; n = 44) and the MP group (VAS < 6; n = 48). Additionally, 25 scoliosis patients without pain were enrolled as painless controls. No significant differences of serum miR-21 expressions were found between control and LDH patients (1.00 ±0.04 compared to 1.00 ±0.06, t = 0.936, p = 0.404; Table 2). Also, no significant differences of serum miR-21 expressions were found between the MP group and SP group when Student’s t-test was used (1.00 ±0.05 compared to 1.00 ±0.06, t = 0.942; p = 0.399; Table 3). Compared to the controls, miR-21 expressions in NP, STANR and AF were all significantly higher in the LDH group (t = 9.58, 2.58 ±0.87 compared to 0.99 ±0.06, p < 0.001, t = 9.136, t = 13.16, all p < 0.001; Table 2). Subsequently, the local miR-21 expression in the SP as well as the MP groups was further compared. We found that NP (3.25 ±0.40 compared to 1.96 ±0.70, t = 10.700, p < 0.001) as well as STANR (2.75 ±0.61 compared to 2.42 ±0.55, t = 2.776, p = 0.007), but not AF (2.68 ±0.62 compared to 2.49 ±0.58, t = 1.472, p = 0.144) miR-21 expressions were significantly increased in the SP group in comparison with MP group (Table 3).
Correlation between serum/local
miR-21 expressions and Pfirrmann grade in LDH patients
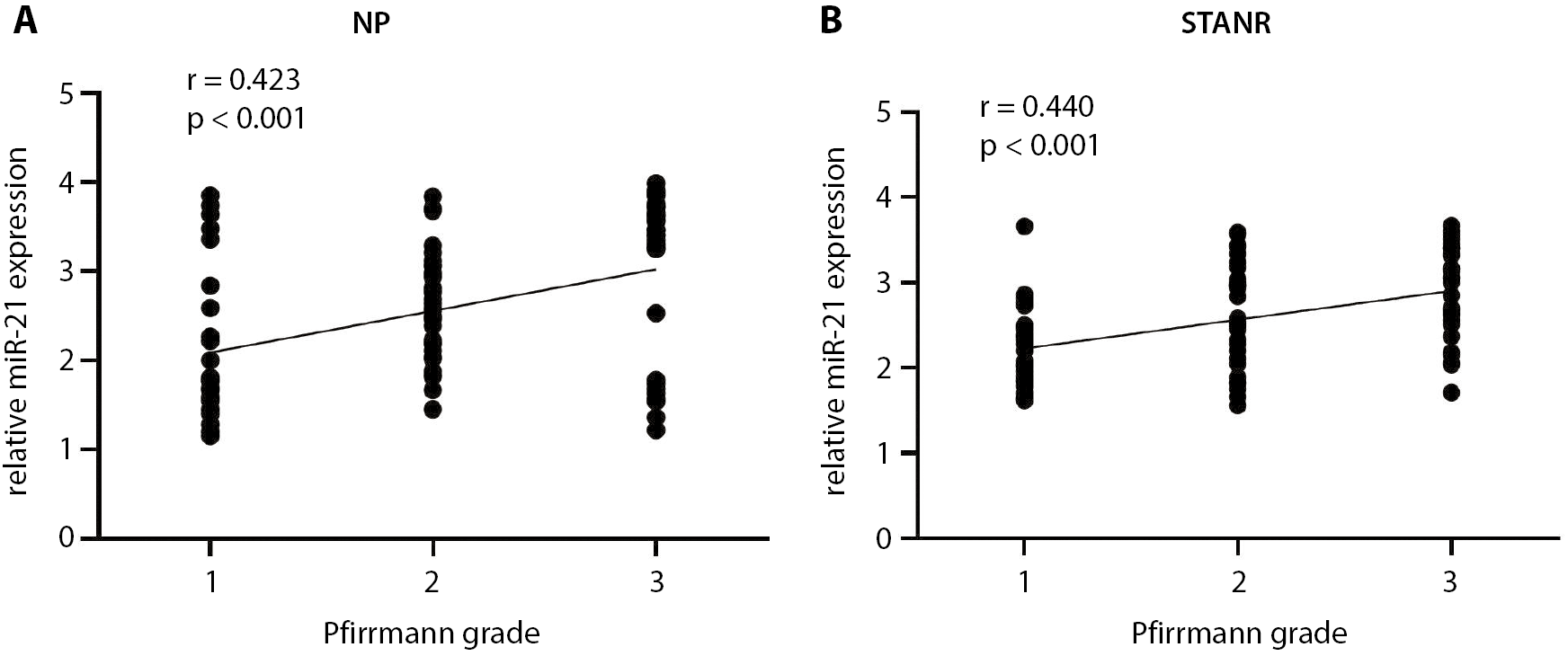
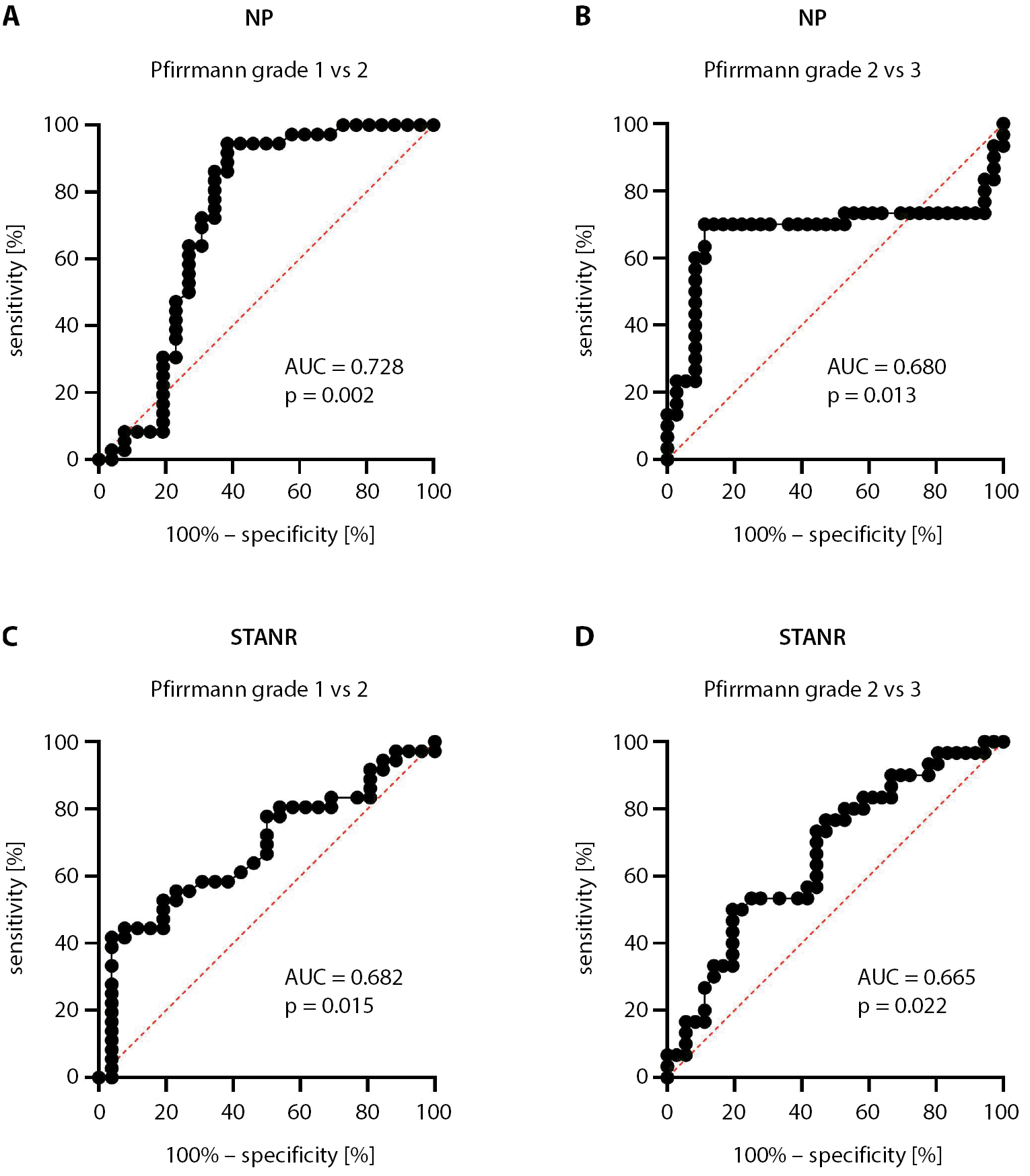
The possible relationship between serum/local miR-21 expressions and compression degree to sciatic nerve was further explored through Pfirrmann grading system. In the LDH patients, there were 26, 36 and 30 patients with Pfirrmann grade 1, 2 and 3, respectively. Through Student’s t analysis, we found that LDH patients with Pfirrmann grade 3 had drastically higher NP and STANR miR-21 expressions than LDH patients with Pfirrmann grade 2 (NP: 2.39 ±0.21 compared to 2.17 ±0.26, t = 2.209, p = 0.031; STANR: 2.90 ±0.54 compared to 2.57 ±0.60, t = 2.316, p = 0.024; Table 4). Furthermore, LDH patients with Pfirrmann grade 2 demonstrated markedly increased NP and STANR miR-21 expressions compared to LDH patients with Pfirrmann grade 1 (NP: 2.17 ±0.26 compared to 2.06 ±0.16, t = 2.844, p = 0.006; STANR: 2.57 ±0.60 compared to 2.22 ±0.48, t = 2.467, p = 0.017; Table 4). The Spearman’s correlation analysis showed that both NP and STANR expressions were positively related to Pfirrmann grade (NP: r = 0.423, p < 0.001; STANR: r = 0.440, p < 0.001; Figure 1A,B). We performed ROC curve analysis to explore the diagnostic value of local miR-21 with regard to Pfirrmann grade. The ROC curve analysis indicated that both NP (Pfirrmann grade 1 compared to 2: AUC = 0.728, p = 0.002; Pfirrmann grade 2 compared to 3: AUC = 0.680, p = 0.013; Figure 2A,B) and STANR (Pfirrmann grade 1 compared to 2: AUC = 0.682, p = 0.015; Pfirrmann grade 2 compared to 3: AUC = 0.665, p = 0.022) miR-21 expressions may serve as significant diagnostic factors for the Pfirrmann grade (Figure 2C,D). However, there were no significant differences in serum miR-21 expressions among different Pfirrmann grades (1–3) detactable with one-way ANOVA (0.98 ±0.06 compared to 1.01 ±0.06 compared to 1.00 ±0.06, respectively, F = 0.387, p = 0.681; Table 4). Besides, serum miR-21 expressions were not significantly associated with Pfirrmann grades (r = 0.107, p = 0.310).
Association of local miR-21 expression levels with VAS and JOA scores
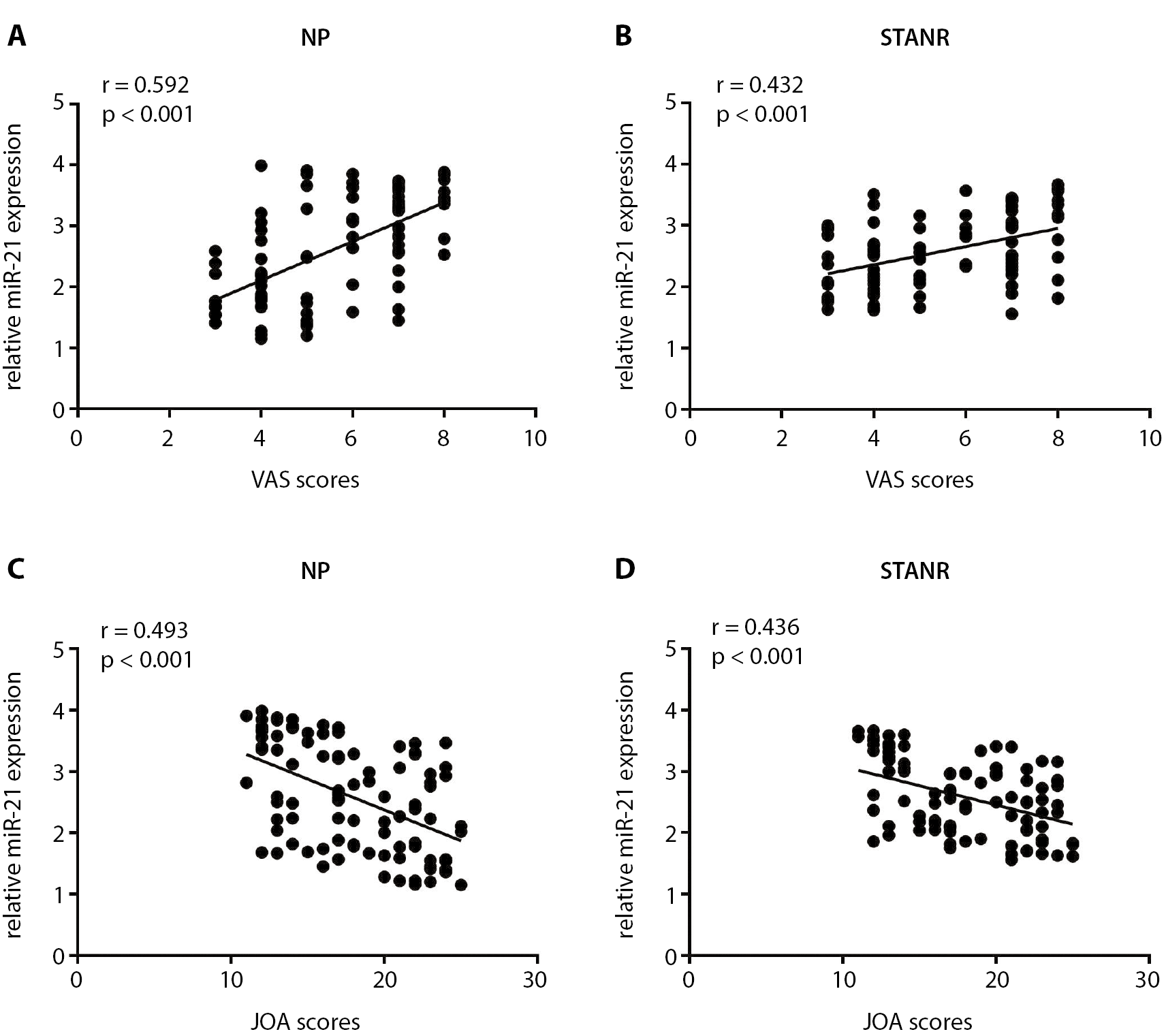
The associations of miR-21 expressions in STANR and NP with VAS and JOA scores were then investigated. The Spearman’s correlation analysis showed that miR-21 expressions in both NP and STANR were positively linked to VAS (NP: r = 0.592, p < 0.001; STANR: r = 0.432, p < 0.001; Figure 3A,B) and negatively associated with JOA scores (NP: r = −0.493, p < 0.001; STANR: r = −0.436, p < 0.001; Figure 3C,D).
Discussion
Lumbar radicular pain was first described by Hippocrates in the 14th century BC.33 Most of the pathophysiologic mechanisms in animal models as well as experimental studies underpinning sciatica have been explored. However, the relevant neoplastic, infectious or degenerative conditions have remained unexplored. In addition to mechanical deformation, the pathophysiologic mechanisms of sciatica may also be related to inflammation, immunology and neurophysiology.
Neuropathic and inflammatory pain promote a large number of persisting adaptations at the cellular and molecular level, allowing even transient tissue or nerve damage to elicit changes in cells that contribute to the development of chronic pain and associated symptoms.34 In recent years, authors who were striving to achieve a consensus of opinion related to the pathogenesis of neuropathic or inflammatory pain, in their works have been devoting increasingly more attention to the importance of an epigenetic component.35 The advances in the basic and clinical sciences over these years have substantiated the belief that neuropathic or inflammatory pain could be partially regulated by epigenetic factors.36 The miRNAs do not only function as one of the most important epigenetic machineries, but also are epigenetically modified by DNA methylation and histone modification like any other protein-coding gene.37
The current study investigated the effect of serum/local miR-21 expression on disease severity in LDH patients with sciatica. We found that local miR-21 expression was significantly higher than in controls, indicating that local miR-21 may take part in the process of sciatica in LDH patients. In this study, we did not observe any significant differences in serum miR-21 expressions between LDH patients and controls, indicating that LDH causing radicular pain is a local event instead of a systematic process. On the other hand, sometimes, microRNA expressions in the serum are not stable and may be affected by many other conditions.
Additionally, we found that local miR-21 levels of NP and STANR were positively linked to VAS score and negatively related to JOA score. As mentioned before, the herniated tissue is not inert but very active in expressing inflammatory mediators. Both the chemical irritation caused by the NP-released bioactive substances and an autoimmune response against itself can also induce the inflammation. We extended these findings and demonstrated that higher local NP and STANR miR-21 expressions in LDH patients are linked to the increased radicular pain.
The following ROC curve analysis showed that both NP and STANR miR-21 expressions may serve as a significant diagnostic factor for the Pfirrmann grade, indicating that the more the disk is herniated, the higher the miR-21 is expressed. The herniated disk tissues also affect the STANR, but not in AF. This may be attributed to the fact that increased miR-21 expressions originate from the degenerated disk. Many researchers focused on the proinflammatory role of NP around the nerve root. As reported in studies, NP had both inflammatogenic and leucotactic effects.38, 39 An animal study also reported that autologous NP applied to the lumbar nerve roots of rats led to a reduced blood flow to the DRG as well as an elevated endoneurial fluid pressure.40 The miR-21 has been implicated to play a role in causing the inflammatory and neuropathic pain in previous studies. Simeoli et al. found that pain neurons in DRG release exosomes containing miR-21 after nerve injuries. These exosomes are then absorbed by the immune cells in the surrounding, further contributing to the local inflammation as well as neuropathic pain.41 Chemokines produced by Schwann cells and satellite cells promote monocyte/macrophage infiltration at the site of injury and DRG. When they blocked the release of miR-21 from the exosomes of DRG pain neurons, they played an anti-inflammatory role and prevented the neuropathic pain in mice.41
Limitations
There were some limitations that should be taken into account. First, the sample size was relatively small. More samples would be needed to identify the findings of our study. Second, we only examined serum and local miR-21 expressions. The investigation of other miRNAs or related inflammatory cytokines may reveal much more valuable information.
Conclusions
We found that local NP and AF miR-21 expressions were significantly upregulated in LDH patients with sciatica compared to controls, and local miR-21 expressions were positively correlated with disease severity of LDH. Local interventions that target miR-21 and its related signaling in LDH patients require further study.