Abstract
Background. Radiofrequency (RF) ablation is a commonly used method of atrial fibrillation (AF) treatment. High-power short-duration (HPSD) ablation has been suggested as a method to reduce procedure times whilst creating safe and lasting lesions. High-power ablation with contact force (CF)-sensing technology catheters might aid in a further improvement of safety whilst generating lasting transmural lesions.
Objectives. We report our experience using lesion size index (LSI)-guided 50 W ablation with a CF-sensing catheter of AF.
Materials and methods. We performed LSI-guided 50 W point-by-point ablation using a CF-sensing catheter (TactiCath). Target LSI at the anterior left atrium (LA) was 5.0 and at the posterior LA it was 4.5.
Results. Altogether, 4641 RF lesions were created in 86 consecutive patients. To reach a mean LSI of 4.9 ±0.01, a mean RF ablation time of 14.3 ±0.1 s was applied with a mean CF of 13.4 ±0.1 g. The RF time per lesion at the anterior wall of LA was 15.9 ±0.2 s, while it was 13 ±0.2 s at the posterior wall of LA. We observed force time integral (FTI) values between 36 g and 310 g. Procedure duration was 107 ±4 min with a RF ablation time of 15.4 ±0.6 min. No audible steam pops occurred. No pericardial effusion was observed. After a 1-year follow-up, no adverse events were reported and 83% of patients had no symptomatic arrhythmia recurrence.
Conclusions. We provide evidence for the safety and efficacy of LSI-guided 50 W ablation using the TactiCath CF-sensing ablation catheter. These data support the use of high-power ablation with CF sensing technology to improve both safety and efficacy.
Key words: atrial fibrillation, high-power ablation, lesion size index, contact force sensing
Background
Generation of transmural lesions for targeted ablation of atrial tachycardia circuits or substrate and pulmonary vein isolation has been proven to be of high clinical value for the treatment of atrial rhythm disorders. Different energy forms are used to create these lesions. Radiofrequency (RF) energy is still the most commonly used energy form. To achieve transmural and lasting lesions, different settings of RF energy have been suggested with different relative contributions of the resistive or conductive heating phase.1
Recently, high-power (≥50 W) short-duration (HPSD) RF ablation with irrigated non-contact force has been shown to be safe while reducing procedure and ablation time, as compared to the traditional lower-power (e.g., 35 W) longer-duration ablation.2, 3 Moreover, lesion width has been suggested to be increased in HPSD as compared to traditional ablation techniques, owing to the fact that a substantial fraction of the ablation time is the resistive heating phase.4
Ablation with contact force (CF)-sensing technology catheters has been linked to enhanced procedural safety and efficacy in traditional ablation settings.5, 6, 7, 8, 9, 10 Lesion size index (LSI) is a multiparametric index introduced to improve lesion formation. It incorporates time, power, CF, and impedance data recorded during RF ablation with CF-sensing technology catheters.11, 12 The LSI-guided high-power ablation with CF-sensing technology catheters might aid in a further improvement of safety while generating lasting transmural lesions.
Objectives
We aim to examine the clinical safety and efficacy of LSI-guided 50 W ablation with CF-sensing catheter in patients with atrial fibrillation (AF).
Materials and methods
Study population
We included all consecutive patients that underwent RF ablation for AF with a LSI-guided 50 W ablation protocol in our clinic. All clinical, imaging and procedural data were recorded. The AF type was categorized as paroxysmal when lasting <1 week, or persistent when lasting >1 week and when electrical cardioversion was performed. The study protocol was approved by the human ethics committee of the Charité-Universistätsmedizin Berlin, Germany (application No. EA2/099/20). The study is in accordance with the Declaration of Helsinki.
Procedure and ablation settings
Prior to ablation procedures, a transesophageal echocardiogram was performed to exclude atrial thrombus formation, and transthoracic echocardiography was used to obtain measures of left atria and left ventricle, as previously described.13 Oral anticoagulation therapy with vitamin K antagonists were continued, targeting an international normalized ratio between 2 and 3. Direct oral anticoagulation was paused on the morning of the procedure and resumed after the procedure.
During ablation, patients were sedated by using boluses of midazolam (3–5 mg) and a continuous infusion of propofol (1.5–4 mg/kg/h). Fluoroscopic guided transseptal puncture was performed and intravenous (i.v.) unfractioned heparin (initial bolus 100 U/kg) was administered with an intraprocedural activated clotting time between 300 s and 400 s. A biplane angiography of the left atrium (LA) was performed in angulations of RAO 30° and LAO 60° prior to ablation.
In all cases, the Abbott Ensite PrecisionTM system (Abbott, St. Paul, USA) was used for 3-D electroanatomic mapping with a single dispersive electrode. A decapolar Abott circular mapping catheter (Inquiry OptimaTM) or the multipolar HD grid catheter (both from Abbott) were used for creating a 3-D map of the atrium and for documenting pulmonary vein (PV) potentials. In all cases, a point-by-point circumferential ablation of PVs was performed.
Lesions were generated using a 3.5-mm open-tip irrigated TactiCath Quartz ablation catheter (Abbott) with the Abbott AgilisTM steerable sheath (Abbott). The TactiCath Quartz ablation catheter utilizes 3 fibers for optical force sensing via infrared laser light.12, 14 It was continuously flushed with 2 mL/min of normal saline solution during mapping. Flush rate was increased to 30 mL/min during ablation with a 1-second pre-flushing period before and 2-second post-flushing period after the ablation. The RF energy was generated using an Ampere RF generator (Abbott) with a maximal temperature of 43°C at 50 W both at the anterior and posterior left atrial wall.
The RF energy delivery was initiated at a stable CF between 10 g and 30 g. In our LSI-guided approach, we terminated RF energy delivery when a target LSI of 5.0 for the anterior LA wall and a target LSI of 4.5 for the posterior LA wall were reached. This conservative ablation approach was chosen to minimize the complication rate. The RF energy delivery for linear lesions was also performed with a LSI-guided 50 W ablation protocol, with a targeted LSI of 5.0 at the anterior LA wall and 4.5 at the posterior LA wall. The target inter-lesion distance was 4 mm.
The LSI is generated from CF, impedance, power, RF duration and, most importantly, in vivo experimental data of lesion generation. The underlying formula is based on an empirical model derived from >3000 lesions in animal models and human tissue.11 It accounts for a time-independent resistive and a time-dependent diffusive heating component (see also Calzolari et al. and Mattia et al.11, 15), and considers the nonlinear lesion formation observed in vivo.
After encircling the veins, entry and exit block were confirmed using an Abbott circular mapping catheter (Inquiry OptimaTM; Abbott) or the multipolar HD grid mapping catheter, by documenting lack of vein potentials and failure of pacing inside the vein.
Study outcomes
For each patient, we recorded the pre-ablation clinical characteristics. For each ablation pulse, we obtained duration of RF application, impedance, power, CF, force time integral (FTI), and LSI. All ablation parameters were analyzed and grouped according to the different atrial regions: left/right upper and lower PV and anterior/posterior LA wall. Furthermore, the rate of acute pulmonary vein isolation (PVI), total RF ablation time, fluoroscopy time, and procedure time (skin-to-skin) were documented. The occurrence of steam pops was noted by the operators. Transthoracic echocardiography was performed after the procedure on the same day to exclude pericardial effusion.
For determination of early recurrence, all measures were taken to obtain electrocardiography (ECG) documentation in case of reported symptoms suggestive of arrhythmia recurrence at the 3- and 12-month follow-up visits. This includes either a 24-hour Holter ECG or a 12-lead ECG at the time of the follow-up visit. Symptomatic patients were classified as recurrences.
Statistical analyses
Continuous variables are shown as mean ± standard deviation (SD). Categorical variables are described as numbers or percentages. A correlation between type of AF (paroxysmal or persistent) and binary variables was analyzed with Pearson’s χ2 test. Comparisons of metric variables between paroxysmal and persistent AF were evaluated with Mann–Whitney U test, thereby accounting for not nominally distributed variables. A value of p < 0.05 was used to indicate statistical significance.
Results
Patient characteristics
A total of 86 patients with symptomatic AF were consecutively included in this study. Patients’ baseline clinical characteristics are given by AF type in Table 1. The mean age in the study group was 66 ±1 years. Mean CHA2DS2-Vasc score was 2.8 ±0.2. Mean LA diameter was 40.4 ±0.8 mm and mean left ventricular ejection fraction (LVEF) was 52 ±1%.
The majority of patients were concomitantly treated with a ß-blocker and inhibitors of the renin-angiotensin-aldosterone system (Table 2). There was no statistically significant difference in baseline characteristics between patients with paroxysmal AF and persistent AF other than statin and ACEi/AT1R use, which was more frequent in patients with persistent AF.
Most patients underwent de novo PVI (59% of all procedures) for persistent or paroxysmal AF. De novo PVI was especially prevalent in paroxysmal AF patients (Table 3). However, there were no statistically significant differences in the ablation strategy.
In the remaining patients, re-isolation of the PVs was performed. Additionally, patients with re-isolation of PVs underwent linear ablation in case of inducible left atrial tachycardias.
Procedural data
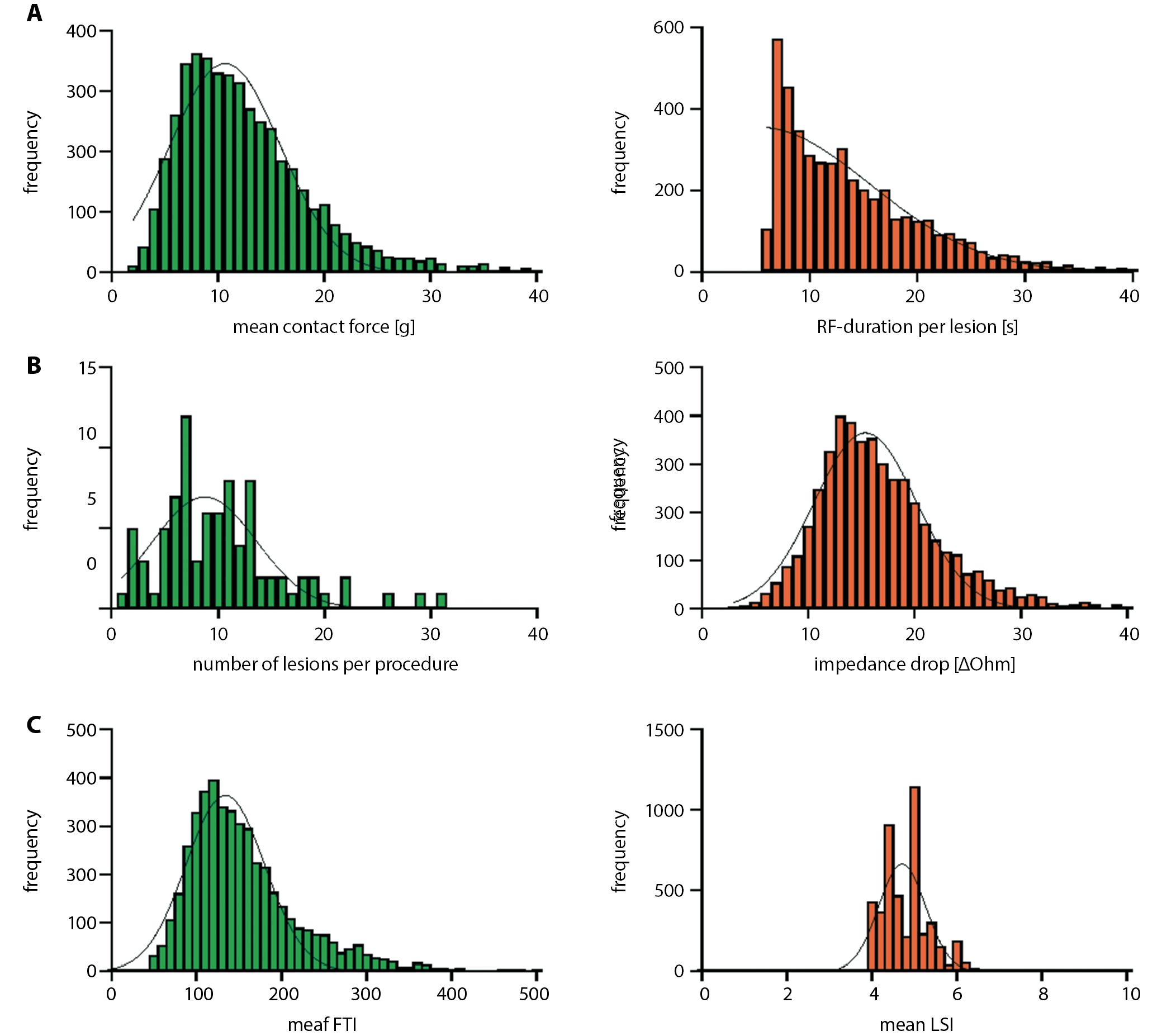
A total of 4641 RF lesions were obtained with an average of 51 ±3 lesions per patient. The LSI-guided 50 W ablation was used for all lesions. Mean procedure duration was 107.7 ±4.8 min (range: 58–187 min), with a mean total RF time of 15.4 ±0.8 min (range: 10.5–39.9 min). Mean RF time per lesion was 14.3 ±0.1 s (range: 6–50 s) and the mean LSI was 4.9 ±0.01 (range: 3.9–6.9; Figure 1).
The PVI or freedom from atrial tachycardia inducibility (in cases of atrial tachycardia) were achieved in all patients without major adverse events.
Mean LSI at the anterior part of the LA was 5 ±0.01. Mean LSI at the posterior part of the LA was 4.6 ±0.01. Mean energy delivery time to reach a LSI of 5.0 was 15.9 ±0.2 s. Mean application time to reach a LSI of 4.5 was 13 ±0.2 s (Figure 2).
The RF duration, FTI and impedance drop showed a continuous increase along with higher LSI ranges. However, most importantly, even high LSI values above 5.5, characterized by RF duration of 17.2 ±1.3 s and a CF of 22.7 ±0.8 g, led to no audible or tactile steam pops or adverse events in any of the 4641 RF applications (Figure 2).
Safety and outcome
Overall, with regard to efficacy and safety, a complete isolation of the pulmonary veins with entry and exit block or freedom from AT inducibility was achieved in all patients without major adverse events. No audible steam pops occurred and no pericardial effusion was observed. Furthermore, in none of the studied patients, a transient ischemic attack or stroke occurred. At 1-year follow-up, no additional adverse events occurred (especially atrio-esophageal fistula, symptomatic pulmonary vein stenosis or phrenic nerve palsy). Freedom from AF or atrial tachycardia was achieved in 83% of all patients.
Discussion
In the present study, we investigated LSI-guided 50 W ablation using TactiCath CF ablation catheter for the treatment of left atrial tachycardia (AF and/or left macroreentrant atrial tachycardia). We determined ablation parameters for different atrial regions and provided catheter- and ablation-related data for different LSI ranges for qualitative and quantitative lesion characterization.
The main finding of this study is that a target LSI of 5.0 at the anterior left atrial wall and 4.5 at the posterior left atrial wall (including left atrial lines) can be safely reached using the TactiCath CF-sensing catheter with an energy delivery of 50 W. With a mean CF of 22.7 ±0.8 g, energy delivery time up to 17 s showed no complications. It was also associated with short procedure times and RF energy delivery, and low risk for arrhythmia recurrences.
The impact of CF catheters and high-power (e.g., >35 W) ablation techniques on long-term outcomes has been studied in several trials.6, 16, 17, 18 In a previous study, the sole use of CF catheters or high-power ablation was associated with a particularly high success rate in patients with paroxysmal AF.19
High-power ablation creates lesions with equal volumes as compared to standard settings; however, they are wider and less deep, most likely due to the increased resistive heating component.20 Previous studies evaluating 50 W ablations using non-CF catheters16, 21, 22 showed a better long-term freedom from AF and shorter fluoroscopy and procedural times without an increase in complication rates, when compared with 35 W ablations using non-CF catheters.2, 3 In our previous experience using 35 W ablation, mean RF application time was 30 min for atrial ablation procedures.23 In the present study, the total RF and procedure times were further decreased as compared to our traditional lower-power (i.e., 30–35 W) ablation approach.
Ablation with a CF-sensing catheter with an appropriate CF has been shown to achieve a higher 1-year freedom from AF when compared with non-CF-sensing ablation catheters.18, 20 Prediction of lesion size is an important aspect of safe and effective RF ablation, especially considering the known variability of myocardial wall thickness. The FTI values above 400 g have been recommended and a wide range of FTI values has been reported for LSI-targeted ablation in a low-power (25–30 W) approach.15 In the present study, we observed FTI values between 36 ±2 and 310 ±15. As reported by Winkle et al.,16 the high variability of FTI makes it an inferior target parameter as compared to LSI guidance. Physicians should be aware that FTI values during high-power ablation may be low despite creating an effective lesion. Traditional FTI cutoffs should be abandoned in high-power ablation.
The LSI has been shown to be a good predictor of lesion size in low-power ablation settings.11, 16 A LSI of 4.5 at the posterior left atrial wall and a LSI of 5.0 at the anterior left atrial wall have been suggested by some studies to predict effective lesion formation.11, 24 Moreover, several animal studies support the use of 50 W ablation using CF catheters for 5–10 s.24, 25, 26
Yet, the appropriate target LSI in high-power ablation using a CF-sensing still needs to be determined. For example, Winkle et al., using a CF-sensing catheter and 50 W ablation strategy as in our study, used a target LSI of 6.0 in patients in AF and a mix of LSI and “loss of pace capture” strategy in patients in sinusrhythm. Their average RF duration per lesion was 11.2 ±3.7 s. As in our study, they could also safely isolate all PVs with short procedure and RF ablation time.16
In our study, to reach an average LSI of 4.9 ±0.01, we needed an average energy delivery time of 14.3 ±0.1 s with a mean CF of 13.6 ±9.1 g. It is important to emphasize that an appropriate CF between 10 g and 30 g appears to be paramount to avoid unnecessary RF energy delivery, which may lead to edema formation, which in turn makes an effective lesion creation at this particular site more difficult or even impossible, thereby increasing the risk for reconnection and arrhythmia recurrence.
Limitations
The main limitation of this study is the consecutive enrolment design and the single-center experience. We did not compare LSI-guided high-power ablation to LSI-guided traditional lower-power (e.g., 35 W) longer-duration ablation protocol. Nevertheless, the study could demonstrate that LSI-guided 50 W ablation proved to be safe, with high acute success rates and short procedure time, whilst also being effective in reducing documented arrhythmia recurrences. As we included both patients with de novo pulmonary vein isolations and patients with redo procedures in our study, we observed an excellent arrhythmia-free survival of 83% during the 1-year follow-up.
Conclusions
We provide evidence for the safety and efficacy of LSI-guided 50 W ablation using the TactiCath CF ablation catheter. We show that a target LSI of up to 5.0 in 50 W ablation strategy is safe and associated with short procedure times and a low symptomatic arrhythmia recurrence rate.