Abstract
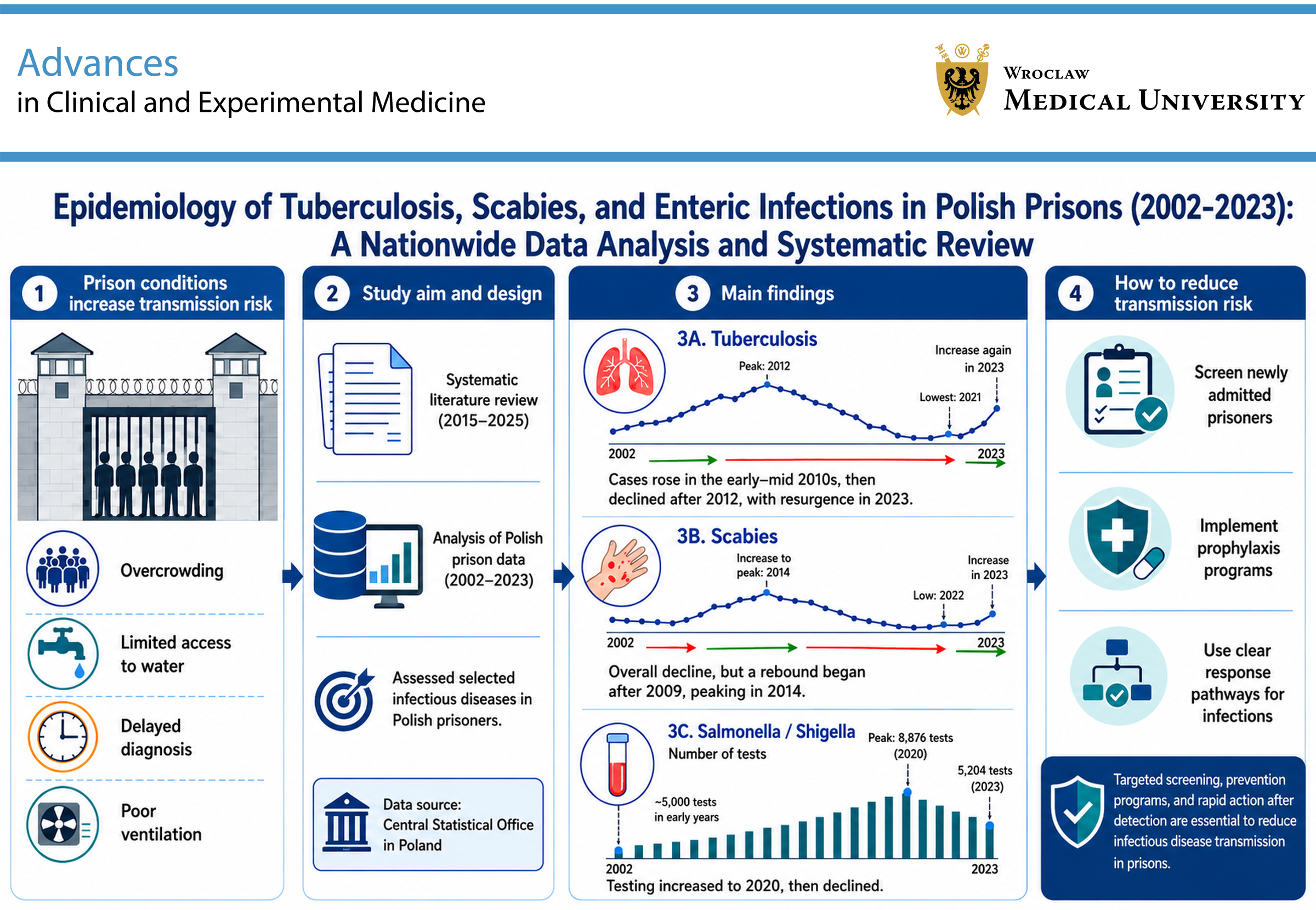
The specific conditions prevailing in prisons increase the risk of disease transmission among inmates. Several factors influence the risk of infectious disease transmission in prisons, including overcrowding, limited access to water, delayed diagnosis, and poor ventilation. The aim of this study was to assess the burden of selected infectious diseases among Polish prisoners between 2002 and 2023 and to analyze the literature addressing these diseases published between 2015 and 2025. In the 1st part, a systematic review was conducted. In the 2nd part, the results of the authors’ own research were presented. The source material was obtained from Statistics Poland. An increase in tuberculosis (TB) cases was observed from the early to mid-2010s, peaking in 2012. Subsequently, a decrease in TB cases was noted after 2012, reaching a nadir in 2021, followed by a resurgence in 2023. A decrease in scabies cases was also observed. However, from 2009 onward, this trend reversed, with cases increasing and peaking in 2014. Subsequently, the number of cases reached a new low in 2022, before increasing again in 2023. For Salmonella/Shigella, the number of tests remained around 5,000 in the early years, reaching a peak of 8,876 in 2020. This was followed by a decline, with 5,204 tests recorded in 2023. To minimize the risk of infectious disease transmission in prisons, several preventive measures should be implemented, including screening of newly admitted prisoners, introduction of prophylactic programs, and development of standardized procedures to follow in cases of infection.
Key words: prison health, tuberculosis pulmonary epidemiology, scabies epidemiology, enteric diseases epidemiology, overcrowding
Introduction
Specific conditions prevalent in penitentiary institutions can significantly increase the risk of infectious disease transmission among incarcerated populations. Several factors contribute to this heightened vulnerability in prison settings, including overcrowding, limited access to safe drinking water, delayed diagnosis, and poor ventilation.1 Existing literature consistently reports elevated rates of infectious diseases within correctional facilities worldwide, including tuberculosis (TB), HIV (which can progress to AIDS), hepatitis C virus (HCV), and COVID-19.2, 3, 4, 5, 6, 7, 8, 9, 10 Furthermore, the particular conditions inherent in prison environments may facilitate the transmission of foodborne illnesses and infections caused by ectoparasites such as mites.
Tuberculosis, caused by the bacterium Mycobacterium tuberculosis, is notably more prevalent in prisons than in the general population and remains one of the leading causes of death among incarcerated individuals.1, 2, 3 Studies show that the prevalence of active TB is closely linked to the country in which the prison is located. In high-burden TB countries, the incidence of active TB is 2.5 times higher than in countries with a lower burden.3 Tuberculosis typically presents as a pulmonary infection and is transmitted through inhalation of aerosolized droplets from an infected individual. Its constitutional symptoms are nonspecific and usually include a persistent cough, fever, weight loss, night sweats, and general malaise.11
According to data from the European Centre for Disease Prevention and Control (ECDC), presented in the Annual Epidemiological Reports (AERs), 30 countries within the European Union/European Economic Area (EU/EEA) reported a total of 36,179 TB cases in 2022 (8.0 per 100,000 population). Of these, 25.6% occurred in Romania (9,270 cases), while only 1 case was recorded in Liechtenstein.12 Compared with previous years, a slight increase was noted. The number of reported drug-resistant TB cases in the EU/EEA also rose in 2022, which can be attributed to factors such as the resumption of regular testing after the COVID-19 pandemic, migration resulting from the war in Ukraine, and the expansion of targeted TB screening programs for high-risk populations.
Although the World Health Organization (WHO) has set a target of 85% for TB treatment success, the actual success rate reported in 2022 was only 64.0%, highlighting the need for significant improvement.12 The Status Report on Prison Health in the WHO European Region 2022, which includes data from 16–28 member states, reported a TB prevalence of 0.46% among prison populations.13
A study published in 2021 found that TB cases among incarcerated individuals in Central and South America increased by 269% between 2000 and 2018. The prevalence of TB is disproportionately concentrated among people in prison, with 11% of all TB cases occurring within this population. In the past year, TB outbreaks have been reported in prisons in both Brazil and Venezuela.14
Scabies is an ectoparasitic infestation caused by Sarcoptes scabiei var. hominis, an obligate human parasite that completes its entire life cycle on the host. Female mites burrow into the stratum corneum of the skin to lay eggs, triggering an immune response that causes intense itching (pruritus) and erythematous rashes. The mites can survive for up to 24–36 h in environments with temperatures around 21°C and relative humidity levels between 40% and 80%, thus posing a risk of transmission during this period. Scabies is primarily spread through prolonged skin-to-skin contact with an infected individual. Symptoms usually appear 4–6 weeks after the initial infestation and typically include generalized itching, which worsens at night, along with a vesicular or papular rash.15, 16 In 2017, the WHO classified scabies as a Neglected Tropical Disease (NTD). However, epidemiological data on scabies remain limited in many countries, with most estimates based on a small number of non-representative surveys. Current estimates suggest a global point prevalence of 100–200 million scabies cases, with approx. 455 million new cases occurring each year. Scabies is estimated to cause around 3.8 million disability-adjusted life years (DALYs), making it one of the highest-burden NTDs.17
Salmonella is a genus of bacteria in the Enterobacteriaceae family and a major cause of gastroenteritis in humans. Transmission occurs primarily through ingestion of contaminated food or water, with poultry and poultry-derived products serving as key reservoirs. The severity of illness depends on the specific Salmonella serotype and the immune status of the host. The infection is classified into 2 main forms: typhoidal, which is characterized by persistent fever, headache, abdominal pain, anorexia, bradycardia, and either diarrhea or constipation; and non-typhoidal, which presents acutely with diarrhea, abdominal cramps, and fever.18
In 2022, 30 EU/EEA countries reported 66,721 cases of salmonellosis, of which 65,967 were laboratory confirmed. The highest numbers were recorded in the Czech Republic (7,563 cases) and Slovakia (3,669), while the lowest were reported in Portugal (412), Bulgaria (310), and Latvia (90). Although the number of cases increased compared with 2020, it remained lower than pre-COVID-19 levels.19
Shigellosis is an infection caused by bacteria of the Shigella genus, a group of facultative anaerobic, Gram-negative bacilli. Transmission occurs via the fecal–oral route, typically through direct person-to-person contact, ingestion of contaminated food or water, or, in some cases, through sexual contact, particularly among men who have sex with men. The hallmark clinical manifestation of shigellosis is dysentery, characterized by bloody, often mucous-laden diarrhea accompanied by abdominal cramps and vomiting.20
In 2022, 30 EU/EEA countries confirmed a total of 4,149 shigellosis cases. The highest numbers were reported in France (1,290 cases), Spain (598), and the Netherlands (419). Two countries (Iceland and Liechtenstein) reported no cases. Compared with 2020 and 2021, an increase in incidence was observed.21
Objectives
The aim of this study was to evaluate the incidence and epidemiological trends of TB, scabies, Salmonella, and Shigella infections among prisoners in Poland between 2002 and 2023, as well as to analyze the available literature addressing these diseases. The literature was sourced from publications indexed in Web of Science (WoS) and Scopus and published between 2015 and 2025. Additionally, this study sought to identify the most effective infection prevention strategies for implementation in penitentiary settings.
Materials and methods
This research consisted of 2 parts. First, a systematic review was conducted to analyze the existing literature on infectious diseases in prison populations, with a particular focus on TB, Salmonella, Shigella, and scabies. Second, findings from the authors’ own empirical research are presented. Ethical review and approval were waived for this study because public databases were used.
Systematic review
Strategy of searching and criteria of material selection
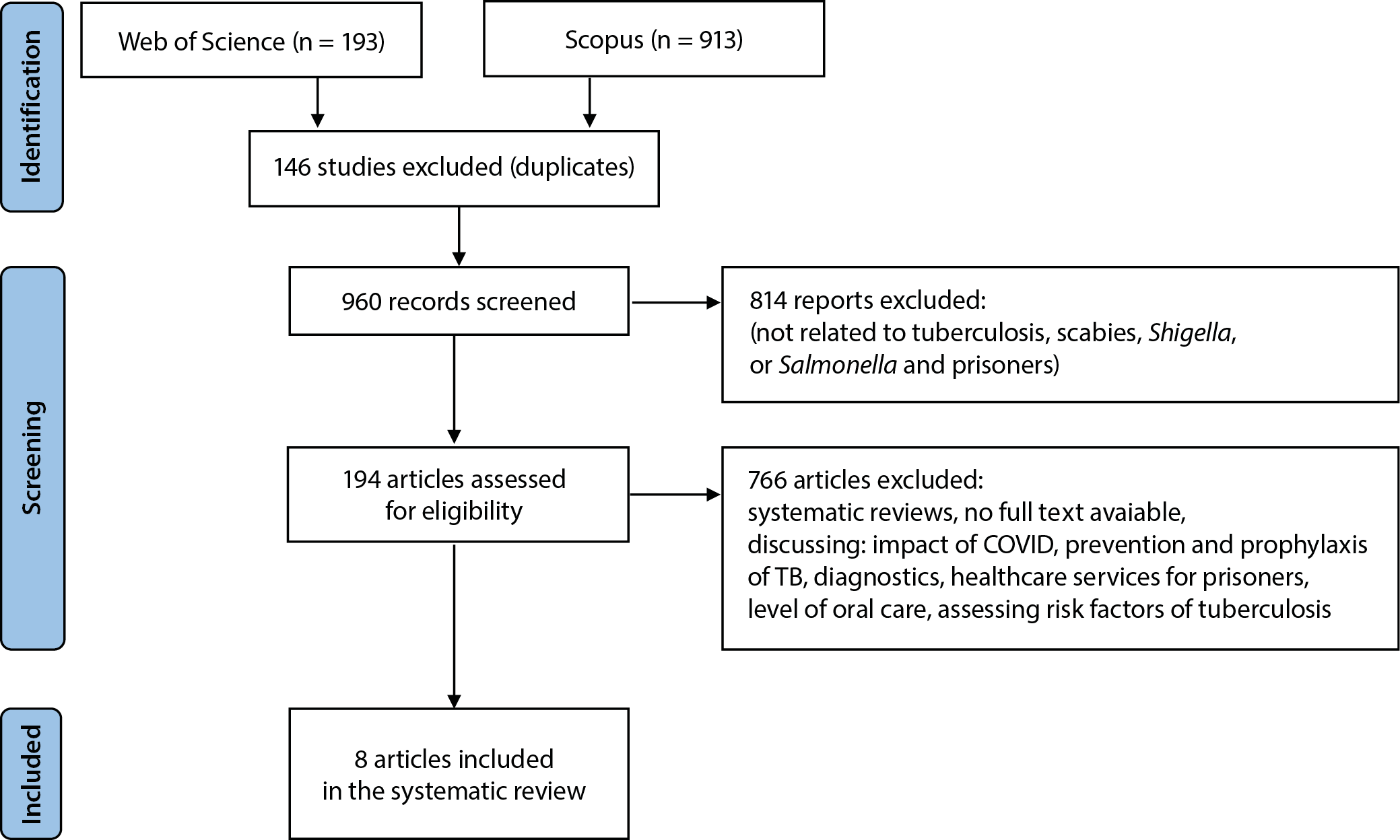
The research protocol was prepared based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). The available literature on TB, Salmonella, Shigella, and scabies infections among inmates was analyzed. To gather the literature, 2 databases were searched: Scopus and WoS. The inclusion and exclusion criteria were as follows:
Inclusion criteria: original articles presenting TB (diagnosed using X-ray findings or epidemiological data from national institutions), Salmonella, Shigella, and scabies infections in prisoners; articles published in English between January 1, 2015 and April 9, 2025; full-text articles available; and studies assessed as satisfactory using the Newcastle–Ottawa Scale. Exclusion criteria: case reports, reviews, articles without full-text availability, and articles discussing the impact of COVID-19, prevention and prophylaxis of TB, diagnostics, healthcare services for prisoners, or risk factors for TB.
For database searching, the following keywords were selected: “prison” OR “inmates” OR “prisoners”; “infectious diseases”; “TB” OR “scabies” OR “Shigella” OR “Salmonella”. Medical Subject Headings (MeSH) were used to identify appropriate search terms. Studies were screened by title and abstract according to the PICO (population, intervention, control, and outcome) criteria. The PICO question was as follows: Are prisoners at an increased risk of infection with TB, scabies, Salmonella, or Shigella compared with the general population?
The search was conducted on April 9, 2025. Article selection was performed independently by 2 calibrated researchers (A.T. and R.K.). Agreement between the reviewers was assessed using Cohen’s kappa coefficient. The results were interpreted as follows: <0.00 – poor; 0.00–0.20 – slight; 0.21–0.40 – fair; 0.41–0.60 – moderate; 0.61–0.80 – substantial; and 0.81–1.00 – almost perfect. The agreement between the reviewers was 0.442.
Duplicates exclusion
To eliminate duplicates, a Python script was used. The script combined and processed 2 bibliographic datasets from WoS and Scopus to generate a unified list of medical publications. It began by reading Microsoft Excel 2013 (Microsoft Corp., Redmond, USA) and CSV files using the Pandas library, extracting relevant columns such as authors, title, source, and abstract. The script then standardized column names across both datasets and merged them into a single DataFrame. To remove duplicate entries, it created a “clean_key” column by stripping and normalizing article titles. After duplicate removal, source names were formatted in title case and the DataFrame index was reset. The final dataset was used to generate a Word document using the python-docx library. Each publication entry was formatted with bold labels and listed as a numbered item. The final document included the title, authors, source, and abstract for each article. This approach ensured consistent formatting and removed redundancies across multiple bibliographic sources (Figure 2).
Substantive analysis
The following information was extracted from the selected manuscripts: year of the study, country in which it was conducted, characteristics of the study participants, and information on the prevalence of selected infectious diseases among inmates. Data were extracted by 1 researcher (A.T.). The extracted information was checked by another co-author (M.T.) to minimize the risk of bias.
Quality assessment
The reliability of the studies was assessed using the Newcastle–Ottawa Quality Assessment Scale for cross-sectional studies. The following domains were assessed: selection (SD), comparability (CD), and outcome (OD). The maximum score was 10 points: 5 points for the 1st category, 2 points for the 2nd category, and 3 points for the outcome domain. Interpretation of the Newcastle–Ottawa Quality Assessment Scale was as follows:
− 9–10 points: very good quality;
− 7–8 points: good quality;
− 5–6 points: satisfactory quality;
− 0–4 points: unsatisfactory quality.
This part of the research was conducted independently by 2 authors (A.T. and R.K.). Any discrepancies were resolved by the 3rd author (M.R.).
Analysis of epidemiological data
The research methodology was based on the possibility of obtaining anonymized data concerning inmates in all prisons across the country diagnosed with TB, scabies, Salmonella, and Shigella infections between 2002 and 2023. Access to these sensitive data was possible due to the obligation of the Prison Service (PS) to provide health-related information about inmates to Statistics Poland, in accordance with the provisions of the Act of June 29, 1995, on Public Statistics,22 as well as the annually updated Program of Statistical Research of Public Statistics (PSRPS). According to the Public Statistics Act, Article 13: “Respondents, including entities in the public finance sector, are obliged to provide statistical data free of charge for the purposes of public statistics.” Health data of prisoners, transmitted by the PS to statistical offices, are collected and forwarded on the basis of medical reports and healthcare registry systems within correctional facilities. These data are gathered through internal registry systems that maintain detailed medical documentation of inmates. Subsequently, the PS submits this information to statistical offices, such as Statistics Poland, for the purposes of analysis, reporting, and use in social and health research. For this study, publicly available data from the PS official website (https://sw.gov.pl/strona/Statystyka) were used. The information contained there is collected through internal recording systems based on medical reports related to inmate healthcare.
Due to the retrospective and noninvasive nature of the study, and because all data were anonymous, ethics committee approval was not required. Studies exempt from ethical approval include most educational research, case reports on 1–3 patients (without hypothesis testing), studies involving no risk to participants, studies involving information available in the public domain, analyses of open-source or anonymized datasets obtained from other researchers with appropriate informed consent collected during primary data collection, and research evaluating public health programs or government schemes.23
Statistical analyses
The Shapiro–Wilk test was conducted to evaluate whether the distribution of a given variable conformed to a normal distribution. The test results indicated a significant deviation from normality (p < 0.050). Consequently, it was deemed appropriate to utilize Spearman’s rank correlation coefficient instead of Pearson’s correlation coefficient, as the former does not require the assumption of normality in the data distribution. Using Spearman’s rho correlation coefficient, the association between variables that did not follow a normal distribution was assessed. The p-values were determined using an asymptotic approximation based on the t-test. The p-values were additionally adjusted (padj) using the Holm method when multiple comparisons were assessed.
The growth rate of the time-series data was quantified using the compound annual growth rate (CAGR) parameter, calculated with the following formula (https://www.calkoo.com/en/cagr-calculator):
CAGR = (EV/BV)^(1/n) − 1,
where: EV – the value of the studied parameter in the final year; BV – the initial value in the first year; n – the number of years under observation. Analyses were conducted using R v. 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria) on Windows 10 Pro 64-bit (build 19045; Microsoft Corp.), using the packages sjPlot v. 2.8.15 (https://strengejacke.github.io/sjPlot), report v. 0.5.7,24 ggstatsplot v. 0.12,25 and ggplot2 v. 3.4.4.26 Microsoft Excel 2013 and Statistica v. 11.0 (StatSoft Inc., Tulsa, USA) were used to carry out the analyses.
Results
Systematic review
Quality assessment
The Newcastle–Ottawa Scale was used to assess the quality of the 8 articles included in the review. This part of the research was conducted independently by 2 authors (A.T. and R.K.). Any discrepancies were resolved by the 3rd author (M.R.) (Table 1). Only 1 article was assessed as satisfactory, 2 as good, and 5 as very good.
Study characteristics
Two databases were searched: Scopus and WoS. As a result, 1,106 articles were identified (Figure 1). After removing duplicates, 960 articles were obtained for the first screening. In the next step, the articles were analyzed with regard to the inclusion criteria, which resulted in the exclusion of 814 articles that did not address the prevalence of the selected infectious diseases (TB, Salmonella, Shigella, or scabies). Subsequently, 766 articles were excluded for the following reasons: being systematic reviews, unavailability of the full text, or focus on topics such as the impact of COVID-19, prevention and prophylaxis of TB, diagnostics, healthcare services for prisoners, level of oral care, or assessment of TB risk factors.
As a result, 8 articles were included in the review (Table 2). Each article described the situation in a different country (USA, Côte d’Ivoire, North Macedonia, Iran, Gauteng, Limpopo, Mpumalanga and North West Provinces in South Africa, China, Poland, and Ghana). One article was published in 2016, 1 in 2017, 2 in 2018, 2 in 2019, 1 in 2020, and 1 in 2024. Six of the articles discuss TB infections,27, 28, 29, 30, 31, 32 while 2 address scabies infections in prisons.33, 34
None of the articles included in the review addressed the problem of Salmonella or Shigella infections. During article screening, the authors identified 1 article describing Salmonella; however, because it was a case report, it was excluded from the review.
Tuberculosis in prisons
The problem of TB in penitentiaries is widely discussed in the available literature. In 4 articles, the authors performed X-rays to confirm the TB diagnosis.28, 30, 31, 32 Séri et al.28 confirmed the diagnosis through medical examination and interview, followed by chest X-rays and sputum collection. Similar methodology was used by authors from Iran, South Africa, and China.30, 31, 32 Researchers from North Macedonia and the USA decided to analyze data provided by national institutions. Lambert et al.27 analyzed data obtained from the National Tuberculosis Surveillance System. Authors from North Macedonia gathered information from the Central Register for TB within the Institute for Lung Diseases.29 Table 3 presents the results of the research described in the studies included in the review.
Scabies in penitentiary institutions
Bartosik et al.33 analyzed data provided by the Central Board of the Prison Service and the District Inspectorate of the Prison Service in Lublin. They also described the problem of pediculosis in prisons. The 2nd article included in the review and discussing the problem of scabies was authored by researchers from Ghana.34 They conducted a cross-sectional study, collecting information from medical histories and demographic data using the Research Electronic Data Capture (REDCap) questionnaire. Subsequently, skin examination was performed and scabies was diagnosed according to the criteria of the International Alliance for the Control of Scabies (ICAS).34 The results of these 2 studies are presented in Table 4.
Epidemiological data analysis
Analysis of X-ray screenings and tuberculosis detection in Polish prisons (2002–2023)
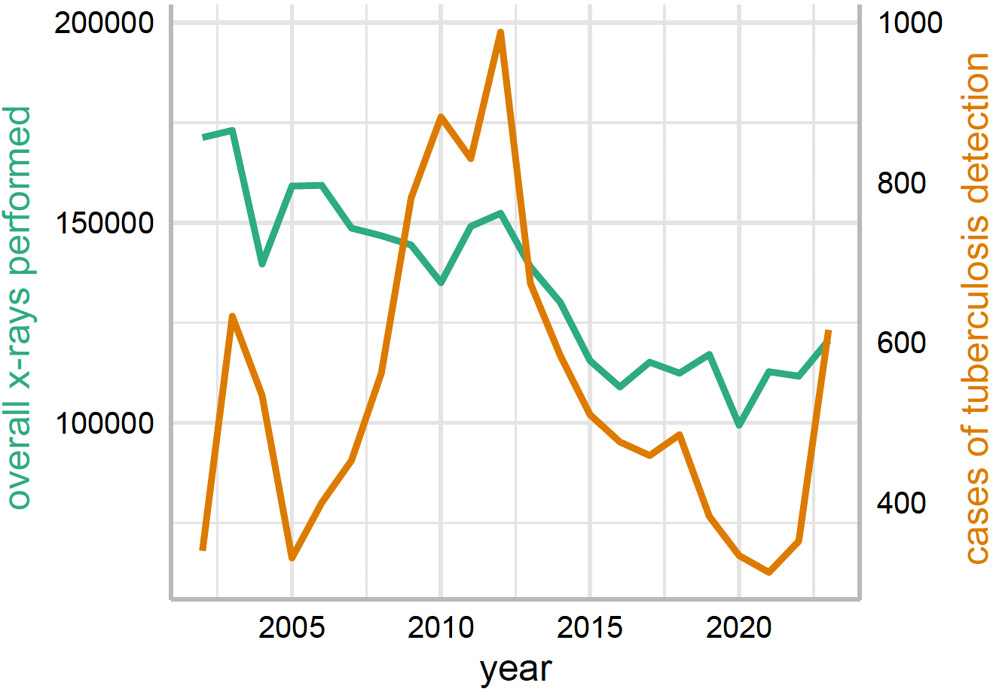
Over the 22-year period, a discernible trend emerges from the analysis of X-ray screenings and TB case detection (Figure 3). Initially, a slight increase in the number of X-rays performed was observed, peaking at 173,047 in 2003, followed by a general downward trajectory to a low of 99,400 in 2020.
Parallel to the changing frequency of X-ray use (CAGR = −1.9%; 95% confidence interval (95% CI): −2.9 to −1.9), the number of TB cases detected showed substantial fluctuation, not strictly following the pattern of X-ray screenings. A significant rise in TB cases was noted from the early to mid-2010s, peaking in 2012 with 988 cases. Subsequently, a decrease in TB cases after 2012 was observed, reaching a nadir in 2021, followed by a resurgence to 616 cases in 2023.
Trends and compound annual growth rate analysis of scabies cases in Polish prisons (2002–2023)
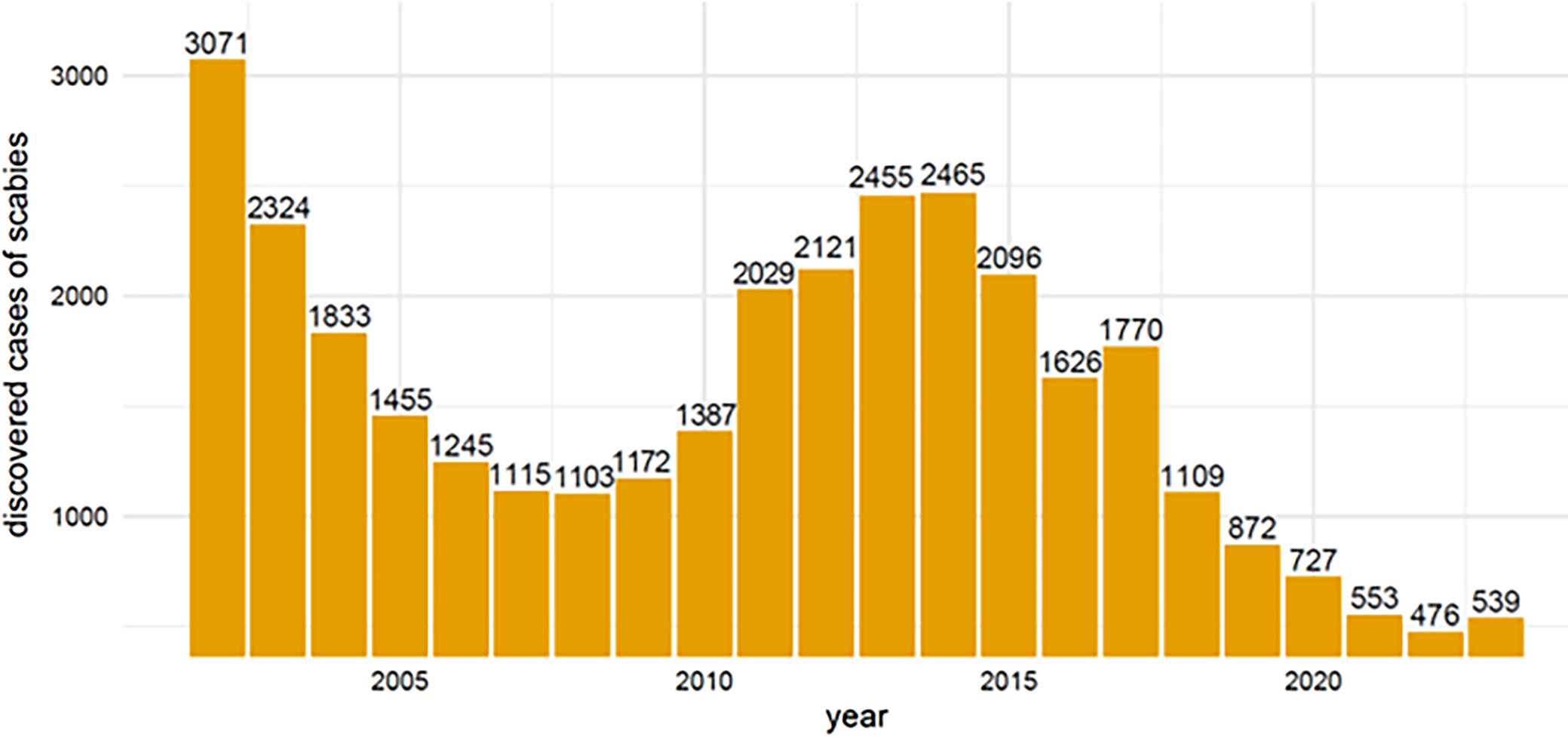
The data in Figure 4 represent the number of scabies cases reported annually from 2002 to 2023. Initially, there was a consistent decrease in cases from 3,071 in 2002 to 1,103 in 2008. However, from 2009 onwards, there was a noticeable reversal in this trend, with cases increasing and peaking in 2014 at 2,465 cases. After reaching the peak in 2014, the number of cases began to decline again. By 2021, the number of cases had dropped significantly to 553, reaching a new low in 2022 with 476 cases, before a slight increase to 539 cases in 2023. This negative CAGR of approx. −2.4% (95% CI: −3.6 to −1.3) annually over the 21-year period indicates a general decline in scabies cases despite the observed fluctuations. This overall decline suggests that the measures implemented over the years have been largely effective, albeit with periods of challenge requiring renewed focus and possible adaptation of strategies.
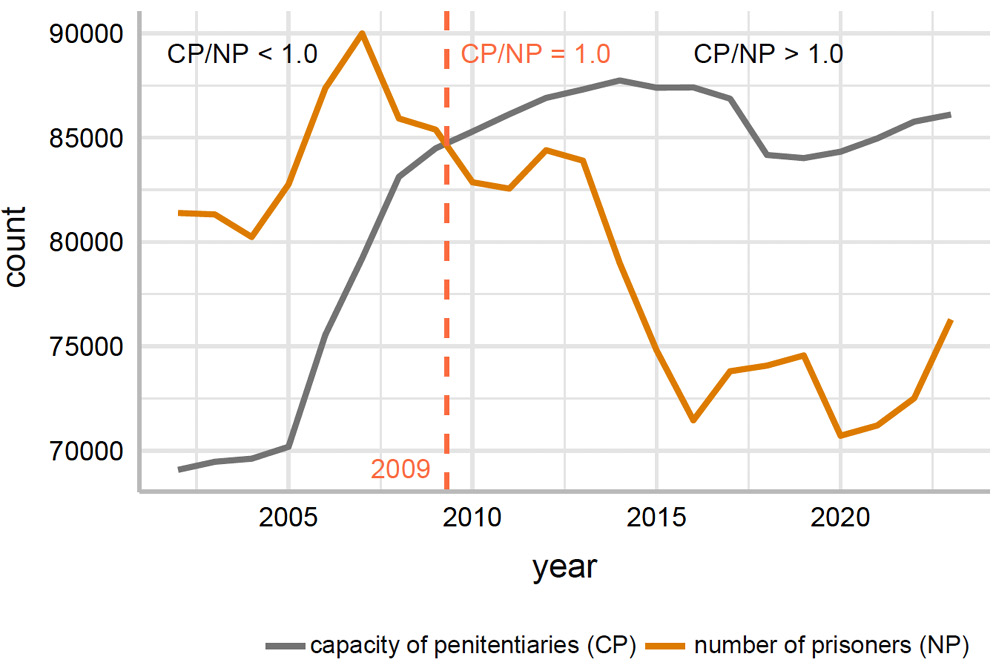
The analysis of trends in penitentiary capacity and inmate population in Poland from 2002 to 2023, based on the data presented in Figure 5, reveals the dynamics of the prison system over 2 decades. Overall, the data from 2002 to 2023 reveal a correctional system that has undergone significant changes aimed at effectively balancing capacity with inmate populations.
Initially, both capacity and the number of inmates showed an upward trend. The capacity of penitentiaries increased steadily from 69,083 in 2002 to a peak of 87,742 in 2014, reflecting a systematic expansion of facilities, which coincided with an increase in the inmate population, reaching a peak of 89,995 in 2007 (Figure 5).
Annual trends in diagnostic examinations for Salmonella/Shigella: volume, positivity rates, and comparative analysis in Polish prisons (2002–2023)
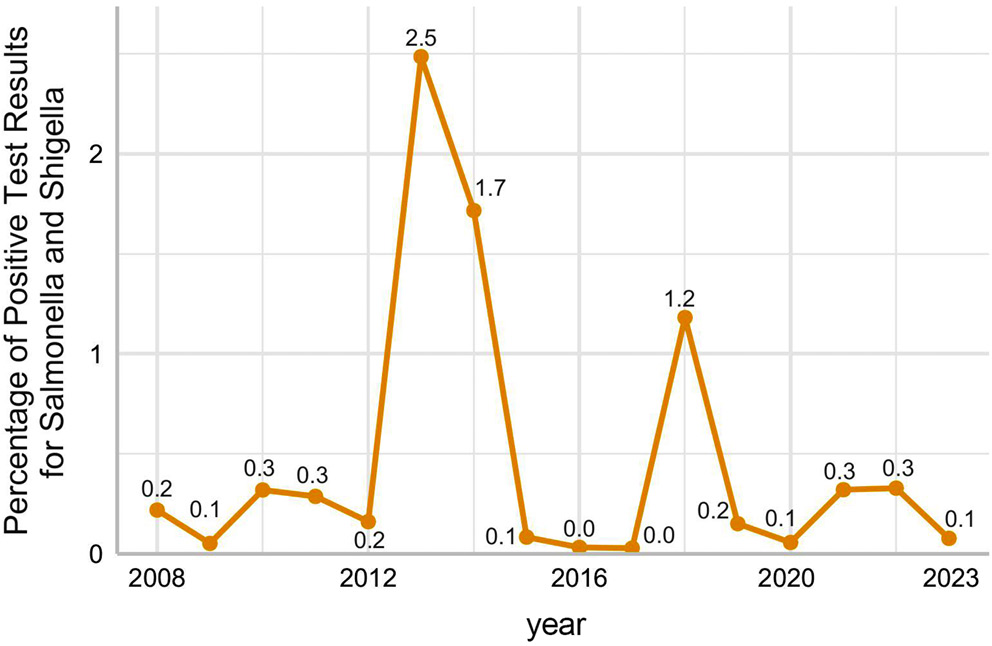
Analyzing the data on diagnostic tests for Salmonella/Shigella in Polish inmates from 2002 to 2023 reveals interesting trends in both the number of tests conducted and the positivity rates for each disease.
For Salmonella/Shigella, the number of tests initially hovered around 5,000 in the early years, gradually increasing to a peak of 8,876 in 2020. Following this peak, there was a noticeable decline, with 2023 recording 5,204 tests (CAGR = −0.77%; 95% CI: −2.50 to 1.10). The positivity rates for these tests were generally low, often below 1%, except for certain years such as 2013 and 2014, when they increased to 2.48% and 1.72%, respectively (Figure 6).
Discussion
The effective implementation of this research project, which enabled the collection of selected anonymized statistical data from specific study cohorts – particularly inmates – was made possible by the robust operation of the statutory obligation requiring the PS to transmit health-related data concerning inmates to Statistics Poland. The PS is legally authorized to process personal and sensitive data, including inmates’ health information, without explicit consent when such processing is necessary to fulfill statutory duties, maintain order and security within penitentiary institutions, and provide appropriate living and healthcare conditions. All data processing is conducted in strict compliance with data protection regulations, with full respect for individual dignity and the right to privacy. Personal data may be processed and disseminated in a manner that precludes identification of individuals, particularly for statistical and research purposes.35
Although prison systems vary globally, common challenges are observed across countries – overcrowding, poor inmate health, inactivity, violence and abuse, substance use disorders, and limited access to healthcare – each representing major public health concerns.36 In 2023, the global occupancy rate in penitentiary centers varied significantly: 616.9% in the Republic of the Congo (Congo-Brazzaville), 302% in Haiti, 231.4% in Peru, 176.5% in Kenya, 101.5% in Hungary, 95.6% in the USA, 77.6% in Germany, 67.0% in Russia, 56.6% in Japan, 31.0% in Monaco, and 14% in Nauru. In Poland, the occupancy rate was reported at 87.2%.37, 38
Despite an increase in prison capacity, the prisoner-to-capacity ratio in Poland exceeded 1.0 until 2009, indicating persistent overcrowding. From 2010 onward, this ratio dropped below 1.0, suggesting either a reduction in inmate numbers or effective expansion of prison infrastructure. Notably, after 2014, both the number of prisoners and available capacity declined – although the inmate population fell at a faster rate. By 2016, the ratio had reached its lowest point (0.82) and remained below 0.9 through 2023. These trends may reflect successful reforms such as sentencing alternatives, non-custodial penalties, and recidivism reduction programs. Overcrowding is a well-established factor contributing to the spread of infectious and parasitic diseases, including TB, scabies, Salmonella/Shigella infections, and HIV. Our findings show that increases in TB and scabies cases are closely correlated with prison population density. The highest number of TB cases was recorded in 2012 (988 cases), yet this did not coincide with the peak in X-ray screenings, indicating that other factors – such as overcrowding or more virulent TB strains – may have contributed. A decline followed, reaching a low point in 2021, before resurgence in 2023. The weak correlation between case rates and X-ray screening volume (rho = 0.28, p = 0.203, 95% CI: −0.16 to 0.63) suggests that screening alone is insufficient to control TB and should be part of a broader health strategy.
The decrease in screening rates and the complex trend in TB incidence (CAGR = 2.5%, 95% CI: 0.6–4.4) reflect the dynamic nature of healthcare challenges in prisons. This underscores the need for ongoing adaptation – through advanced diagnostics, improved control measures, and better healthcare access for inmates. Notably, the significant drop in screenings in 2020 likely resulted from the COVID-19 pandemic disrupting routine care. Tuberculosis remains a strong indicator of overall infection control performance, and its persistence raises broader concerns about institutional preparedness for managing infectious disease outbreaks, including SARS-CoV-2.39
Our findings align with those of Placeres et al.,3 whose meta-analysis confirmed TB in prisons as a global public health and social issue, advocating rapid assessments and precision interventions in correctional settings. Several other studies confirm the elevated TB burden in prisons,27, 28, 29, 30, 31, 32 including work by Séri et al.,28 Ilievska-Poposka et al.,29 Seyedalinaghi et al.,30 Jordan et al.,31 and Tong et al.,32 all of whom emphasized the urgent need for effective TB management systems in penitentiaries.
Implementing protective measures, including screening of inmates, prophylactic programs, and protocols in case of an outbreak, could minimize the risk of infectious disease transmission in prisons. Beaudry et al.40 conducted a systematic review on managing outbreaks of highly contagious diseases in prisons. Out of 28 studies included in the review, 14 agreed that screening was crucial to reduce the causes of the outbreak. Kending et al.41 reviewed the challenges and strategic opportunities for infection prevention and control (IPC) efforts in U.S. jails and prisons. They recommended several steps that could improve IPC: training personnel to manage IPC programs, improving infectious disease surveillance, preparing augmented evidence-based guidance particularly for correctional facilities, strengthening external stakeholder engagement (vaccination programs, screening, outbreak management), and developing and funding a national research agenda to evaluate IPC implementation. In the USA, scientific reports have identified a correlation between the rise of AIDS and the resurgence of TB in prisons, particularly since the beginning of the HIV/AIDS epidemic in 1981.42
Scabies remains a public health challenge both in Poland and globally.43, 44, 45, 46 Korycińska et al.43 found that scabies prevalence was highest in urban and rural communities, correlating with reduced healthcare access and lower health literacy. Adolescents (aged 10–19 years) were most affected, likely because of increased close contact. The infection also correlated with socioeconomic status, including residence in areas with high unemployment.
A systematic review by Delie et al.16 linked scabies in prisons to poor hygiene, overcrowding, shared beds and clothing, and shorter sentence lengths. Similar results were presented by Bogino et al.,5 who found strong associations with inadequate hygiene, shared clothing, lack of soap, and poor ventilation.
In our analysis, scabies incidence declined from 2002 to 2008, rose to a peak in 2014, and then declined again. These fluctuations may reflect varying levels of disease control, changes in reporting practices, or other institutional factors. The likely driver of the mid-period increase was prison population growth. However, Bartosik et al.33 found no clear correlation between inmate numbers and scabies cases in Polish prisons (2001–2015), with higher inmate counts sometimes coinciding with fewer cases.
Only 2 studies in our review discussed scabies prevalence in Poland and Ghana.33, 34 Between 2001 and 2015, Polish data showed a mean infection rate of 2.3% (min 1.2% in 2007; max 3.9% in 2001), while at Kumasi Central Prison in Ghana, scabies prevalence reached 65.8%. This stark contrast highlights the critical importance of control measures, hygiene, and health education.
The literature also documents outbreaks of Shigella and Salmonella in correctional facilities.6, 7, 8 Ranjabar et al.6 described a Shigella flexneri outbreak in Isfahan, Iran, linked to raw vegetable consumption. Gicquelais et al.7 emphasized strict food safety practices after a Salmonella outbreak in 2 Arkansas prisons caused by contaminated eggs. Mardu et al.8 advocated food-handler education as a means of outbreak prevention.
In our study, the highest positive test rates for Shigella and Salmonella were recorded in 2013 (2.48%) and 2014 (1.72%), respectively. This could suggest increased awareness and testing during that period or reflect actual outbreaks mitigated by staff training and better food safety practices.
Insfran-Rivarola et al.47 in their systematic review analyzed the effects of food safety and hygiene training on food handlers. They included 31 studies in the review and classified them into 3 categories according to the main outcome. Sixteen articles reported changes in food safety practices, with interventions increasing adherence to food safety practices. The authors agreed that, for the training to be more successful, it is important to combine theory and practice, as active participation in training has been shown to be more effective. Moreover, they noted that such programs should be implemented regularly to prevent knowledge attrition.
Dadu et al.48 reported a decline in TB incidence in European prisons (2014–2018), including in Russia. This trend likely reflects WHO-backed national TB control strategies launched in 2014. A similar pattern was observed in Poland, where TB incidence declined between 2014 and 2017. In Poland, prison healthcare is governed by the Regulation of the Minister of Justice, published on June 14, 2012 (https://eli.gov.pl/eli/DU/2012/738/ogl), with subsequent amendments likely contributing to improved TB control.
The use of a Python script was the authors’ own approach, which enhanced the selection process during the article-screening stage. This method may be useful for other authors preparing a systematic review.
Limitations of the study
Several limitations must be acknowledged. First, we analyzed only secondary data provided by authorities; no direct patient examination was conducted. We do not have information on the basis on which the diagnoses were established or whether they were validated through laboratory testing. Second, we lack information on whether data collectors were trained and standardized, which limits methodological comparability. Third, data on scabies were incomplete, and no data on Salmonella or Shigella infections were available before 2008, restricting trend analysis to more recent years.
Conclusions
Overcrowding in prisons, observed from 2002 to 2023, has contributed to the transmission of infectious and parasitic diseases, particularly scabies, as well as TB and Salmonella/Shigella infections. A marked increase in TB cases occurred from the early to mid-2010s, peaking in 2012. This rise does not correspond to the highest number of chest X-rays performed. The elevated number of positive test results for Salmonella/Shigella infections paralleled the growth of the prison population. This underscores the necessity for improved food safety protocols and more stringent oversight of food preparation practices within correctional facilities, with a particular emphasis on preventing gastrointestinal diseases and enhancing hygiene standards. To mitigate disease transmission within the prison environment, it is essential to implement rapid health assessments that enable targeted and precise interventions. Incarceration restricts personal liberties; however, this should not occur at the expense of reducing the minimum standard of healthcare, which should remain at least equivalent to that available in the general population. The available literature emphasizes the higher occurrence of TB compared with the general population and the need for implementation of effective systems to control TB and scabies in correctional settings.
The use of a Python script during the systematic review process (at the duplicate-removal stage) improved the process, saved time, and eliminated errors that may result from human factors. To minimize the risk of infectious disease transmission in prisons, several protective measures should be implemented. These include systematic screening of newly admitted inmates, introduction of prophylactic programs involving periodic screening, and development of clear response protocols in the event of an outbreak. Effective control of infectious diseases within correctional facilities requires coordinated efforts and collaboration among all relevant authorities.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.15806506. The package contains the following files:
The data presented in the supplementary tables and figures show the number of cases of the studied diseases among prisoners in Poland in individual years. Supplementary Table 1 and Supplementary Fig. 1 present the number of TB cases among inmates in Poland from 2002 to 2023.
A significant rise in TB cases was observed from the early to mid-2010s, peaking in 2012 with 988 cases. This was followed by a decline in TB incidence after 2012, reaching its lowest point in 2021, and then rising again to 616 cases in 2023. Supplementary Table 2 and Supplementary Fig. 2 present the number of scabies cases. Initially, a consistent decline was observed from 3,071 cases in 2002 to a low of 1,103 cases in 2008. However, from 2009 onwards, this trend reversed, with a steady increase peaking in 2014 at 2,465 cases.
After reaching this peak in 2014, the number of cases began to decline again. Supplementary Table 3 and Supplementary Fig. 3 present data on the number of inmates diagnosed with Salmonella or Shigella infections. The highest number of cases was recorded in 2013, with a total of 121 cases.
Data Availability Statement
The data that support the findings of this study are available in Zenodo at https://doi.org/10.5281/zenodo.15852790.
Use of AI and AI-assisted technologies
Not applicable.