
















Abstract
Background. Positron emission tomography (PET) using 18-fluorodeoxyglucose (18-FDG) is the primary imaging modality for mediastinal staging of lung cancer. Higher standardized uptake value (SUVmax) reportedly correlates with more aggressive and more readily detectable tumors. However, high-quality scientific evidence regarding the correlation between primary tumor SUVmax and PET performance in detecting mediastinal lymph node metastases remains limited.
Objectives. To analyze the correlation between 18-FDG SUVmax and the diagnostic yield of PET, as well as the impact of clinical factors such as age, sex, body mass index (BMI), primary tumor lobar location, and histological type on this relationship.
Materials and methods. This retrospective analysis utilized an institutional database and included a consecutive cohort of patients who underwent lung cancer surgery.
Results. In the overall cohort of 774 patients, PET demonstrated sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of 59%, 76%, 27%, and 92%, respectively. Significant differences in sensitivity were observed between the SUVmax < 10 and SUVmax > 15 groups (p = 0.007), as well as between the SUVmax 10–15 and SUVmax > 15 groups (p = 0.001). Significant differences in NPV were found between the SUVmax < 10 and SUVmax 10–15 groups (p = 0.011). Logistic regression analysis revealed no association between the risk of false negative (FN) PET results for detecting N2 disease and patient characteristics, primary tumor lobar location, or histological type.
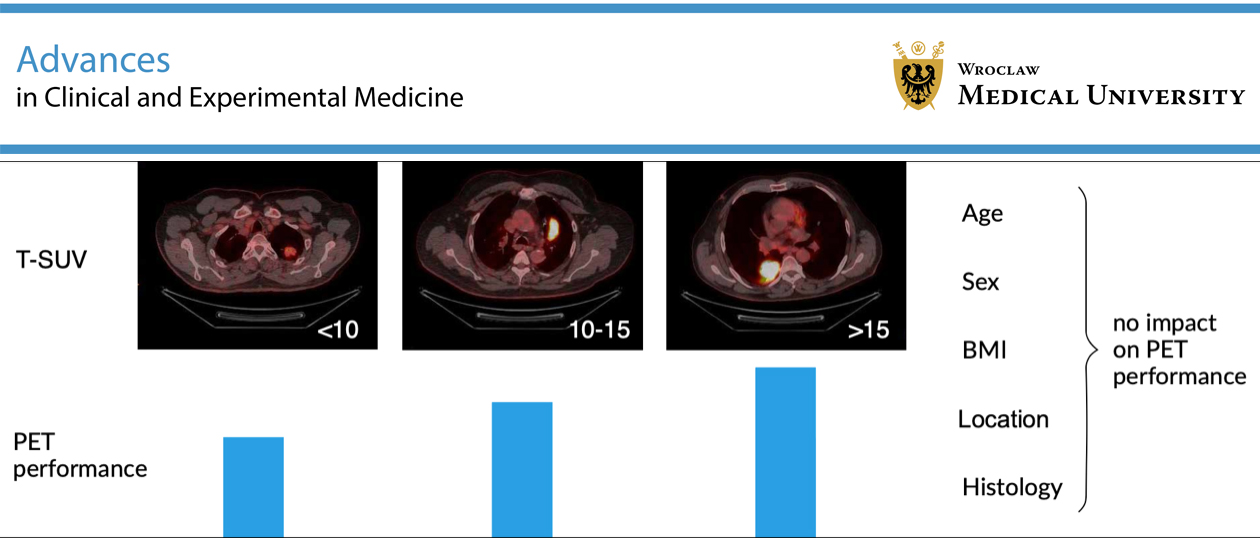
Conclusions. Our study confirms that higher SUVmax values of the primary tumor correlate with improved PET diagnostic performance in assessing mediastinal lymph node metastasis. A novel finding of this study is that clinical variables such as age, BMI, sex, tumor location, and histological type did not significantly influence the risk of FN results. The main limitations of this study are its retrospective design and single-institution cohort, which may not fully represent the diversity of patient demographics, disease characteristics, and treatment practices across different healthcare settings and populations.
Key words: lung neoplasms, neoplasm staging, lymph nodes, positron emission tomography, standardized uptake value
Background
Lung cancer is one of the leading causes of cancer-related mortality worldwide.1, 2 Positron emission tomography (PET) using 18-fluorodeoxyglucose (18-FDG) is the primary imaging modality for mediastinal staging of lung cancer. In particular, the negative predictive value (NPV) of PET is high.3, 4, 5, 6, 7 False positive PET results are common due to the glucose-dependent metabolism of leukocytes and granulation tissue. These mainly affect the specificity of PET and necessitate pathological confirmation of PET-positive lesions. However, as the primary goal of pretreatment evaluation is to exclude N2 disease, NPV remains the most important parameter.
Higher standardized uptake value (SUVmax) values reportedly correlate with more aggressive and more easily detectable tumors.8, 9 However, this does not directly translate into the risk of mediastinal lymph node involvement. Reliable assessment of the correlation between specific clinical characteristics and the probability of N2 disease requires analysis of large patient cohorts treated according to a uniform protocol. Such reports are lacking. Therefore, high-quality scientific data regarding the correlation between primary tumor SUVmax and PET performance in detecting mediastinal lymph node metastases remain limited. In addition, our understanding of the influence of different clinical variables on the diagnostic yield of PET is still incomplete.
Current guidelines from the European Society of Thoracic Surgeons (ESTS) indicate a low risk of N2 disease in cases of PET-negative mediastinum, tumor diameter <3 cm, and tumor location within the outer 1/3 of the lung. These guidelines do not consider primary tumor SUVmax as a risk factor for N2 involvement.10 From a practical perspective, it is important to determine whether similar diagnostic performance of PET can be expected across sexes, body mass index (BMI) categories, primary tumor lobar locations, and histological cancer types.
Objectives
The primary objective of this study was to analyze the correlation between the SUVmax of 18-FDG in primary tumors and the effectiveness of PET in diagnosing mediastinal lymph node involvement. The secondary objective was to evaluate the impact of clinical factors such as age, sex, BMI, primary tumor lobar location, and histological type on the rate of false negative (FN) PET results.
Materials and methods
Study design
This study employed a retrospective cohort design.
Clinical questions
1. Is there a correlation between the SUVmax of primary lung cancer and the diagnostic yield of PET in detecting mediastinal lymph node involvement?
2. What is the impact of specific clinical variables on the risk of obtaining FN results in N2 node assessment using PET?
Patients
The study included a consecutive group of surgically treated patients with non-small cell lung cancer (NSCLC). The inclusion criteria were: 1) age 18–90 years, 2) clinical stages I–IVA, and 3) curative-intent pulmonary resection with systematic lymph node dissection. The exclusion criteria were: 1) neoadjuvant treatment, 2) a final diagnosis other than NSCLC, and 3) incomplete mediastinal lymph node dissection.
Intervention
Positron emission tomography imaging was performed in all patients using a Discovery 690 scanner (GE Healthcare Chicago, USA). The upper limit of the allowed blood glucose concentration was 11 mmol/L. A weight-based formula for FDG dose calculation of 3–4 MBq/kg was used. The imaging protocol included computed tomography (CT) attenuation-correction imaging and lung window reconstruction, with specific data acquisition parameters (80–210 mA, 3.75 mm section thickness, and 0.8-s gantry rotation speed). Whole-body PET scans were conducted with a 2.5 mm section thickness. Both non-attenuation-corrected (NAC) and measured attenuation-corrected (MAC) images were acquired using the Q.Clear algorithm (GE Healthcare). The interval between FDG injection and data acquisition was 45–60 min. The maximum SUV values were calculated using Pet Odyssey software (GE Healthcare), adjusted for patient weight and administered isotope dose. Positron emission tomography positivity was defined with reference to the SUV value of the aortic arch. The PET images were analyzed by the same team. A radiologist and a nuclear medicine specialist independently reviewed each PET scan with access to the clinical data.
Next, endobronchial ultrasound (EBUS) and endoscopic ultrasound (EUS) imaging of the mediastinum were performed with fine-needle biopsy of all PET-positive lymph nodes. Patients with no evidence of mediastinal spread were scheduled for curative-intent surgery. Pathological N stage, determined by examination of the surgical specimen and generally considered the gold standard, was used as the reference test. During surgery, anatomical lung resection and systematic lymph node dissection were performed according to the ESTS guidelines.11 The consultant thoracic surgeon meticulously dissected lymph nodes from all stations and categorized them according to the 7th edition of the TNM classification.8
Postoperatively, tissue specimens were examined by an experienced lung pathologist with access to the clinical data. Standard light microscopy images with hematoxylin and eosin staining were used to diagnose nodal metastases (Olympus BX51; Olympus Corp., Tokyo, Japan).
Data extraction and handling
Relevant data, including demographics (age and sex), clinical details (cancer stage and histological type), treatment specifics (surgery type and PET scan parameters), and outcomes (pathological results and PET scan findings), were extracted from the hospital database. Extracted data were anonymized and securely stored to maintain patient confidentiality. Artificial intelligence (AI) was not used for the production of images or graphical elements in the paper, nor for data collection or analysis.
Statistical analyses
Statistica v. 13.5 PL (StatSoft Inc., Tulsa, USA) was used for statistical analysis. Logistic regression models were used to identify factors associated with FN PET results. Variables were grouped as follows: age (<60, 60–70, and >70 years), BMI (18.5–25 kg/m2, >25–30 kg/m2, and >30 kg/m2), and SUVmax (<10, 10–15, and >15). Both univariate and multivariate models were constructed. Initially, the forward stepwise selection method was applied to identify promising predictor variables efficiently. The results were then compared with those obtained using best subset selection, which examines all possible predictor combinations but is more computationally intensive. Odds ratios (ORs) with 95% confidence intervals (95% CIs) calculated using the Clopper–Pearson exact method were used to interpret important factors. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the entire patient cohort and for subgroups based on sex, age, histological type, BMI, SUVmax, and primary tumor lobar location. The 95% CIs for sensitivity and specificity were also calculated and compared across specific SUVmax categories. Statistical significance was set at p < 0.05.
Results
In total, 884 patients were included. Of these, 110 met the exclusion criteria (89 received neoadjuvant chemotherapy, 17 had a final diagnosis other than NSCLC, and in 4 patients, complete mediastinal lymph node dissection was not performed due to intraoperative cardiopulmonary instability). Thus, data from 774 patients were analyzed. The characteristics of the study groups are presented in Table 1.
For the entire cohort, the sensitivity, specificity, PPV, and NPV of PET were 59%, 76%, 27%, and 92%, respectively. Detailed values according to sex, age, and BMI are presented in Table 2.
Separate analyses were performed for subgroups according to SUVmax categories: <10, 10–15, and >15. The results are summarized in Table 3.
A significant difference in sensitivity was found between the SUVmax < 10 and SUVmax > 15 groups (p = 0.007) and between the SUVmax 10–15 and SUVmax > 15 groups (p = 0.000). For NPV, a significant difference was found between the SUVmax < 10 and SUVmax 10–15 groups (p = 0.011). Logistic regression analysis did not show an association between the risk of FN PET results in detecting N2 disease and the following factors: age (p = 0.769), BMI (p = 0.430), sex (p = 0.231), primary tumor lobar location (p = 0.312–0.757), upper vs lower lobe location (p = 0.126), and histological type (p = 0.623–0.999). Simplified categorization into squamous and nonsquamous histology also showed no significant association (p = 0.275). Multivariate logistic regression analysis, which further investigated potential associations between FN results and clinical factors, also did not reveal significant relationships (p = 0.079–0.469).
Discussion
There is a large body of evidence demonstrating the strong prognostic value of N status.12 The prognostic value of primary tumor SUVmax has been confirmed in several studies.13, 14, 15 Our analysis of data from 774 patients revealed that the sensitivity, specificity, PPV, and NPV of PET were 59%, 76%, 27%, and 92%, respectively. These values are consistent with previous studies that also demonstrated a high NPV of PET in evaluating mediastinal lymph node metastasis.3, 4, 5, 6, 7
Our findings revealed significant differences in sensitivity among the primary tumor SUVmax categories of <10, 10–15, and >15. The group with SUVmax > 15 exhibited significantly higher sensitivity, suggesting that higher glucose metabolism in the primary tumor was associated with improved detectability of lymph node metastases using PET. This may be attributable to a higher likelihood of nodal metastasis arising from less differentiated tumor cell clones. These findings are consistent with previous research indicating that higher SUVmax values correlate with more aggressive and more easily detectable tumors.8, 9 According to some authors, higher primary tumor SUV is associated with a higher rate of FN results regarding N2 node metastasis.5, 6, 7, 16 Our previous study demonstrated a correlation between primary tumor SUVmax and histological grade, further supporting the present findings.17
Logistic regression analysis did not show a significant association between the risk of FN PET results and factors such as age, BMI, sex, lobar tumor location, or histological type. This suggests that the diagnostic yield of PET for detecting N2 disease is consistent across different patient populations. To the best of our knowledge, this is the only study to analyze this relationship. Our findings are important from a practical perspective, as they demonstrate that the diagnostic performance of PET is similar across sexes, age groups, BMI categories, tumor locations, and histological tumor types. Moreover, these findings suggest that greater caution should be exercised when assessing N2 disease in patients with primary tumor SUVmax < 15, as sensitivity for detecting N2 disease is considerably lower in this group. The lower sensitivity of PET in these patients may indicate the need for more extensive use of invasive mediastinal lymph node diagnostics.
The strength of our study lies in its large cohort size, the largest published to date, and the use of standardized imaging and pathological protocols across all analyzed patients. Moreover, the distribution of histological cancer types, with 79% adenocarcinoma (AC) and squamous cell carcinoma (SCC), is representative of that commonly observed in thoracic surgical practice.
Limitations of the study
The main limitation of this study is its retrospective design. In addition, the study cohort consisted of patients from a single institution, which may not fully represent the diversity of patient demographics, disease characteristics, and treatment practices observed across different healthcare settings and populations. Further prospective multicenter studies with larger patient cohorts are warranted to confirm our findings and identify potential factors affecting PET performance.
Conclusions
Our study confirms that higher SUVmax of the primary tumor correlates with improved PET diagnostic performance in assessing mediastinal lymph node metastasis. However, when the primary tumor SUVmax values are below 15, N2 assessment should be approached with greater caution, as sensitivity for detecting N2 disease in this group is significantly lower. Positron emission tomography demonstrated a high NPV, making it valuable for ruling out N2 metastasis. Additionally, clinical variables such as age, BMI, sex, tumor location, and histological type did not significantly influence the risk of FN results. Further research is needed to better understand these phenomena and optimize imaging protocols, thereby improving clinical outcomes in patients with lung cancer.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.16977760. The package contains the following files:
Supplementary Table 1. Box–Tidwell test.
Supplementary Table 2. Variance inflation factor (VIF).
Supplementary Table 3. Cooks’s distance.
Data Availability Statement
The datasets supporting the findings of this study are not publicly available due to ethical and privacy restrictions related to sensitive patient information. Although the data have been anonymized, they contain health information protected under privacy laws and unrestricted public sharing could risk patient confidentiality and lead to misuse by unauthorized third parties. The data are available from corresponding author upon reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.