Abstract
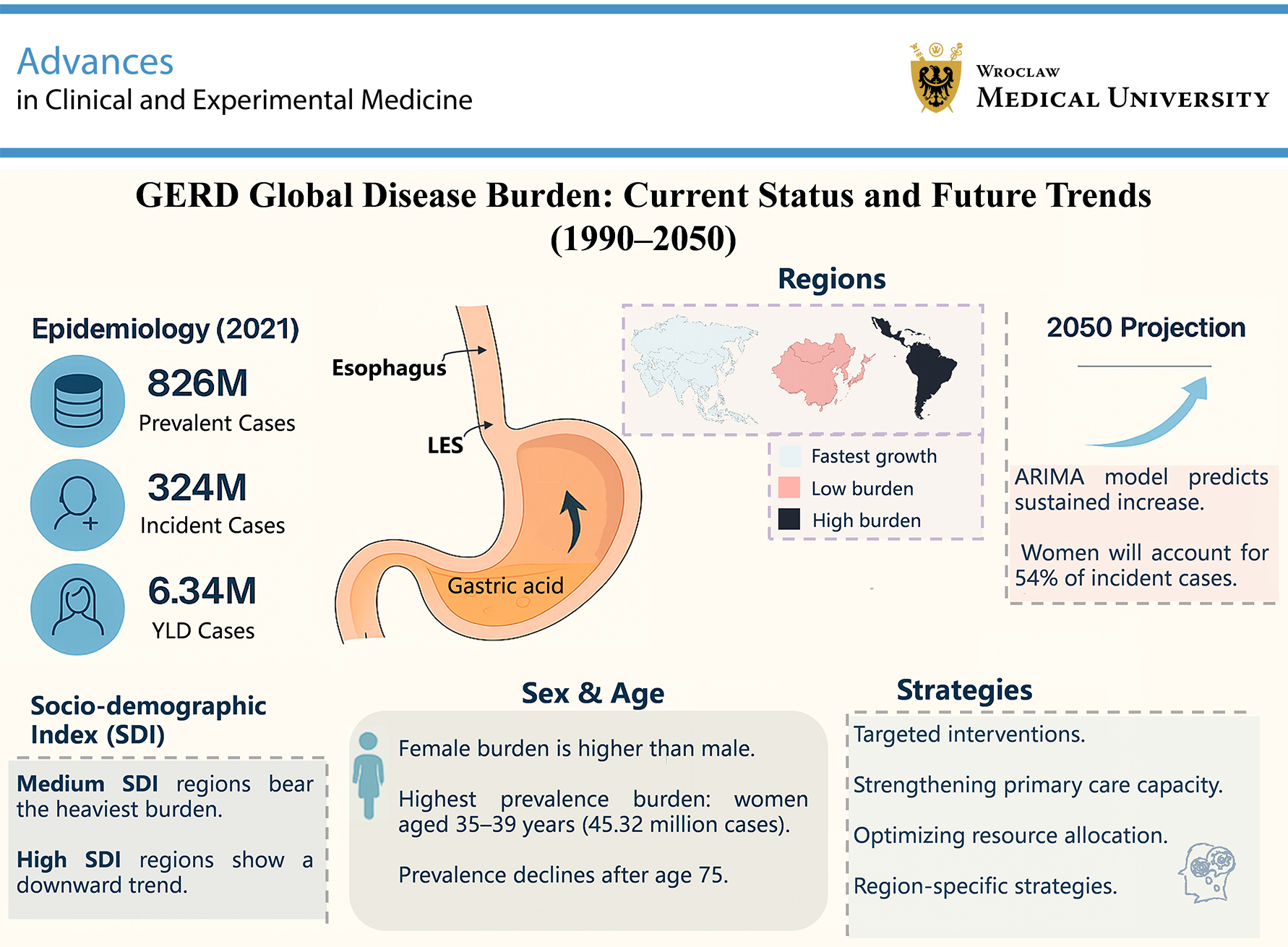
Gastroesophageal reflux disease (GERD) is a common digestive system disorder encountered in clinical practice. In recent years, the prevalence of GERD has increased, substantially affecting patients’ daily lives. This study aimed to address this issue by leveraging data from the Global Burden of Disease (GBD) 2021 database to systematically evaluate the burden and epidemiological characteristics of GERD and to predict trends in GERD burden from 2022 to 2050. We comprehensively analyzed the burden of GERD from 1990 to 2021, evaluated years lived with disability (YLDs), prevalence and incidence rates, and conducted stratified analyses according to geographical region, Sociodemographic Index (SDI), sex, and age groups ranging from 0 to 95 years. Globally, in 2021, there were 324 million (95% uncertainty interval (95% UI): 287.7–358.9 million) incident cases, 826 million (95% UI: 733–926 million) prevalent cases, and 6.34 million (95% UI: 3.19–11.24 million) YLDs attributable to GERD. Among individuals aged 0–95 years, women aged 35–39 years had the highest prevalence, estimated at 45.32 million (95% UI: 32.92–61.05 million). The burden was highest in middle-SDI regions and lowest in high-SDI regions. Predictions using autoregressive integrated moving average (ARIMA) modeling indicated that the global burden of GERD will continue to increase from 2022 to 2050, posing increasingly severe challenges to global healthcare systems, particularly among women. It is projected that by 2050, women will account for 54% of new cases.
Key words: epidemiology, gastroesophageal reflux, Global Burden of Disease
Introduction
Gastroesophageal reflux disease (GERD) is a prevalent gastrointestinal disorder worldwide, pathologically defined by the retrograde flow of gastric contents into the esophagus, oropharynx, or pulmonary system. Clinical manifestations include typical symptoms (heartburn and acid regurgitation) as well as atypical extraesophageal presentations, including laryngitis, chronic cough, and asthma exacerbations. The disease exhibits a bimodal age distribution, affecting both pediatric and adult populations. In children aged <8 years, GERD primarily manifests as feeding refusal, recurrent vomiting, and pulmonary complications (chronic cough and recurrent pneumonia), whereas older children (>8 years) and adolescents typically present with adult-type symptoms such as epigastric pain, nocturnal cough, and wheezing.1, 2
Endoscopic classification distinguishes 2 phenotypes: erosive esophagitis (EE; 30% prevalence), characterized by mucosal breaks (Los Angeles Grade A–D), and nonerosive reflux disease (NERD; 60–70% prevalence), characterized by intact mucosa despite symptomatic reflux.3 Barrett’s esophagus (BE) is a specific form of GERD characterized by replacement of the squamous epithelium in the lower esophagus with metaplastic columnar epithelium. Patients with BE may experience reflux symptoms, and some may also present with dysphagia and retrosternal pain, although a significant proportion remains asymptomatic. Barrett’s esophagus is one of the major complications of GERD and the only recognized precancerous lesion of esophageal adenocarcinoma (EAC).4, 5
The epidemiological burden of GERD is greater among individuals aged ≥50 years, smokers, users of nonsteroidal anti-inflammatory drugs (NSAIDs), and patients with obesity.6, 7 Research has shown that the diagnosis, treatment, and cancer surveillance associated with GERD impose considerable economic and psychological burdens. Currently, several studies have analyzed the epidemiological burden of GERD in different regions based on the Global Burden of Disease (GBD) 2017 and GBD 2019 databases. However, these studies often rely on relatively outdated data and still lack analyses stratified by sex and age groups, as well as projections of disease trends over the next 30 years.8, 9 Given the dynamic changes in the burden of GERD over time, it is important to promptly understand the current epidemiological status of GERD and monitor its changing trends. This knowledge is crucial for developing effective intervention strategies and policies at the global, regional, and national levels.
To provide comparable and up-to-date information on the burden of GERD, this study used the latest GBD 2021 data to analyze the incidence, prevalence, and years lived with disability (YLDs) of GERD across different regions, sexes, and age groups worldwide. In addition, the incidence of GERD from 2022 to 2050 was projected to provide a reference for public health interventions and policy development in different countries and regions and to support further basic research and clinical practice related to GERD.
Materials and methods
Data source
The GBD 2021 database expands epidemiological surveillance of GERD across 811 subnational regions in 204 countries. All data resources were obtained from the GBD Results Tool (http://ghdx.healthdata.org/gbd-results-tool) of the Global Health Data Exchange (GHDX) platform, maintained by the Institute for Health Metrics and Evaluation (IHME; Washington, D.C., USA). The diagnosis of GERD was classified according to the 10th revision of the International Classification of Diseases (ICD-10) using codes R12.11, K21–K21.9, and K22.7–K22.719.10 Age-standardized rate estimates and counts per 100,000 population are presented according to the GBD standard population structure.
Within the GBD framework, 95% uncertainty intervals (95% UIs) are provided for all estimates. Final estimates were calculated as the mean of 1,000 estimates obtained through sampling, with the lower and upper 95% UIs corresponding to the 2.5th and 97.5th percentiles, respectively, among the 1,000 samples.11 Confidence intervals (CIs) were calculated based on standard errors (SEs) under the assumption of a normal distribution. Confidence intervals are used to quantify uncertainty surrounding the estimation of a single model parameter and are commonly applied to assess the statistical significance of trends. Accordingly, in GBD studies, UIs are used to characterize the magnitude of disease burden estimates, whereas CIs are applied to evaluate changes in disease burden trends over time.
Additionally, the Sociodemographic Index (SDI), a composite measure of income, education, and fertility reflecting the level of sociodemographic development in a country or territory, was used. The SDI incorporates 5 levels based on SDI quintiles: low, low-middle, middle, high-middle, and high. The GBD data are available for 20 nonoverlapping 5-year age groups, ranging from under 5 years to over 95 years.
Trend analysis
We explored the temporal trends in the global burden of GERD from 1990 to 2021 according to age group, sex, SDI, GBD region, and country, and estimated the estimated annual percentage change (EAPC) using a linear regression model. Based on the EAPC values, we assessed disease burden trends in each GBD region and identified regions with similar patterns of disease burden change.12
Predictive analysis
To better inform public health policy and healthcare resource allocation, we further projected the global burden of GERD through 2050. Autoregressive Integrated Moving Average (ARIMA) models are statistical models commonly used for time-series analysis and forecasting.13 These models capture the characteristics of time-series data and predict disease trends over the next 30 years by combining autoregressive (AR), differencing (I), and moving average (MA) components.
Results
Trends in the incidence of GERD in 2021
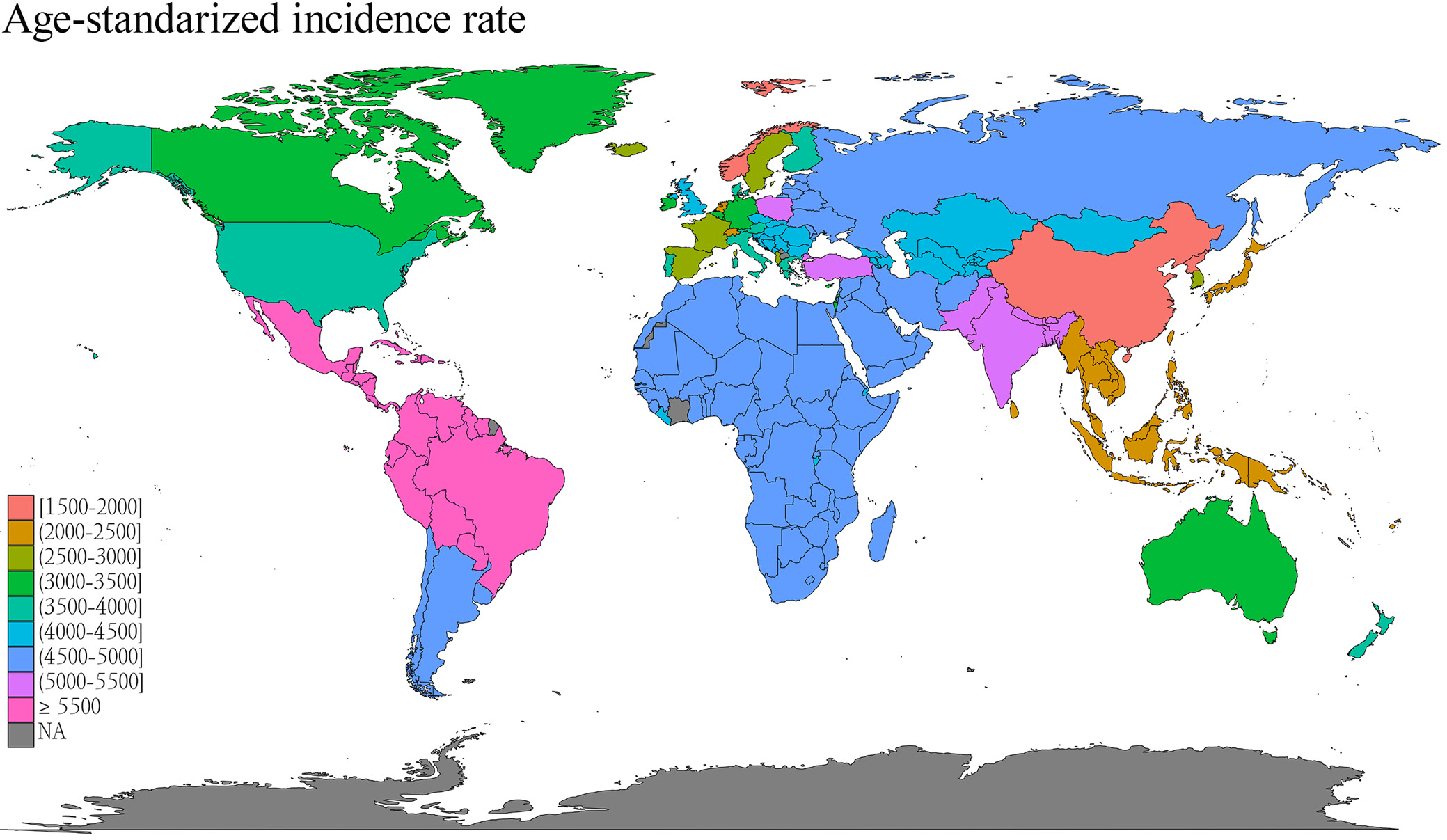
In 2021, the global number of incident cases reached 324 million (95% UI: 288–359 million), reflecting an 80% increase from 1990. After adjustment for age structure, the global age-standardized incidence rate (ASIR) increased from 3,740 per 100,000 population (95% UI: 3,314–4,142) in 1990 to 3,882 per 100,000 (95% UI: 3,446–4,300) in 2021, with an EAPC of 0.36 (95% CI: 0.29–0.43).
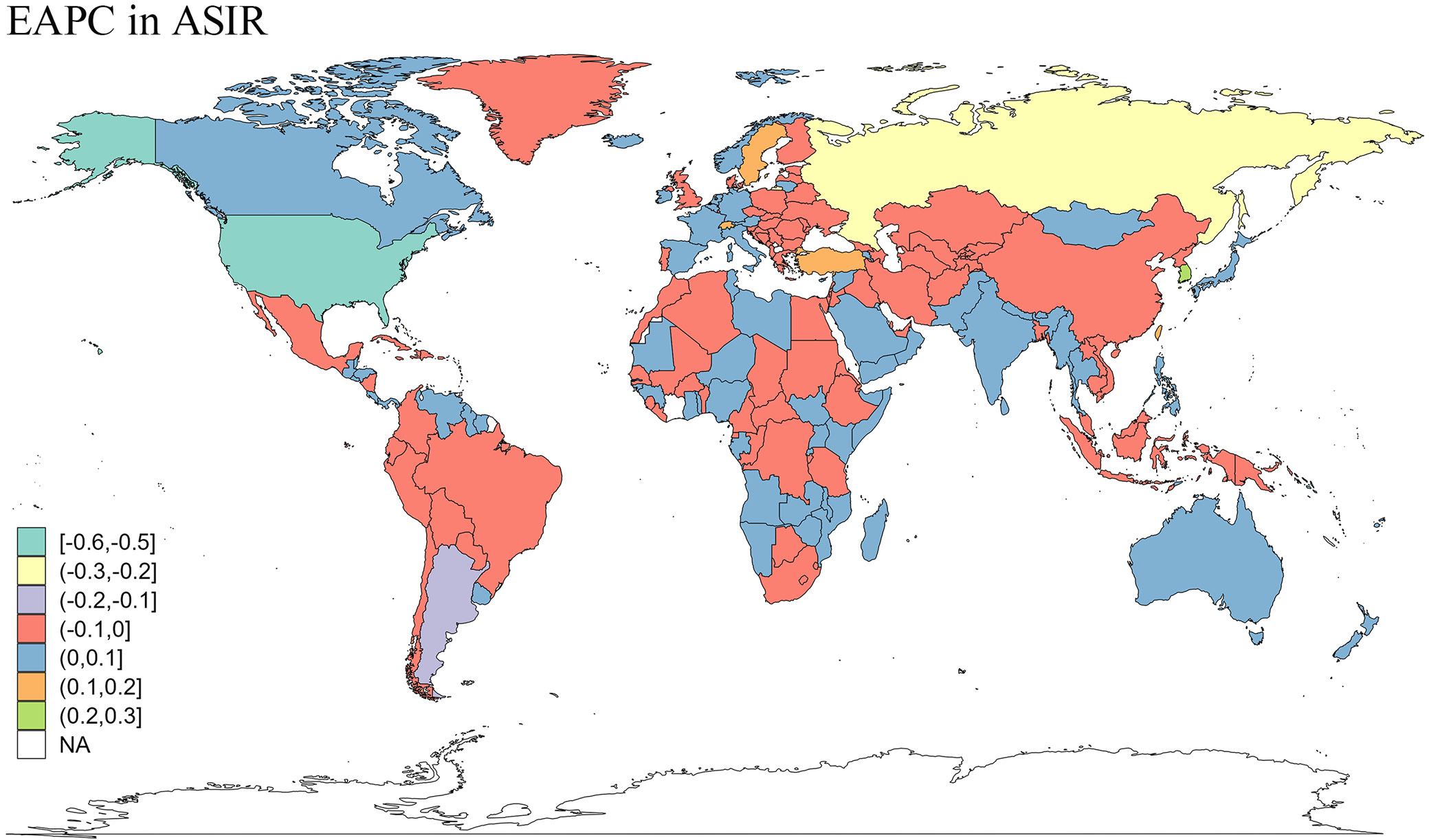
The SDI-stratified analysis revealed declining trends in high-SDI (EAPC = −0.13; 95% CI: −0.20 to −0.06), high-middle SDI (EAPC = −0.23; 95% CI: −0.30 to −0.15), and low-SDI regions (EAPC = −0.01; 95% CI: −0.01 to −0.01), whereas middle-SDI regions exhibited an increasing trend (EAPC = 0.28; 95% CI: 0.26–0.31).
Regionally, ASIRs varied widely, ranging from 6,248 per 100,000 (95% UI: 5,568–6,875) in Tropical Latin America to 1,850 per 100,000 (95% UI: 1,610–2,090) in East Asia, with the highest incidence rates (>6,000 per 100,000) observed in Latin America (Tropical Latin America, Central Latin America, and Andean Latin America) and the Caribbean. In contrast, the lowest rates (<3,000 per 100,000) were found in East Asia, the Western Pacific region, Oceania, Southeast Asia, and High-Income Asia Pacific. Notably, Asia (EAPC = 0.60; 95% CI: 0.50–0.70) and High-Income Asia Pacific (EAPC = 0.50; 95% CI: 0.15–0.86) experienced pronounced growth, contrasting with the decline observed in High-Income North America (EAPC = −0.30; 95% CI: −0.55 to −0.06).
At the national level, the highest burdens were observed in India (76,322,880; 95% UI: 67,266,798–84,678,866), China (32,387,866; 95% UI: 27,851,900–36,711,150), and the USA (16,021,759; 95% UI: 14,111,407–17,823,288). The 3 countries with the lowest ASIRs in 2021 were Norway (1,838.34; 95% UI: 1,582.47–2,072.53), China (1,844.31; 95% UI: 1,605.06–2,084.12), and North Korea (1,927.59; 95% UI: 1,683.71–2,178.28), while the highest ASIRs were observed in Brazil (6,249.93; 95% UI: 5,569.09–6,875.72), Mexico (6,219.29; 95% UI: 5,559.67–6,822.16), and Paraguay (6,177.95; 95% UI: 5,528.53–6,806.60). National-level heterogeneity was evident in EAPC patterns: the Maldives (0.89; 95% CI: 0.56–1.22), South Korea (0.84; 95% CI: 0.55–1.13), and Iran (0.71; 95% CI: 0.48–0.93) exhibited significant increases, while the USA showed a marked decline (−0.35; 95% CI: −0.60 to −0.10) (Supplementary Table 1 and Figure 1, Figure 2).
Trends in the prevalence of GERD in 2021
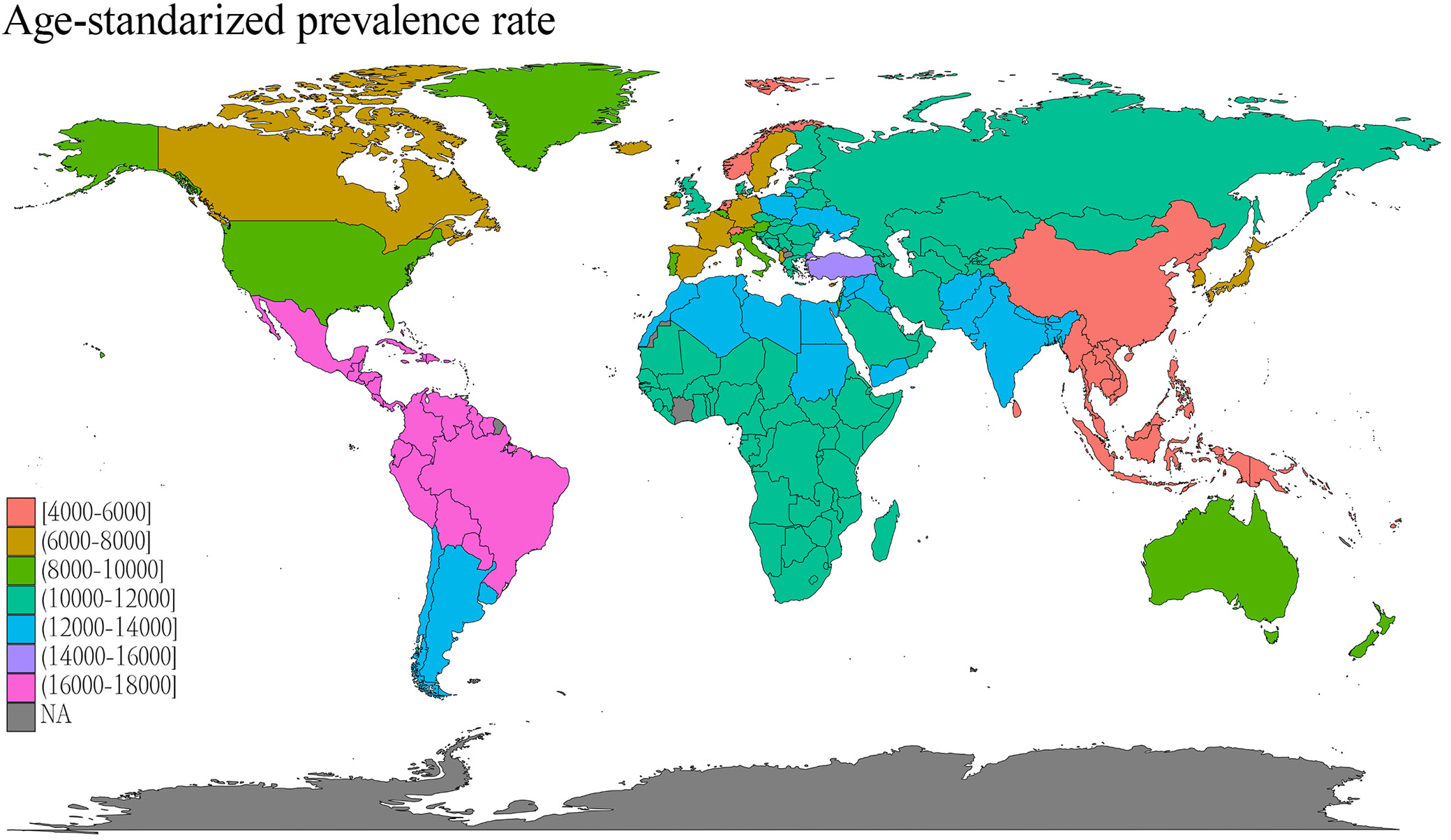
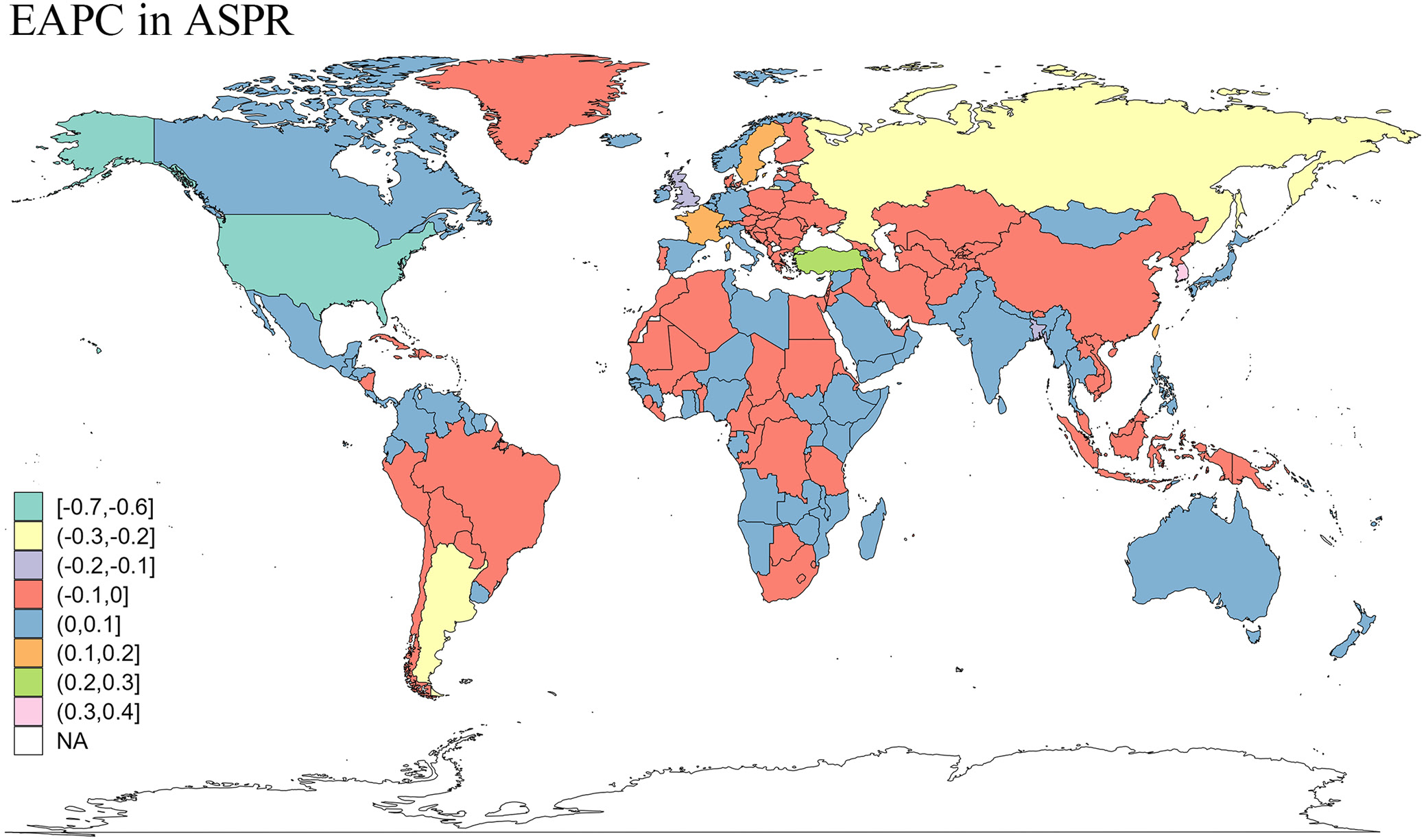
The total number of prevalent GERD cases worldwide increased from 450 million in 1990 to 830 million in 2021, while the age-standardized prevalence rate (ASPR) showed a more modest increase, from 9,516.49 per 100,000 population (95% UI: 8,427.33–10,664.72) in 1990 to 9,838.60 per 100,000 (95% UI: 8,732.46–11,056.05) in 2021. Among SDI regions, high- and high-middle-SDI regions exhibited a decline in ASPR, whereas only middle-SDI regions demonstrated an increase, with an EAPC of 0.27 (95% CI: 0.24–0.30).
In 2021, the highest ASPR was observed in Tropical Latin America (16,681.34 per 100,000 population; 95% UI: 14,832.41–18,433.23), followed by Central Latin America (16,429.42 per 100,000 population; 95% UI: 14,570.23–18,291.39), the Caribbean (16,408.86 per 100,000 population; 95% UI: 14,498.52–18,308.49), and Andean Latin America (16,405.98 per 100,000 population; 95% UI: 14,495.47–18,306.62). The highest ASPRs at the national level were observed in Paraguay (16,774.68; 95% UI: 14,835.88–18,709.59) and Brazil (16,678.10; 95% UI: 14,840.12–18,432.84), whereas the lowest ASPRs were observed in China (4,540.66 per 100,000 population; 95% UI: 3,950.76–5,156.56) and Norway (4,330.94 per 100,000 population; 95% UI: 3,783.45–4,956.78). South Korea exhibited the most significant upward trend in ASPR (EAPC: 1.00; 95% CI: 0.68–1.33), while the USA showed a declining trend (EAPC: −0.49; 95% CI: −0.77 to −0.21) (Supplementary Table 2 and Figure 3, Figure 4).
Trends in the YLDS of GERD in 2021
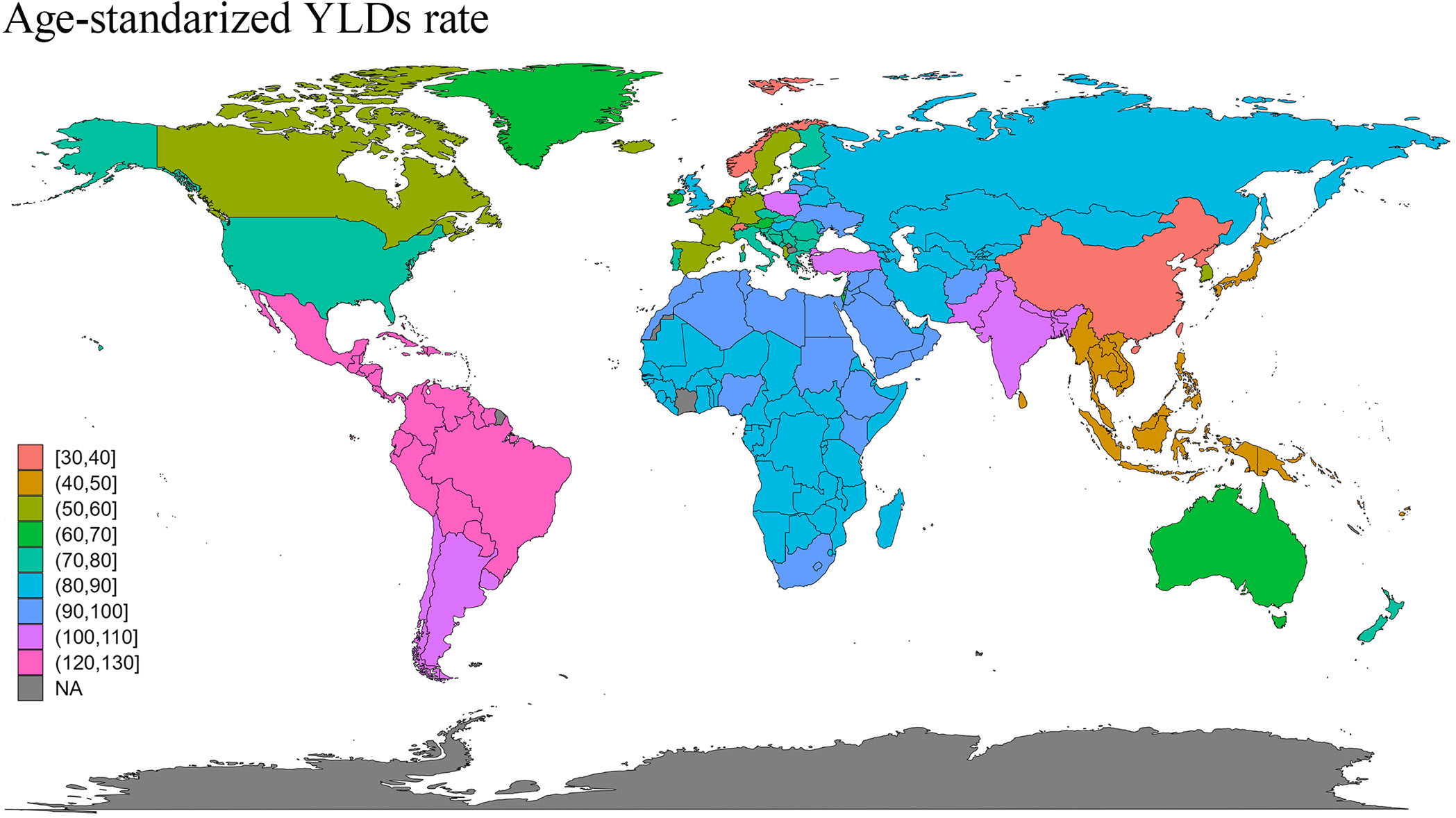
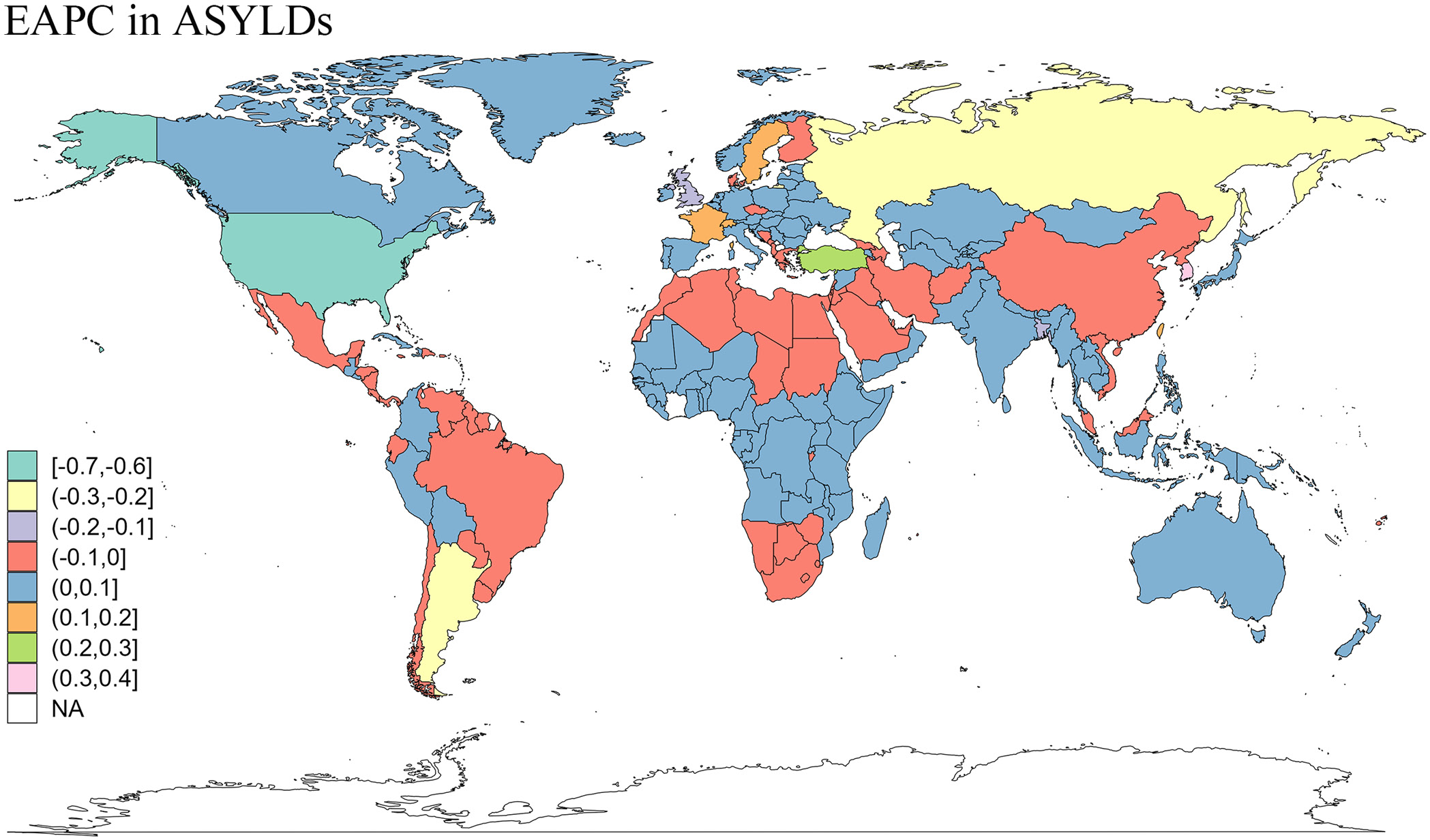
During the period from 1990 to 2021, the age-standardized years lived with disability (ASYLDs) rate exhibited a gradual upward trend, increasing from 73 cases per 100,000 population (95% UI: 36.75–129.66) in 1990 to 75.56 cases per 100,000 population (95% UI: 38.05–133.87) in 2021, with an EAPC of 0.37% (95% CI: 0.29–0.45). Gender-specific analysis revealed that the ASYLDs rate increased from 70.37 (95% UI: 35.3–125.34) and 75.62 (95% UI: 38.18–133.94) cases per 100,000 population in 1990 to 72.95 (95% UI: 36.6–129.73) and 78.14 (95% UI: 39.48–137.95) cases per 100,000 population in 2021 for men and women, respectively, with a more pronounced upward trend observed in men.
Geospatial analysis demonstrated heterogeneous temporal patterns across different SDI regions and geographical areas. While low-middle-SDI regions, African regions (Central, Eastern, Southern, and Western), Australia, Eastern Europe, and the Oceania region showed nonsignificant trends, high-SDI regions (−0.19; 95% CI: −0.27 to −0.10), high-middle-SDI regions (−0.23; 95% CI: −0.31 to −0.16), and North America (−0.46; 95% CI: −0.74 to −0.19) exhibited significant improvements in ASYLDs (EAPC < 0%). Conversely, Southeast Asia, South Asia, Central Latin America, High-Income Asia Pacific, and Andean Latin America showed significant increases in disease burden.
At the national level, South Korea (0.99; 95% CI: 0.67–1.31), the Maldives (0.99; 95% CI: 0.63–1.35), Iran (0.78; 95% CI: 0.53–1.03), Saint Lucia (0.74; 95% CI: 0.55–0.92), Turkey (0.74; 95% CI: 0.61–0.87), and Libya (0.73; 95% CI: 0.47–0.98) demonstrated substantial increases in GERD-related burden. In contrast, the USA showed a significant improvement trend (−0.52; 95% CI: −0.79 to −0.24) (Supplementary Table 3 and Figure 5, Figure 6).
The trends of the incidence, prevalence, and YLDs of GERD in different gender-age groups
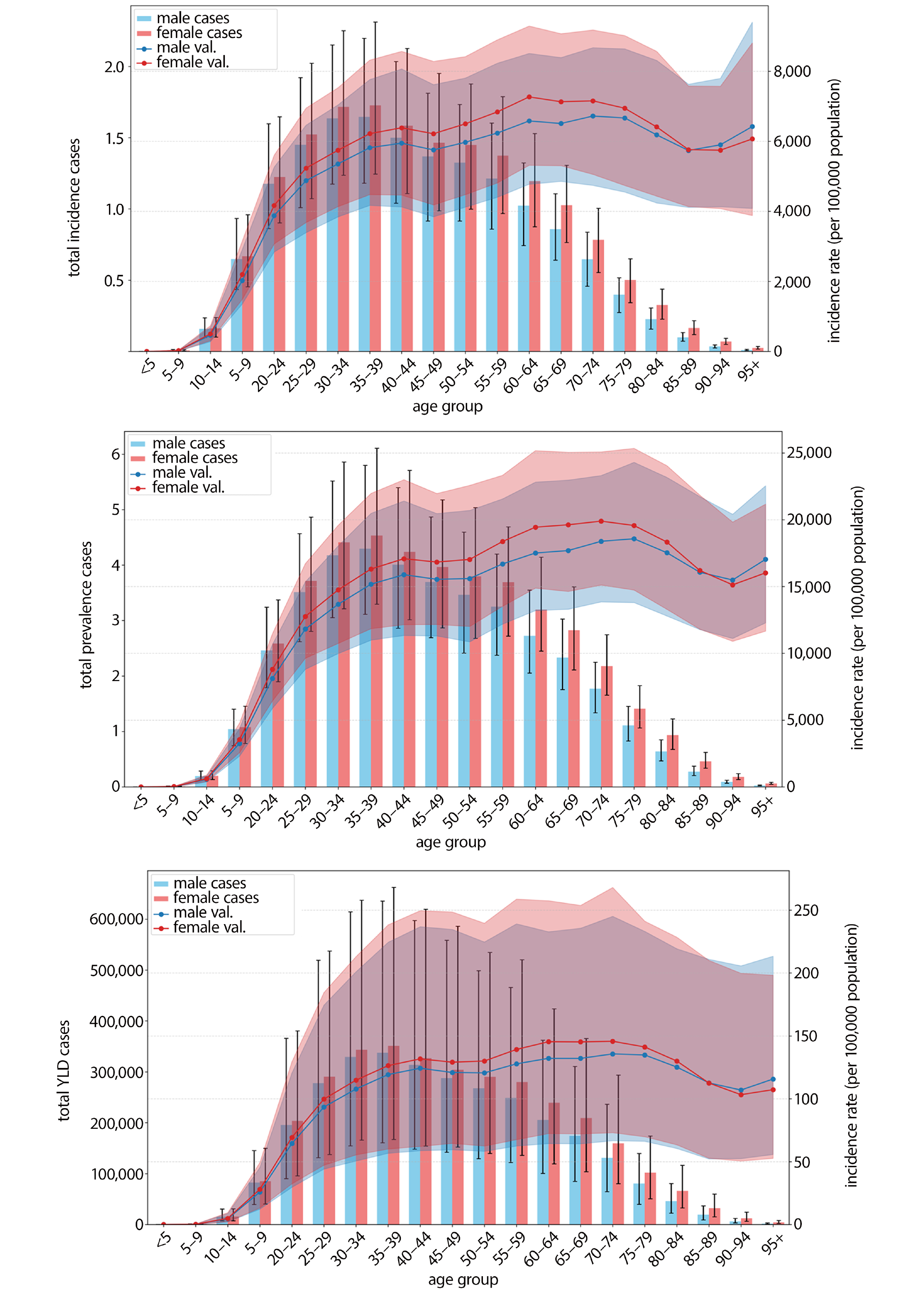
In the global cohort aged 0–95 years in 2021, the 35–39-year age group exhibited the highest burden of GERD. Women within this demographic reached peak values for incident cases (17,272,298 cases), prevalent cases (45,317,937 cases), and YLDs (351,061 cases). Concurrently, men in this age group reached the highest values across all age groups for incident cases (16,463,111 cases), prevalent cases (42,955,218 cases), and YLDs (337,582 cases). Notably, women consistently demonstrated higher prevalence, incidence, and YLDs than men across all age groups.
Age-specific incidence rates progressively increased, reaching an initial peak at ages 40–44 years, followed by a decline. This trend reversed after age 50, reaching a secondary peak at ages 60–64 years. After age 65, incidence rates demonstrated a sustained decline, although a resurgence was observed beyond age 89, with men exhibiting higher incidence rates than women during this geriatric phase. Age-specific prevalence peaked at ages 70–74 years, subsequently declined, and showed a secondary resurgence at ages 90–94 years. The YLD rates remained relatively stable from ages 40–84 years, peaking at ages 70–74 years. A sex-specific crossover phenomenon was observed: women maintained higher YLD rates until age 85, beyond which male rates predominated (Figure 7).
Global prediction model for the burden of GERD from 2022 to 2050 (based on ARIMA)
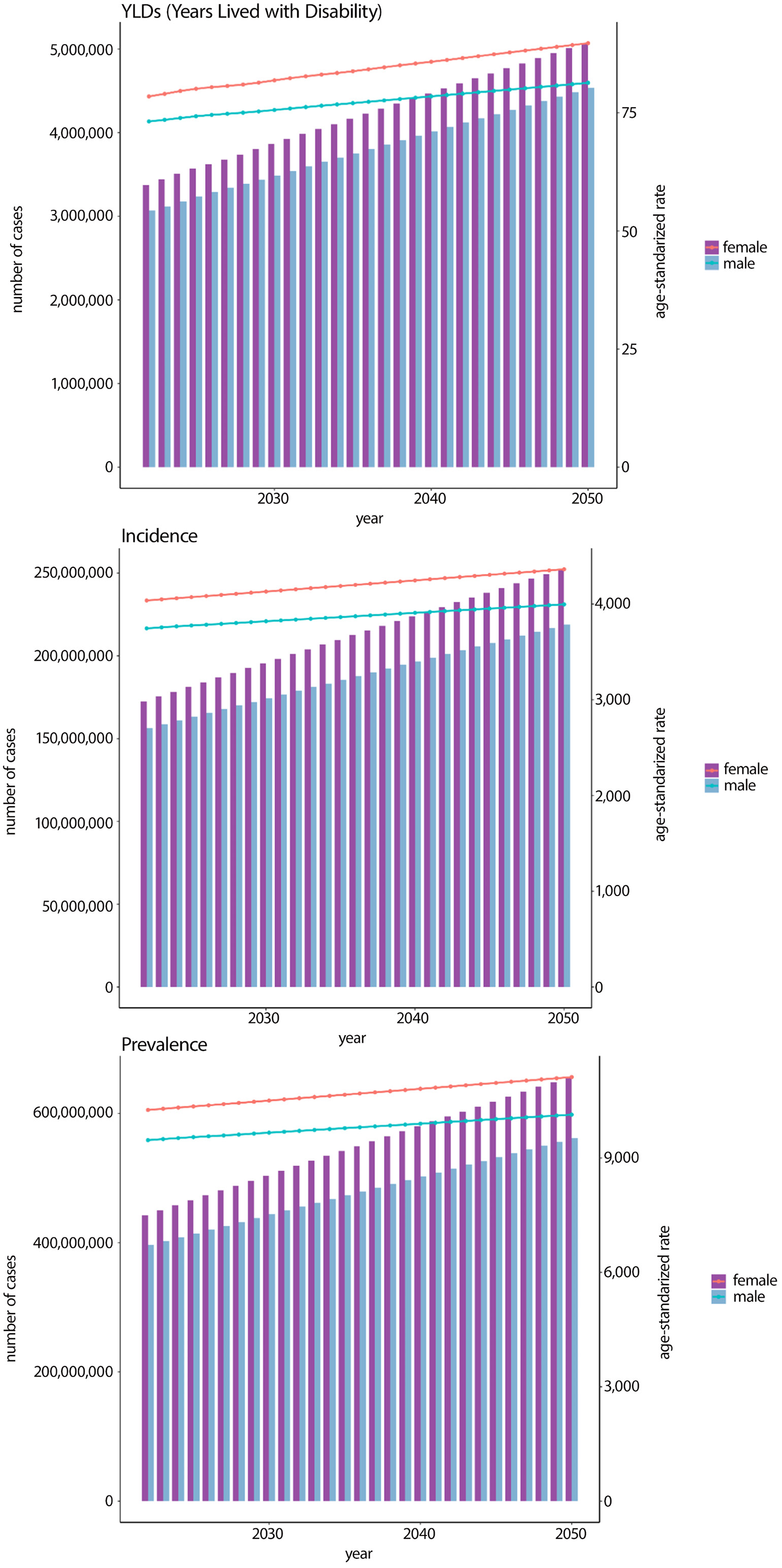
The model predicts a sustained increase in incidence, prevalence, and YLDs for both sexes during this period. Specifically, the total number of incident cases is projected to exceed 200 million by 2032 among women and by 2042 among men. By 2050, the ASIR is expected to rise to 4,363 per 100,000 population for women and 3,996 per 100,000 population for men. Similarly, the number of prevalent cases among women is projected to surpass 600 million by 2043, with the ASPR reaching 11,121 per 100,000 for women and 10,135 per 100,000 for men by 2050. Furthermore, the ASYLD rate is anticipated to increase to 90 per 100,000 for women and 81 per 100,000 for men by 2050, reflecting a growing burden of disability attributable to GERD (Figure 8).
Discussion
Our study provides the most recent estimates of the global burden of GERD across 204 countries based on the GBD 2021 study. By systematically evaluating incidence, prevalence, and YLDs at global, national, and subnational levels – stratified by SDI quintiles, sex, and age groups – we found that in 2021 there were 324 million incident cases, 826 million prevalent cases, and 6.34 million YLDs attributable to GERD worldwide. The burden exhibited significant geographical heterogeneity: ASIRs and ASPRs were highest in Tropical Latin America and lowest in East Asia, a disparity potentially driven by regional variations in dietary patterns, obesity prevalence, alcohol and tobacco consumption, and population aging.3, 14 Meanwhile, socioeconomic disparities markedly influenced GERD burden, with low- to middle-SDI regions exhibiting the highest ASIRs, ASPRs, and ASYLDs compared with other SDI quintiles, likely reflecting inequities in healthcare access, diagnostic delays, and suboptimal management of chronic conditions. Furthermore, common digestive disorders such as celiac disease may present with symptoms overlapping those of GERD, including abdominal discomfort and reflux-like sensations, which can complicate differential diagnosis and potentially lead to misdiagnosis of GERD or overestimation of its incidence in certain populations.15 Additionally, NSAIDs and corticosteroids have been shown to exacerbate GERD by impairing esophageal sphincter function, reducing mucosal protection, and increasing gastric acid secretion. The risk of reflux symptoms increases one-to-twofold among long-term users. These underrecognized factors may contribute to the continuous rise in GERD incidence, and the projected burden is expected to increase further by 2050. This highlights the need for targeted preventive measures. Future research should integrate detailed data on comorbidities and pharmacological treatments to improve prediction accuracy.
Our analysis yielded the following principal findings. First, the ASIR, ASPR, and ASYLDs associated with GERD exhibited a consistent upward trajectory globally from 1990 to 2021, underscoring the escalating disease burden. These epidemiological patterns align with findings from previous studies published in 2017 and 2019, confirming the persistent temporal progression of GERD-related health impacts. Geospatial analysis revealed distinct regional variations, with the highest ASIR estimates observed in Brazil, Mexico, and Paraguay, while ASPR peaked in Paraguay, Brazil, and El Salvador.
Notably, divergent temporal patterns emerged between 2019 and 2021, with Asia and High-Income Asia Pacific regions demonstrating accelerated growth rates in disease metrics, in contrast to the declining trend observed in High-Income North America. This epidemiological divergence suggests that, beyond universal drivers such as population growth and aging, region-specific determinants – including dietary patterns, obesity prevalence, and healthcare accessibility – may modulate GERD burden dynamics. Numerous studies have also shown that obesity and overweight increase intra-abdominal pressure, weaken the lower esophageal sphincter, and exacerbate reflux, thereby directly contributing to increased GERD incidence.16, 17
Furthermore, we identified a significant disparity in disease burden, with disproportionately higher impacts observed in socioeconomically disadvantaged regions characterized by limited healthcare resource allocation and constrained diagnostic capacity, which is consistent with previous findings.9, 18 Finally, projection modeling using ARIMA algorithms predicts a sustained global increase in both prevalence rates and incidence counts from 2022 to 2050, signaling an urgent need for targeted public health interventions.
First, greater emphasis should be placed on promoting healthy dietary patterns, smoking and alcohol control policies, and obesity management strategies in high-burden regions such as Tropical Latin America. Second, healthcare capacity at the primary care level in low- and middle-SDI regions should be strengthened through the implementation of low-cost diagnostic tools and improved access to treatment. Optimization of healthcare resource allocation and expansion of telemedicine and digital health tools may improve diagnostic accessibility in remote areas, shorten diagnostic delays, and improve chronic reflux management, thereby reducing progression to severe complications. Third, regional epidemiological surveillance and dynamic monitoring systems should be strengthened to track changes in disease burden. In regions with rapidly increasing rates, such as Asia and High-Income Asia Pacific, GERD prevention strategies should be integrated into primary healthcare systems, with emphasis on early symptom recognition and lifestyle counseling. In regions with declining trends, such as High-Income North America, best practices in healthcare accessibility and standardized management could be shared to guide interventions in other regions. Finally, these measures should align with international GERD guidelines while being adapted to local socioeconomic conditions to ensure feasibility and equity across populations with different levels of socioeconomic development, thereby reducing the burden of GERD and narrowing regional disparities.
When assessing the severity of GERD, several high-risk factors related to the occurrence and progression of the disease, such as age, race, and sex, should be taken into account. Our research found that the 35–39-year age group exhibited the highest burden of GERD. Previous studies have shown that psychological factors play an important role in the pathogenesis of GERD.19 Psychological stress can increase both the perception of heartburn and the severity of GERD symptoms.20 Fass et al. indicated that acute stress can enhance esophageal sensitivity to acid exposure in patients with reflux esophagitis or GERD.21 Individuals aged 35–39 often face multiple stressors, including career advancement, mortgage obligations, and raising children. Emotional conditions such as anxiety and depression may lead to irregular eating habits, overeating, and increased smoking and alcohol consumption, thereby increasing the incidence of GERD.
This study found that the prevalence of GERD peaked at ages 70–74 years and subsequently declined. The decline in prevalence after age 75 may reflect the combined effects of “selective survival bias” and “physiological or diagnostic changes.”22 First, GERD is closely associated with several risk factors, such as severe obesity, smoking, and poorly controlled comorbidities, which also increase mortality related to cardiovascular disease (CVD), cancer, and other age-related conditions. Patients with these high-risk characteristics may die before the age of 75, resulting in a “pseudo-decline” in GERD prevalence among individuals surviving to older ages. Second, aging-related reductions in esophageal sensory perception and sensitivity may decrease symptom severity or awareness in elderly individuals, leading to underreporting of GERD diagnoses. Third, individuals older than 75 years often experience multiple comorbidities, such as CVD and dementia, which may divert healthcare attention and contribute to underdiagnosis of GERD symptoms in epidemiological data.
To date, research on the incidence and prevalence of GERD remains limited. For instance, a systematic review by Singendonk et al. estimated that GERD affects approx. 23–40% of pediatric populations.23 In contrast to earlier findings, the GBD 2019 database and a study by Nirwan et al. identified China as having the lowest ASPR for GERD, whereas the latest GBD 2021 data indicate that Norway now has the lowest ASPR.24, 25 Notably, our analysis revealed significant improvements in ASIRs, ASPRs, and ASYLDs in North America. Consistent with previous research, the burden of GERD is closely associated with the SDI. Although high-fat and high-sugar diets in regions such as North America may elevate obesity rates and consequently increase GERD risk, greater health awareness, adequate healthcare resources, and standardized diagnostic and monitoring protocols appear to effectively mitigate GERD incidence.26, 27
Limitations of the study
Our study has several limitations, the most significant of which is the scarcity of data in many regions. Although the analysis of GERD incorporated prevalence and incidence data from a total of 204 location-years, this is substantially fewer than the data available for other chronic conditions such as diabetes and coronary heart disease. The limited availability of data constrains the precision of regional burden estimates, particularly in understudied or data-deficient areas. To address this gap, future iterations of the GBD study should prioritize inclusion of additional high-quality data sources, with a specific focus on underrepresented regions.
Meanwhile, GERD is a heterogeneous disease with a wide range of symptoms and complications. The incidence estimates in this study reflect “clinically diagnosed GERD”; however, GERD may be underreported because of the presence of atypical manifestations. Future research should therefore consider including atypical symptoms and complications of GERD, such as erosive esophagitis, BE, and stenosis, as well as hospitalization rates related to complications and proton pump inhibitor (PPI) use or prescription as supplementary indicators. These revisions may enhance the transparency, scope, and clinical relevance of the analyzed data. Furthermore, there is a critical need for more granular data on GERD incidence, prevalence, severity, and frequency across different age groups, particularly in regions where such data are currently sparse or absent.
Conclusions
Our study demonstrates a substantial increase in the global burden of GERD from 1990 to 2021. Projections indicate that this burden will continue to increase from 2022 to 2050, imposing substantial strain on healthcare systems worldwide, especially among female populations. Middle- and lower-middle-SDI regions consistently exhibit disproportionately high GERD burdens compared with high-income regions. To address these challenges, future efforts must prioritize implementation of precision diagnostic protocols and evidence-based interventions tailored to regional epidemiological profiles. Multifaceted strategies, including enhanced surveillance systems, equitable access to PPIs, and community-based education regarding lifestyle modifications, are critical to mitigating GERD-related complications and reducing the growing impact of GERD on global health equity.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.17132213. The package contains the following files:
Supplementary Table 1. Incidence of GERD in 2021 for both sexes and all locations, with EAPC from 1990 and 2021.
Supplementary Table 2. Prevalence of GERD in 2021 for both sexes and all locations, with EAPC from 1990 and 2021.
Supplementary Table 3. YLDs of GERD in 2021 for both sexes and all locations, with EAPC from 1990 and 2021.
Use of AI and AI-assisted technologies
Not applicable.