Abstract
Background. Given that long-term anticoagulant therapy is required in many clinical scenarios, continuous safety monitoring of direct factor Xa inhibitors is of great importance. To date, the renal safety of these agents remains a subject of debate.
Objectives. The aim of this study was to assess the association between direct factor Xa inhibitors and acute kidney injury (AKI) using data from the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS).
Materials and methods. The study period extended from the first quarter of 2014 to the last quarter of 2024, and reports of adverse events (AEs) related to rivaroxaban and apixaban were extracted separately from FAERS. The association between direct factor Xa inhibitors and AKI was evaluated using disproportionality analysis methods.
Results. Rivaroxaban-associated AKI was more common in men, and the risk was higher among patients older than 65 years. Rivaroxaban showed a significant positive signal for AKI in patients older than 65 years, with a reported reporting odds ratio (ROR) of 3.82 (95% confidence interval (95% CI): 3.65–4.01), proportional reporting ratio (PRR) of 3.78, EBGM05 of 3.68, and IC025 of 1.88. In comparison, apixaban showed no significant risk signal, with an ROR of 0.86 (95% CI: 0.79–0.94), PRR of 0.86, EBGM05 of 0.86, and IC025 of −0.34. Acute kidney injury typically occurred at a median of 109 days after treatment initiation, with approx. 50% of cases occurring within the first 3 months. The main outcomes of AKI were hospitalization (56.06%) and death (37.67%).
Conclusions. Our findings suggest a significant association between rivaroxaban use and AKI in elderly patients. Clinical monitoring of renal function should be intensified in elderly patients receiving rivaroxaban. However, it should be emphasized that this study presents only disproportionality analysis results and cannot establish a causal relationship between rivaroxaban and AKI. Therefore, the findings should be interpreted with caution.
Key words: acute kidney injury, rivaroxaban, spontaneous reporting system, direct factor Xa inhibitors, disproportionality analysis
Background
Direct factor Xa inhibitors are widely used novel oral anticoagulants that exert their anticoagulant effects by directly and reversibly binding to coagulation factor Xa and inhibiting its activity without requiring a cofactor.1 Compared with traditional anticoagulants, direct factor Xa inhibitors offer a faster onset of action, more predictable anticoagulant effects, a wider therapeutic window, no requirement for routine monitoring, and fewer interactions with food and other medications.2 Currently, rivaroxaban and apixaban are the most commonly used agents in this class and have demonstrated particularly strong market performance. Since its approval, rivaroxaban has shown continuous global sales growth, reaching $6,568 billion in 2018. However, in recent years, its market share has been surpassed by apixaban, whose global sales reached $10,263 billion in the 1st half of 2023 alone, making it the 2nd best-selling drug worldwide.
Given that long-term anticoagulant therapy is required in many clinical settings, continuous safety monitoring of direct factor Xa inhibitors is of great importance. To date, the renal safety of these agents remains controversial. A case report described a patient receiving long-term rivaroxaban therapy who was found to have previously unrecognized glomerular disease.3 Marcelino et al. analyzed data from regulatory centers in 134 countries and found that rivaroxaban, apixaban, and edoxaban were associated with renal adverse events (AEs) in 3.5%, 2.0%, and 1.7% of cases, respectively.4 Among users of direct factor Xa inhibitors, acute kidney injury (AKI) is the most frequently reported renal AE, and severe cases may require renal replacement therapy.5, 6, 7, 8, 9, 10 A pharmacovigilance study based on the U.S. Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) identified a significant disproportionality signal between rivaroxaban and AKI.11
On the other hand, several studies have suggested potential renoprotective effects of these drugs. A meta-analysis indicated that rivaroxaban was associated with favorable renal outcomes in patients with diabetes and preexisting kidney disease, as well as in elderly populations and and Asian cohorts.12 In patients with nonvalvular atrial fibrillation and end-stage chronic kidney disease (CKD), rivaroxaban has been associated with a significantly lower incidence of major bleeding compared with warfarin.13 Furthermore, evidence suggests that direct factor Xa inhibitors are associated with a lower risk of AKI compared with warfarin.14
Against this background, further evaluation is needed to determine whether a potential safety signal exists between direct factor Xa inhibitors and AKI using real-world data. Pharmacovigilance is a key method for monitoring associations between drugs and AEs following market approval. The FAERS is a spontaneous reporting database that collects reports of suspected adverse drug reactions15, 16 and serves as an important source of information for post-marketing drug safety research.17
Objectives
To clearly illustrate the association between direct factor Xa inhibitors and kidney injury, this study comprehensively analyzed post-marketing kidney injury AEs associated with direct factor Xa inhibitors using real-world FAERS data. The study investigated the relationship between direct factor Xa inhibitors and kidney injury AEs and their influencing factors, compared differences in renal injury AEs between 2 direct factor Xa inhibitors, and aimed to provide a reference for their clinical use.
Materials and methods
Data source
This study was designed as an observational, retrospective, cross-sectional pharmacovigilance analysis covering the period from the 1st quarter of 2014 (Q1 2014)to the 4th quarter of 2024 (Q4 2024). Data were extracted from the FAERS, a publicly accessible large-scale spontaneous AE reporting database (https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html). As all data used in this study were anonymized and de-identified, ethical approval was not required.
Drug selection and adverse reaction definition
This study focused on 2 widely used direct factor Xa inhibitors, rivaroxaban and apixaban. To minimize potential confounding effects from concomitant medications, only reports in which rivaroxaban or apixaban was listed as the primary suspect drug were included. Reports involving co-medications were excluded. Adverse events in the FAERS database were defined using Preferred Terms (PTs) from v. 25.0 of the Medical Dictionary for Regulatory Activities (MedDRA; https://www.ich.org/page/meddra). We identified relevant AEs using the PT “acute kidney injury (AKI)” as the target keyword. Reports related to the target drugs were screened using both their generic and brand names. For each eligible report, we extracted basic information, including patient age, sex, report year, reporting country, indication, and clinical outcome. The time to onset (TTO) of AKI associated with direct factor Xa inhibitors was defined as the interval between EVENT_DT (event date) in the DEMO file and START_DT (start date of drug administration) in the THER file. Records were excluded if data were missing or inaccurate, or if the reported event occurred before the start of drug administration.
Statistical analyses
This study utilized a disproportionality analysis approach to evaluate the relative risk of AKI in patients treated with direct factor Xa inhibitors. By comparing the observed number of AE reports with the expected number, this method helps identify signals that may indicate an increased risk of adverse reactions and serves as a key tool for post-marketing drug safety surveillance. To improve the accuracy of signal detection, we employed several commonly used disproportionality measures, including reporting odds ratio (ROR),18 proportional reporting ratio (PRR),19 Bayesian Confidence Propagation Neural Network (BCPNN),20 and Multi-item Gamma Poisson Shrinker (MGPS).21 A signal was considered positive only if the predefined threshold criteria for all 4 algorithms were met. The specific mathematical formulas and evaluation criteria are detailed in Table 1. All disproportionality indicators were calculated based on 2 × 2 contingency tables, as presented in Table 2.
To assess the robustness of our findings, ibuprofen was selected as a positive control and insulin glargine as a negative control. Additionally, subgroup analyses were performed based on sex and age groups to enhance the interpretability and reliability of the results.
All data processing and statistical analyses were conducted using Microsoft Excel 2019 (Microsoft Corp., Redmond, USA) and R v. 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria). The primary R packages used for data cleaning, analysis, and visualization included “desc”, “tidyverse”, “table1”, “openxlsx”, “data.table”, “dplyr”, and “ggplot2”.
Results
Basic characteristics
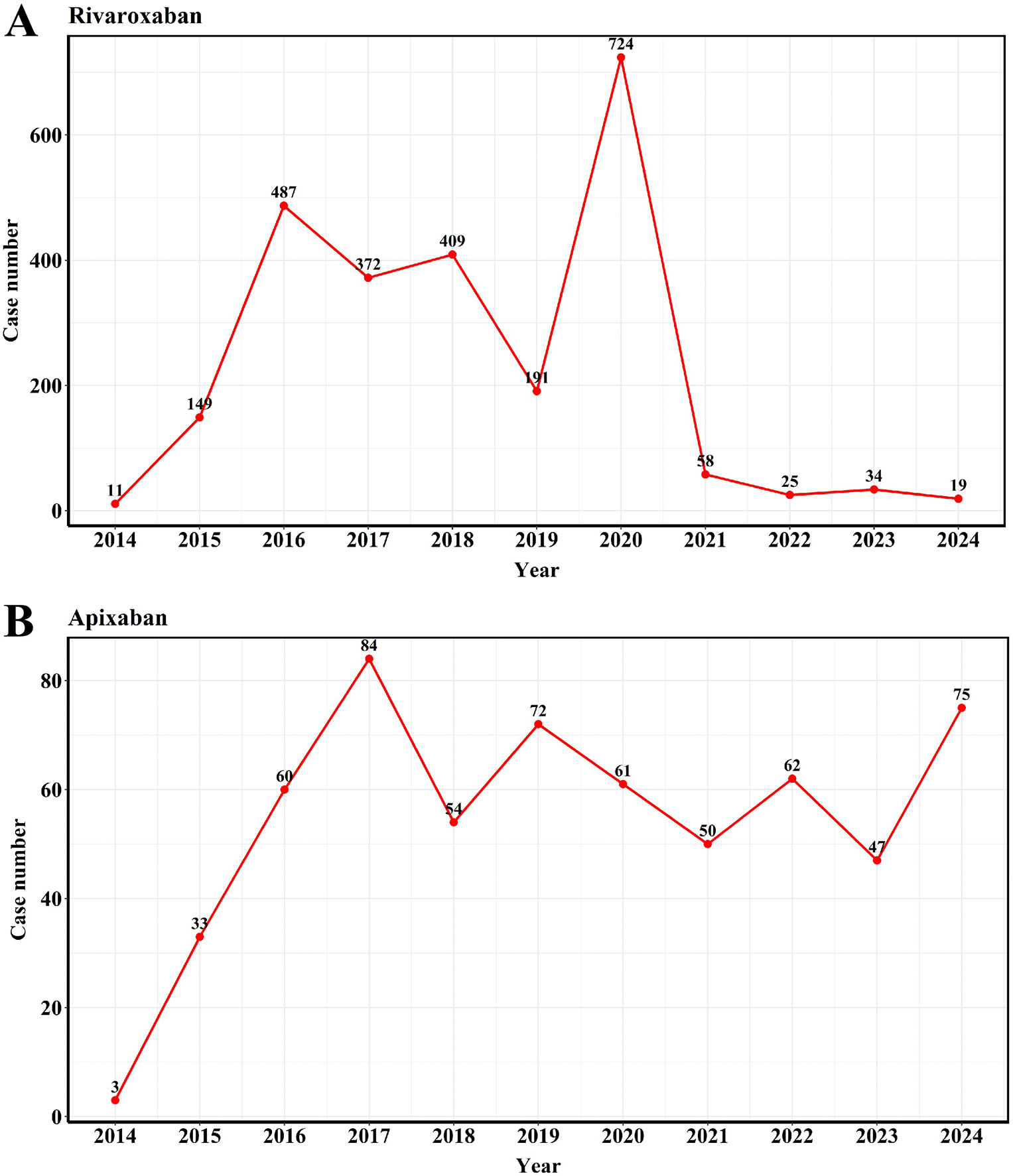
A total of 108,819 AE reports related to rivaroxaban and 135,127 reports related to apixaban were retrieved from the FAERS database between Q1 2014 and Q4 2024. Among them, 2,479 reports of AKI were associated with rivaroxaban (2.28%), while 601 AKI cases were associated with apixaban (0.44%). The annual number of AE reports related to direct factor Xa inhibitors over the past decade is shown in Figure 1.
Descriptive analyses of the clinical characteristics of the reported cases are summarized in Table 3. In both drug groups, AKI cases were predominantly reported in male patients and primarily occurred in individuals aged 65 years and older. Notably, AKI reports were rare among individuals younger than 18 years, likely reflecting the demographic profile of the treated population. The majority of AKI-related reports originated from the USA and France. The most frequently reported indications for direct factor Xa inhibitors included atrial fibrillation, cerebrovascular accident prophylaxis, thrombosis prophylaxis, pulmonary embolism, and hypertension.
Disproportionality analysis in elderly patients aged over 65 years
Since most AKI reports occurred in elderly patients (≥65 years), disproportionality analysis was limited to this subgroup, using the entire FAERS database as the reference. To validate the analytical performance of FAERS, ibuprofen and insulin glargine were used as positive and negative controls, respectively. As shown in Table 4, all 4 disproportionality methods indicated a strong association between ibuprofen and AKI (ROR = 5.75, 95% confidence interval (95% CI): 5.31–6.22; PRR = 5.63, χ2 = 2,377.41; EBGM = 5.58, EBGM05 = 5.22; IC = 2.47, IC025 = 2.34), whereas no significant association was observed for insulin glargine (ROR = 0.11, 95% CI: 0.08–0.16; PRR = 0.11; EBGM = 0.12, EBGM05 = 0.09; IC = –3.10, IC025 = –3.68). Subsequent disproportionality analysis using 4 methods (ROR, PRR, EBGM, and IC) revealed a significant signal for the association between rivaroxaban and AKI in patients aged ≥65 years, while no such signal was observed for apixaban (Table 4). Rivaroxaban exhibited a high ROR (3.82, 95% CI: 3.65–4.01), whereas apixaban had a lower ROR (0.86, 95% CI: 0.79–0.94). The PRR results were consistent with the ROR findings: the PRR for rivaroxaban was 3.78 (χ2 = 3543.98), whereas that for apixaban was 0.78 (χ2 = 10.73). Further validation using EBGM and IC also confirmed these findings: rivaroxaban showed EBGM = 3.68 (EBGM05 = 3.54) and IC = 1.88 (IC025 = 1.80), both exceeding the signal thresholds. In contrast, apixaban had EBGM = 0.86 (EBGM05 = 0.80) and IC = –0.21 (IC025 = –0.36), indicating no signal. Based on these results, subsequent analyses focused on rivaroxaban, which showed a significant association with AKI.
Comparative analysis with other antithrombotic agents
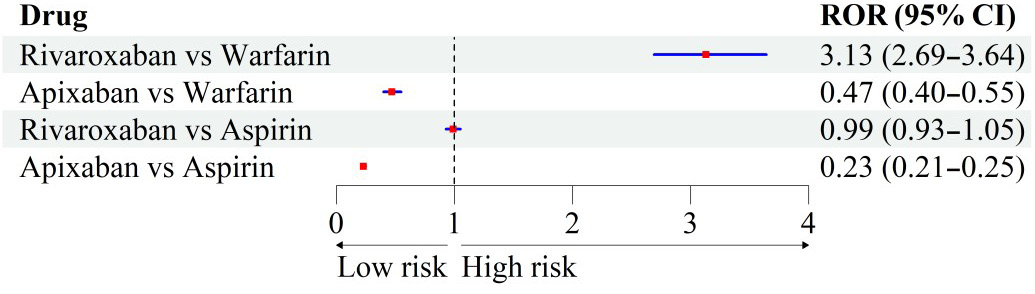
In addition to direct factor Xa inhibitors, commonly used oral antithrombotic agents include warfarin and aspirin. Figure 2 displays the variation in AKI signals for rivaroxaban and apixaban using warfarin or aspirin as reference drugs. Compared with warfarin, rivaroxaban showed a significant association with AKI (ROR = 3.13, 95% CI: 2.69–3.64), whereas apixaban did not (ROR = 0.47, 95% CI: 0.40–0.55). When compared with aspirin, neither rivaroxaban (ROR = 0.99, 95% CI: 0.93–1.05) nor apixaban (ROR = 0.23, 95% CI: 0.21–0.25) showed a significant signal.
Subgroup analysis in patients aged over 65 years
Given the observed association between rivaroxaban and AKI in older adults, a stratified analysis by sex and age was conducted to control for potential confounders (Table 5). Reporting odds ratio values for rivaroxaban remained above the signal threshold across all subgroups. Notably, the risk was more pronounced in elderly females, with an ROR of 6.05 (95% CI: 5.69–6.43), indicating higher susceptibility in this population. It should be noted that these findings warrant confirmation in larger, high-quality prospective studies.
Time to onset
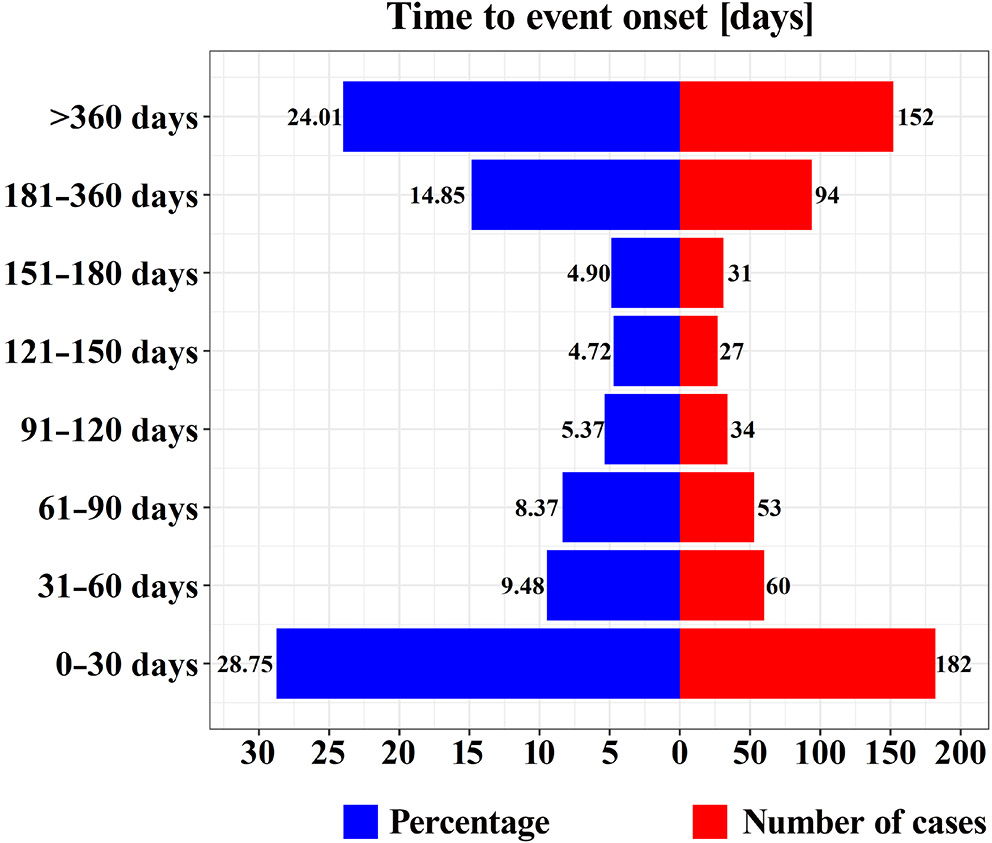
The median time to AKI onset following rivaroxaban administration was 109 days (interquartile range (IQR): 22–340 days). Approximately 50% of AKI events occurred within the first 3 months of treatment. Interestingly, about 10% of AKI cases emerged within the 1st week of drug exposure (Figure 3).
Prognosis of rivaroxaban-associated AKI in patients over 65 years
To assess the clinical outcomes of rivaroxaban-associated AKI, hospitalization and fatality rates were analyzed using the FAERS database (Table 6). The results indicated a hospitalization rate of 56.06%, a fatality rate of 37.67%, and a life-threatening event rate of 4.02%, all of which were significantly higher than those observed in patients without AKI. These findings highlight the substantial impact of AKI on clinical outcomes in this population.
Discussion
Currently, post-marketing safety data regarding direct factor Xa inhibitors and their use in renal disorders remain limited. The FAERS database, as one of the major global resources for detecting signals of rare AEs,22 provides invaluable data for pharmacovigilance and pharmacoepidemiological research and is freely accessible to researchers. In this study, we systematically investigated the potential renal adverse effects associated with direct factor Xa inhibitors using the FAERS surveillance system.
From spontaneous reports submitted between 2014 and 2024, we identified 2,479 AKI cases associated with rivaroxaban and 601 associated with apixaban. Although FAERS data cannot be used to estimate the true incidence rate, the proportion of AKI among all rivaroxaban-related AEs was 2.28% (2,479/108,819), suggesting that this AE may not be as rare as described in the product label. The main strength of this study lies in being the first to systematically evaluate the potential association between direct factor Xa inhibitors, particularly rivaroxaban, and AKI. All 4 disproportionality analysis methods indicated a significant signal for rivaroxaban-associated AKI: ROR = 3.82 (95% CI: 3.65–4.01), PRR = 3.78 (χ2 = 3,543.98), EBGM = 3.68 (EBGM05 = 3.54), and IC = 1.88 (IC025 = 1.81). In contrast, no statistically significant association was observed for apixaban.
With the growing number of patients with cardiovascular disease (CVD), the use of oral anticoagulants has become increasingly common. As early as 2017, case reports suggested that direct factor Xa inhibitors may induce nephrotoxicity, supported by renal biopsy findings in a patient treated with apixaban.23, 24 Subsequent reports by Galloway et al.25 and Iwafuchi et al.26 also described apixaban-associated AKI cases. However, our analysis indicated a significant signal only between rivaroxaban and AKI, with no similar findings for apixaban. Although both agents belong to the same class, emerging evidence suggests potential differences in renal safety profiles. Several comparative studies and meta-analyses have shown that apixaban may pose a lower risk of AKI than rivaroxaban in elderly individuals and those with CKD or diabetes.27 Apixaban has not been statistically linked to adverse renal outcomes in most patients with atrial fibrillation.27 This disparity may arise from differences in pharmacokinetics, renal clearance, and dosing regimens. For example, apixaban is less reliant on renal elimination than rivaroxaban, which may contribute to its more favorable renal safety profile. Additionally, proposed mechanisms of AKI induced by direct factor Xa inhibitors include glomerular hemorrhage, tubular obstruction by red blood cell casts, and free hemoglobin release.28 Users of apixaban had a lower risk of bleeding compared with those receiving rivaroxaban.29
We further analyzed the effects of sex and age on AKI risk. Rivaroxaban-associated AKI was more frequently reported in men and in patients aged ≥65 years. All 4 disproportionality methods confirmed a clear signal for rivaroxaban in the elderly subgroup. Epidemiological data indicate that individuals aged ≥65 years are at greater risk of cardiovascular events30 and experience higher rates of mortality31 and post-hospitalization disability,32 possibly due to declining organ function and metabolic capacity.33 Globally, the age-standardized mortality rate for CVD in men (280.8 per 100,000) is significantly higher than in women (204.0 per 100,000), particularly in high-income regions and across Central/Eastern Europe, Central Asia, and South Asia.34 Thus, male patients are more likely to be prescribed rivaroxaban, which may explain the higher number of AE reports in this group. Clinicians should exercise greater caution when prescribing rivaroxaban to male and elderly patients. With respect to geographical distribution, the majority of rivaroxaban- and apixaban-related AEs were reported in the USA and France, suggesting international differences in reporting behavior, potentially influenced by prescribing habits, regulatory practices, and awareness of the FAERS database. Time-to-onset analysis revealed that nearly 50% of AKI events occurred within 3 months of rivaroxaban initiation, with approx. 10% occurring within the 1st week. Although current clinical guidelines do not recommend routine renal monitoring for all rivaroxaban users,35, 36 our findings underscore the importance of early renal function surveillance to mitigate potential risks.
In terms of clinical outcomes, among the 1,789 rivaroxaban-associated AKI cases, 1,003 (56.06%) required hospitalization and 674 (37.67%) resulted in death, underscoring the severity of these events. In a study by Chen et al., 35% of 28 patients with direct oral anticoagulants (DOAC)-related AKI required acute dialysis, and 60% did not recover baseline renal function.37 Trujillo et al. similarly reported that 28% of patients receiving DOACs required long-term dialysis.38 These findings suggest that rivaroxaban-associated AKI may synergize with complications such as bleeding or infection, complicating treatment and increasing the healthcare burden.35 Nevertheless, this study cannot establish a causal relationship between rivaroxaban use and hospitalization or death, as these outcomes may also result from underlying disease progression or other clinical events. Prospective studies are warranted to verify these associations.
Importantly, although we observed disproportionality in the reporting of rivaroxaban-associated AKI, these findings do not imply causality and should not be overinterpreted. Numerous studies have demonstrated the therapeutic benefits of rivaroxaban in thrombotic disorders. For example, compared with aspirin, rivaroxaban combination therapy reduced all-cause and cardiovascular mortality in patients with chronic coronary or peripheral artery disease.36 Moreover, both rivaroxaban (hazard ratio (HR) = 0.66, 95% CI: 0.55–0.77) and apixaban (HR = 0.73, 95% CI: 0.59–0.87) have been shown to reduce the risk of renal impairment.39 In patients with moderate renal impairment and no increased bleeding risk, the benefit of rivaroxaban plus aspirin was preserved compared with aspirin alone.40 These findings are consistent with our results showing that neither rivaroxaban nor apixaban exhibited a significant association with AKI when aspirin was used as the comparator. Furthermore, rivaroxaban may provide greater benefits in patients with CKD or diabetes. In patients with atrial fibrillation, rivaroxaban has been associated with better renal outcomes than vitamin K antagonists (VKAs).12, 27 Among patients with nonvalvular atrial fibrillation and diabetes, rivaroxaban was associated with a lower risk of renal AEs than warfarin.41 In patients with both atrial fibrillation and advanced CKD, rivaroxaban use was associated with fewer renal AEs compared with VKAs.42 In elderly patients, rivaroxaban tended to improve primary safety outcomes regardless of renal function.43 However, our study identified a significant AKI signal for rivaroxaban, but not for apixaban, when compared with warfarin, which may differ from previous findings due to differences between real-world and case-control study designs.
Limitations of the study
This study has several strengths, including a large sample size, broad coverage of real-world data, and a systematic evaluation of the clinical characteristics and outcomes associated with rivaroxaban-related AKI. Nevertheless, it also has several limitations. First, FAERS data may be incomplete, and AKI diagnoses are often based on spontaneous reports without standardized criteria. Second, the lack of control for confounding factors (e.g., pre-existing CKD) limits causal inference. Third, missing baseline characteristics, exposure information, and renal function data hinder the estimation of incidence and attribution of causality.
Conclusions
Using real-world data from FAERS, this study identified a potential safety signal linking rivaroxaban to AKI in elderly patients (≥65 years). Given that most AKI cases occurred within 3 months of treatment initiation and were associated with high hospitalization and mortality rates, clinicians should remain vigilant and conduct regular renal monitoring, especially during the early phase of therapy. Our findings provide supplementary evidence for the rational use of rivaroxaban and highlight the need to monitor renal function in older adults. It is essential to emphasize that the observed disproportionality does not confirm a causal relationship and should not lead to overinterpretation of the results.
Data Availability Statement
The datasets supporting the findings of the current study are openly available in Zenodo at https://doi.org/10.5281/zenodo.15209285.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.