Abstract
Background. The stability of the tear film is essential for ocular health. Smoking, refractive errors (RE), and a high body mass index (BMI) are key risk factors for dry eye disease. Dry eye symptoms may be caused by a high tear evaporation rate (TER) and/or a thin lipid layer.
Objectives. To assess the correlation between TER and lipid layer patterns (LLP) within 4 distinct groups: healthy controls, smokers, subjects with RE, and individuals with high BMI.
Materials and methods. The study included 120 subjects aged 18–30 years divided into 4 groups (30 per group; 15 women and 15 men). The ocular surface disease index (OSDI) was assessed, followed by evaluation of LLP using EASYTEAR View+ and TER using the Delfin VapoMeter.
Results. Kruskal–Wallis tests revealed significant between-group differences in OSDI (χ2 = 62.91, n = 120, p < 0.001) and LLP (χ2 = 26.59, n = 120, p < 0.001), but not in TER (χ2 = 7.20, n = 120, p = 0.066). Within-group Kendall tau-b correlations between TER and LLP revealed strong negative associations in the high-BMI (τb = −0.563, n = 30, p < 0.001) and smoker groups (τb = −0.457, n = 30, p = 0.002). A moderate negative correlation was found in the RE group (τb = −0.287, n = 30, p = 0.043), but not in healthy controls (τb = −0.199, n = 30, p = 0.189).
Conclusions. The association between TER and LLP was strongly negative in smokers and the high-BMI group, moderate in the RE group, and absent in healthy controls. The inverse relationship between TER and LLP may indicate compromised tear film stability in populations at risk of dry eye disease.
Key words: smokers, tear film, high body mass index, dry eye syndromes, observational correlation study
Background
The tear film is crucial for vision and ocular health. Disturbances in tear film stability and osmolarity can lead to several disorders, with dry eye disease being one of the most common, affecting 5–50% of the population.1, 2 Symptoms include foreign body sensation, dryness, irritation, discomfort, and pain.3 Dry eye disease has significant economic and social impacts, making it important to identify associated factors such as digital screen use, contact lens wear, smoking, systemic illnesses, and certain medications.4
Dysfunction of the meibomian glands leads to increased tear evaporation, whereas lacrimal gland dysfunction results in aqueous deficiency.5, 6 Various tests are used to assess dry eye disease, as each measures different parameters.7, 8, 9, 10 The lipid layer spreads across the tear film with each blink to reduce tear evaporation and is therefore crucial for maintaining tear film stability and function.11 A portable evaporimeter has been effectively used to measure tear evaporation rate (TER).12, 13 This technique is quick, convenient, repeatable, and noninvasive compared with other methods. A TER value exceeding 25 g/m2/h at room temperature and approx. 30% humidity indicates the presence of dry eye symptoms.14
The EASYTEAR view+ is a noninvasive diagnostic tool designed for evaluating the tear film. It plays an essential role in identifying various dry eye syndromes. This device operates as an interferometer, offering detailed insights into the lipid layer of the tear film. It allows practitioners to measure noninvasive tear break-up time after inserting a specialized grid, providing valuable information about tear stability.15 However, it shares similarities with the Tearscope. The EASYTEAR view+ offers enhanced features, including an integrated stopwatch for precise timing and a light-emitting diode that serves as an effective light source for optimal visualization. This device can operate either as a portable handheld unit or be connected directly to a slit lamp, making it suitable for different clinical environments and practitioner preferences.15
Several studies have explored the evaluation of lipid layer patterns (LLP) in smokers, individuals with refractive errors (RE), and those with a high body mass index (BMI), among others.8, 16, 17, 18, 19, 20 For example, smokers and individuals with RE or a high BMI tend to exhibit lower LLP values than healthy individuals.8 However, these investigations often share a common limitation in participant selection: many include only young men or young women, thereby limiting broader population representation. The relationship between TER and LLP has not been systematically studied in smokers, individuals with RE, or those with a high BMI. This research gap highlights the need for further studies to better understand these correlations and their impact on dry eye syndrome.
The integrity of the tear film plays a crucial role in maintaining overall ocular health. Various factors can disrupt this delicate balance, leading to discomfort and dryness. Notably, smoking has been identified as a significant risk factor, as it can adversely affect tear production and quality. Additionally, individuals with RE may experience increased dryness due to imbalance within the visual system. Furthermore, a high BMI has also been linked to dry eye syndrome, as obesity may contribute to inflammation and hormonal changes that affect tear production. Together, these factors highlight the importance of lifestyle modification and appropriate eye care in maintaining a healthy tear film and preventing dry eye symptoms. Therefore, the present comparative observational study examined the correlation between LLP, assessed using EASYTEAR view+, and TER, evaluated using the Delfin VapoMeter, in 3 distinct groups: smokers, individuals with RE, and those with a high BMI.
Objectives
The study aimed to assess the correlation between TER and LLP in smokers, individuals with RE, and those with a high BMI. We hypothesized that smokers and individuals with RE and a high BMI would exhibit thinner lipid layers and higher TER values.
Materials and methods
Subjects
The current comparative observational study included a total of 120 participants aged between 18 and 30 years. They were categorized into 4 distinct groups: individuals with no ocular diseases or disorders, smokers with a smoking history of 1–11 years, individuals with RE ranging from +7.5 to −7.5 D, and those with a high BMI between 30.0 and 48.7 kg/m2, with each group comprising 15 women and 15 men. The sample size was determined based on the prevalence of these participant groups among university students.
Before commencing the study, written informed consent was obtained from all participants, ensuring that they were fully informed about the nature of the study. The study received ethical approval from the King Saud University Ethics Committee (Riyadh, Saudi Arabia; approval No. E-24-9087), and all procedures were conducted in accordance with the principles of the Declaration of Helsinki, emphasizing participant safety and rights. The study was conducted at the clinics of the Department of Optometry, College of Applied Medical Sciences, King Saud University (Riyadh, Saudi Arabia).
Specific exclusion criteria were established to maintain the integrity of the study. Individuals at risk for ocular dryness, such as those who had undergone recent eye surgery or were taking certain medications, were excluded. Other risk factors included thyroid disorders, elevated cholesterol levels, diabetes, and deficiencies in vitamins A and D. Furthermore, the study did not include pregnant or breastfeeding women, individuals with eyelid or eyelash abnormalities, or contact lens wearers. Additionally, participants who had undergone thyroid surgery or radioactive iodine therapy within the previous 3 years were excluded. Lastly, individuals with hypertension, anemia, or other serious health conditions were also excluded to ensure a homogeneous study population. The examiner was masked to ensure that she was unaware of the group to which each participant belonged.
The ocular surface disease index
The Ocular Surface Disease Index (OSDI) was used as a valid and reliable tool to assess the severity of dry eye disease and its impact on vision-related function. It is evaluated on a scale from 0 to 100, with higher scores indicating greater severity of ocular dryness. This index effectively differentiates between healthy individuals and patients with dry eye disease, demonstrating both sensitivity and specificity. All participants completed the OSDI at the beginning of the study. A score below 13 was considered indicative of normal ocular health.21
EASYTEAR VIEW+
The lipids in the tear film were assessed using the EASYTEAR view+ device (EASYTEAR S.R.L., Trento, Italy). This practical and compact device visually represents interference within the lipid phase of the tear film, providing a clearer understanding of lipid layer thickness (LLT). The same examiner performed all measurements to ensure consistency and reliability. The tests were conducted at a temperature of 20°C and a humidity level below 40%.8
Evaluation of the LLP allows detailed assessment of LLT. The LLP was categorized into 5 distinct grades: A, B, C, D, and E, each representing different characteristics and thicknesses of the lipid layer. Grade A showed a subtle gray appearance resembling a very thin white-blue layer associated with a LLT of approx. 13–15 nm. Grade B presented a more compact lipid layer, appearing as a slightly thicker white-blue layer, with an LLT ranging from 30 to 50 nm. Grade C was characterized by dynamic gray waves with a white-blue layer displaying distinct color fluctuations. The thickness of this lipid layer ranged from 50 to 80 nm. Grade D, with an LLT of approx. 80 nm, revealed a dense white-blue layer with a uniform appearance. In contrast, grade E, with an LLT ranging from 90 to 140 nm, displayed a wide variety of colors.8
Delfin VapoMeter
The TER was measured using a VapoMeter (Delfin Technologies UK Ltd, Westhumble, UK). The testing procedure was performed 3 times, with 2 readings obtained during each test. The 1st reading was recorded with both eyes open and blinking normally, while the 2nd reading was taken with both eyes closed after a 2-min interval. The TER was calculated by subtracting the reading obtained with the eyes closed from that recorded with the eyes open, and the mean values from the 3 tests were subsequently calculated. Under normal ocular conditions, the TER was considered to be below 25 g/m2/h, whereas readings above 25 g/m2/h indicated evaporative dry eye. Additionally, the effect of 2-propanol (70%) pads on the VapoMeter was evaluated.12, 13
Statistical analyses
The data for this study were collected using Microsoft Excel 2016 (Microsoft Corp., Redmond, USA). Following data collection, a detailed statistical analysis and interpretation of the data were performed using IBM SPSS v. 22.0 (IBM Corp., Armonk, USA) and R v. 4.4.3 (R Foundation for Statistical Computing, Vienna, Austria; session information and package details are listed in Supplementary Table 1).
Normality of age and continuous variables (OSDI and TER) was assessed within each group using the Shapiro–Wilk test (Supplementary Table 2). Due to violations of normality in the healthy, high BMI, and smoker groups, nonparametric methods were employed throughout. Between-group comparisons were performed using the Kruskal–Wallis one-way analysis of variance (ANOVA) by ranks for OSDDI, TER, and LLP. When the omnibus test was significant (p < 0.05), post hoc pairwise comparisons were conducted using Dunn’s test with Bonferroni adjustment for multiple comparisons (6 pairwise comparisons per variable). Within-group associations between LLP and continuous variables (OSDI and TER) were assessed using Kendall’s tau-b rank correlation coefficient. No multiplicity adjustment was applied to the correlation analyses, as each represented a distinct hypothesis within independent populations. Descriptive statistics are presented as median and interquartile range (IQR) values for age, OSDI, TER, and LLP. Statistical significance was set at p < 0.05 for all analyses.
Results
Table 1 presents the median (IQR) values for age, OSDI, TER, and LLP scores in the 4 groups. The OSDI scores varied according to the participants’ health conditions. Individuals with healthy eyes had OSDI scores ranging from 1.0 to 13.0, indicating no symptoms of dry eye. In contrast, the study groups showed significantly higher scores and, therefore, a greater degree of discomfort. Subjects with RE had OSDI scores ranging from 2.1 to 50. Participants with a high BMI presented OSDI scores between 8.3 and 72.9. Additionally, smokers had scores ranging from 8.3 to 52.1.
The TER scores also varied across the different groups. In subjects with healthy eyes, TER scores ranged from 5 to 22 g/m2/h, indicating normal tear evaporation. In individuals with RE, these scores ranged from 4 to 32 g/m2/h. Participants with a high BMI reported TER scores ranging from 6 to 65 g/m2/h, while smokers exhibited the widest range, with scores from 5 to 75 g/m2/h. For LLP, healthy individuals reported grades ranging from 2 to 5. Meanwhile, smokers and individuals with RE and a high BMI reported similar scores ranging from 1 to 5. These findings demonstrate differences in ocular surface health among the groups, highlighting the impact of underlying health conditions on tear film quality parameters.
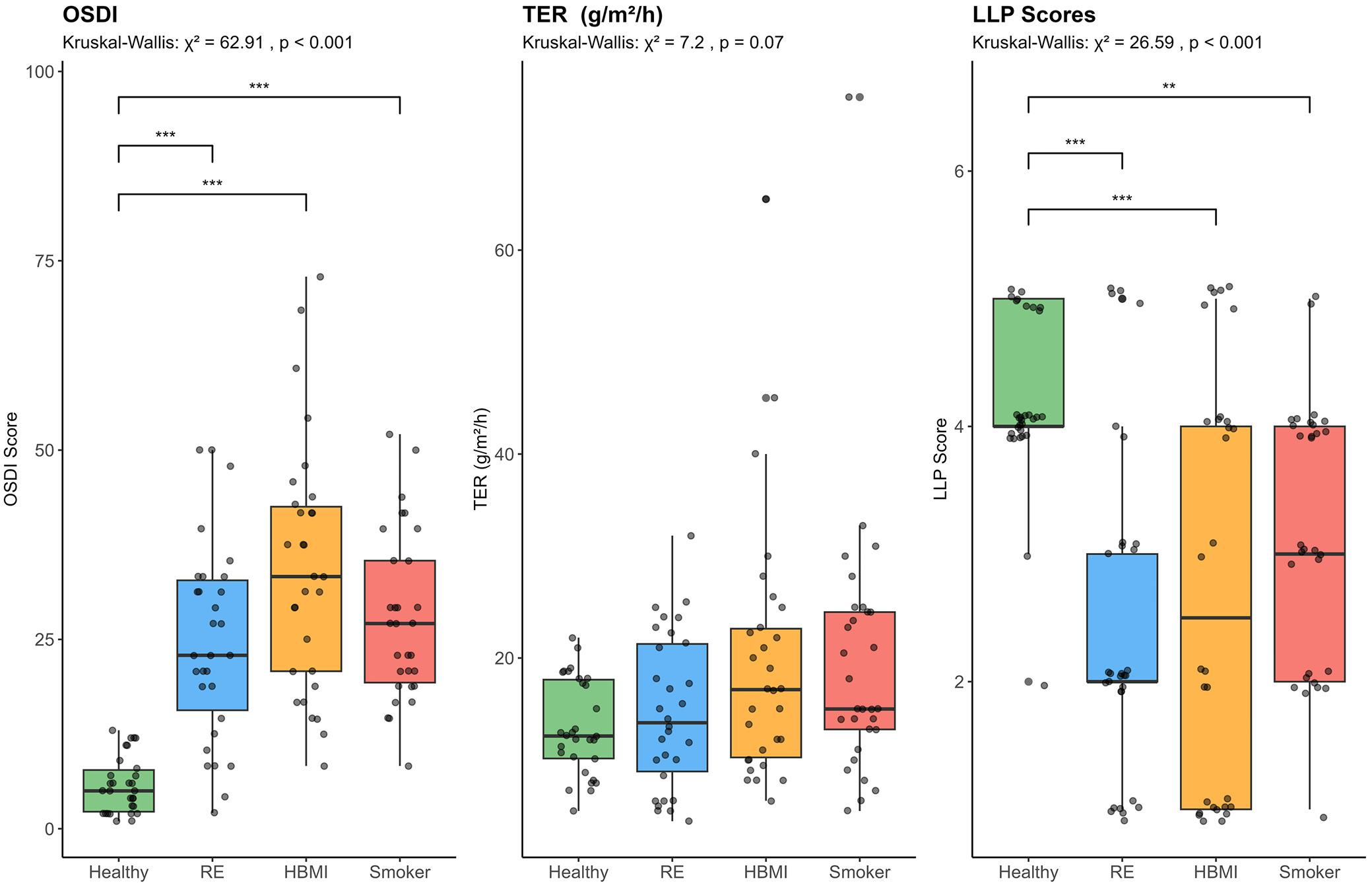
As shown in Table 2, the Kruskal–Wallis omnibus test for between-group differences was statistically significant for OSDI (χ2 = 62.91, n = 120, degrees of freedom (df) = 3, p < 0.001) and LLP (χ2 = 26.59, n = 120, df = 3, p < 0.001), but not for TER (χ2 = 7.20, n = 120, df = 3, p > 0.999). The corresponding effect size estimates for OSDI and LLP were both large (ε2 = 0.503 and 0.198, respectively). Results of Dunn’s post hoc pairwise comparisons with Bonferroni correction applied for 6 comparisons per variable are shown in Table 3 for OSDI and LLP. For both OSDI and LLP, significant differences (p < 0.01 or lower) were observed between the healthy group and each of the 3 study groups. However, there was no evidence of significant differences in these 2 measures among the RE, high BMI, and smoker groups. The analytical results are also illustrated in Figure 1, which includes side-by-side box-and-whisker plots with individual data points for OSDI, TER, and LLP scores by group.
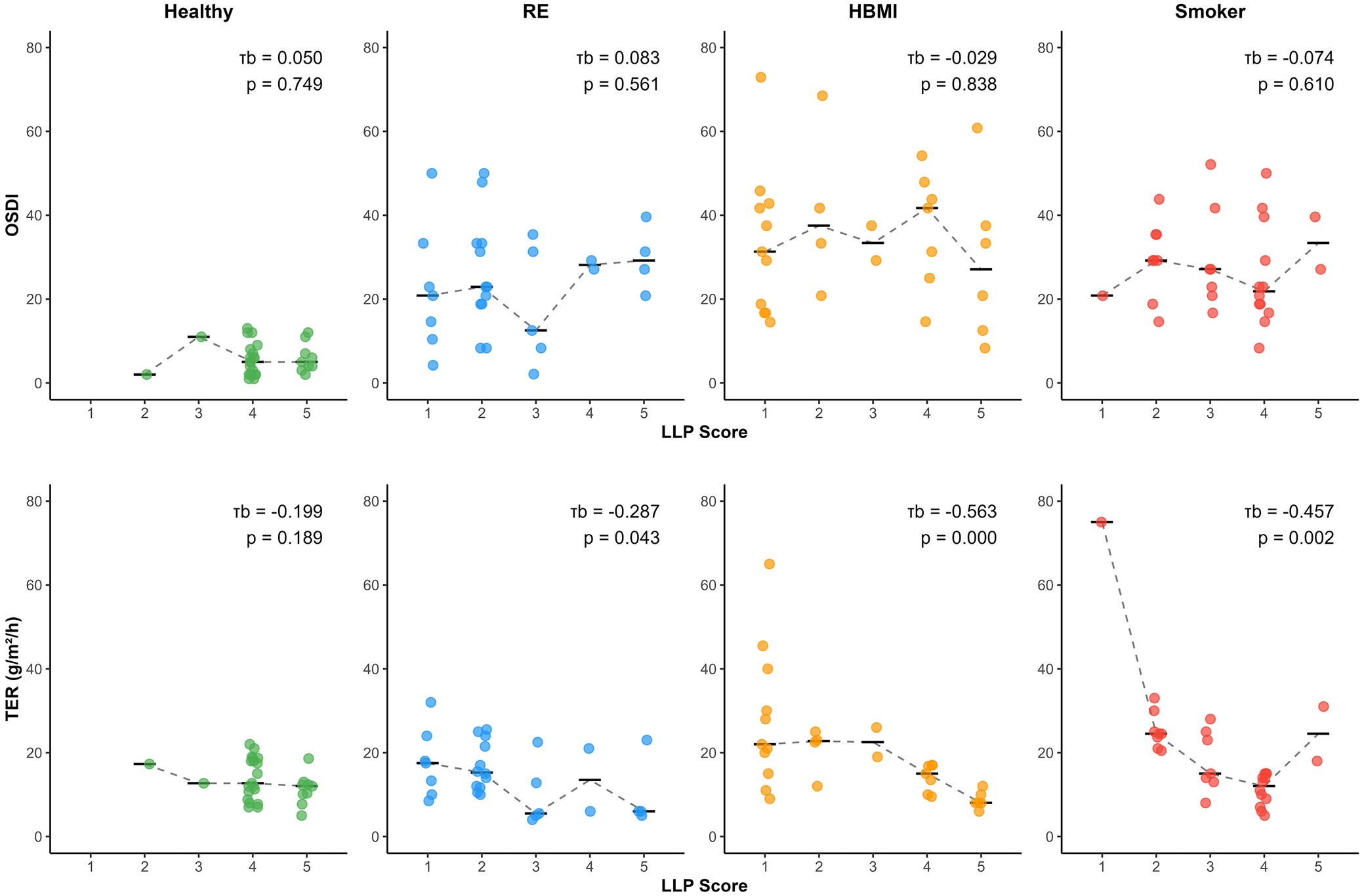
Results of the within-group correlation analyses are summarized in Figure 2. Kendall’s tau-b (τb) rank-order correlation coefficient was used to quantify the association between LLP scores and both OSDI and TER separately in each of the 4 study groups. No significant associations were detected for OSDI in any of the groups. By contrast, significant negative associations were detected in all groups except the healthy subgroup. For example, in individuals with a high BMI, a strong negative correlation was found between TER and LLP scores (τb = –0.563, n = 30, p < 0.001), indicating that as LLP increased, TER decreased. Similarly, among smokers, a strong negative correlation (τb = –0.457, p = 0.002) was also statistically significant, further underscoring the inverse relationship between these parameters. Subjects with RE exhibited a moderate negative correlation (τb = –0.287, n = 30, p = 0.043) between TER and LLP scores, suggesting a less pronounced but still meaningful inverse relationship. Although the association between TER and LLP scores was also negative among healthy subjects, it was not statistically significant (τb = –0.199, n = 30, p = 0.043).
Discussion
It was anticipated that the thickness of the lipid layer would influence TER. An increased LLT was expected to correspond with a reduction in TER.22 The findings of the current study indeed revealed a robust negative correlation between TER scores and LLP grades, particularly in individuals with RE, a high BMI, and smokers. Previous research has shown that both smokers and individuals with a high BMI tend to have significantly reduced LLT. Moreover, these groups also demonstrated lower tear meniscus height (TMH) scores compared with the control group.8
Elevated TER may increase tear osmolarity, indicating a higher concentration of solutes in the tear film. This phenomenon highlights the importance of understanding the complex relationship between TER and osmolarity, which requires further investigation. In evaporative dry eye, moisture loss through evaporation appears to result primarily from osmotic flow across the corneal and conjunctival surfaces rather than from secretion by the lacrimal glands.23, 24 This process acts as a compensatory mechanism to counteract evaporative moisture loss. As a result, this interaction helps mitigate the expected rise in osmolarity, highlighting the delicate balance within the ocular surface environment.23, 24 Tear evaporation rate plays an essential role in this process and may vary significantly depending on the LLP of the tear film. Importantly, eyes with thinner lipid layers exhibit substantially higher TERs, resulting in increased discomfort and dryness.
The integrity of the tear film lipid layer is essential for maintaining ocular health, and its disruption is particularly significant in smokers, in whom studies indicate an increase in TER of approx. 90–95%.25, 26 The lipid layer acts as a protective barrier, and its thickness is inversely correlated with TER, meaning that as the lipid layer thins, the TER increases. Interestingly, smokers, individuals with conditions such as RE, and those with a high BMI tend to exhibit a reduced thickness of this vital lipid layer. Thinning of the lipid layer disrupts its normal function, which may lead to changes in blinking rate.27 Blinking plays a vital role in maintaining the tear film by effectively spreading and evenly distributing lipids across its surface. When the blinking rate changes, instability of the tear film occurs, resulting in symptoms associated with dry eye.28 This instability is primarily driven by increased tear evaporation, causing irritation and discomfort in affected individuals. The interplay between these factors highlights the importance of preserving a healthy tear film for overall ocular health.
Dry eye disease in individuals with meibomian gland dysfunction (MGD) is alarmingly common, with prevalence rates ranging from 20% to 69%.29 Meibomian gland dysfunction disrupts the delicate balance of the lipid layer, leading to abnormalities in its components that can significantly increase the rate of water evaporation from the ocular surface. As such, LLT and integrity serve as critical indicators of meibomian gland function. Consequently, evaluation of LLP is an essential diagnostic tool for identifying obstructive MGD. A study involving patients diagnosed with MGD revealed that the thickness of the lipid layer does not consistently correlate with other important tear film parameters, including Schirmer, NIBUT, and TMH scores.30 This observation has led to the hypothesis that increased tear fluid production may compensate for the deficiency in the lipid layer resulting from MGD.31 However, the relationship between LLP and tear production remains controversial and warrants further investigation to better understand the underlying mechanisms.
Lipid layer thickness increased with age and exhibited a significant correlation with both meibomian gland secretion and morphology in middle-aged and older individuals with obstructive MGD. Measurement of LLT may serve as a valuable tool for diagnosing MGD. It is crucial to consider age as an important factor when evaluating the implications of LLT measurements.30 The LLT of patients with dry eye disease should not be considered in isolation; instead, it should be assessed alongside other tear film parameters.32
Limitations of the study
The study has several limitations worth mentioning. It involved a relatively small sample size, which may affect the generalizability of the findings. The research focused solely on a specific demographic, namely young individuals, primarily students from King Saud University. Additionally, all participants were recruited from a single geographic region, Riyadh, which may further limit the diversity and scope of the collected data.
Conclusions
Significant differences were found in OSDI and LLP scores between the control group and the 3 study groups (RE, high BMI, and smokers). For TER, a significant difference was observed between the control group and both the RE and smoker groups. Additionally, a significant difference in OSDI scores was identified between the RE and high BMI groups. A strong negative correlation was found between TER and LLP in smokers and individuals with a high BMI. In individuals with RE, a moderate negative correlation was observed between TER and LLP scores.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.17036238. The package contains the following files:
Supplementary Table 1. R session information.
Supplementary Table 2. Shapiro–Wilk test for normality by group.
Data Availability Statement
The datasets supporting the findings of the current study are openly available in Zenodo at https://doi.org/10.5281/zenodo.17036246.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.