Abstract
Background. Musculoskeletal disorders (MSDs) impose a significant burden on primary healthcare systems and the economy. Massage therapy (MT) may represent a useful tool for addressing these issues. However, the lack of robust evidence confirming its effectiveness makes this therapy controversial.
Objectives. This study aimed to assess the feasibility of implementing guideline-based MT into routine primary care practice.
Materials and methods. In this retrospective study, records of 258 primary care patients (median (Me) = 51.5 years; 1st and 3rd quartiles (Q1–Q3) = 42–66) were analyzed. These patients had previously received MT according to guidelines recommended by the Polish Society of Physiotherapy, the Polish Society of Family Medicine, the College of Family Physicians in Poland, and the European Rural and Isolated Practitioners Association (EURIPA). The effectiveness of therapy was evaluated using the visual analogue scale (VAS) and the number of general practitioner (GP) appointments booked by patients (NA).
Results. The majority of patients who received MT suffered from low back pain (M54.5) (39.1%); soft tissue disorders related to use, overuse, and pressure (M70) (27.5%); unspecified spondylosis (M47.9) (9.3%); and osteoarthritis of the knee (M17.5 and M17.9) (4.3%). A Wilcoxon test revealed a significant reduction in NA for M54.5 (p < 0.001), M70 (p < 0.001), others (p < 0.001), M17 (p = 0.004), and M47.9 (p < 0.001), as well as in VAS scores for M54.5 (p < 0.001), M70 (p < 0.001), others (p < 0.001), M47.9 (p < 0.001), and M17 (p = 0.003) after MT.
Conclusions. This study supports the potential benefits of integrating physiotherapy-led massage into routine primary care practice for the management of selected musculoskeletal disorders. When implemented in cooperation with family physicians, MT may reduce pain and decrease the need for additional GP visits.
Key words: primary health care, pain management, musculoskeletal diseases, clinical practice guidelines, massage therapy
Background
Musculoskeletal disorders (MSDs) are among the most prevalent and disabling health conditions worldwide, affecting approx. 1.71 billion people across all age groups.1 These disorders not only cause persistent pain and limit mobility but also significantly impair quality of life and social functioning. Beyond their direct impact, MSDs are associated with an increased risk of developing chronic comorbidities such as cardiovascular disease (CVD), obesity, and diabetes.2 The growing incidence of MSDs observed in recent decades reflects a combination of demographic changes, sedentary lifestyle, and occupational exposures.3, 4 This trend imposes an increasing burden on individuals, healthcare systems, and national economies.
Despite their prevalence, the management of MSDs remains suboptimal. Pharmacological interventions such as opioids and non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used, particularly in early-stage disease.5, 6 However, the effectiveness of opioids in reducing musculoskeletal pain is questionable and may paradoxically contribute to prolonged work disability.5 NSAIDs, although widely accepted, carry a well-documented risk of gastrointestinal, renal, and cardiovascular adverse effects.6 This is especially concerning in the current healthcare landscape, where there is growing recognition of the public health consequences of long-term opioid and NSAID use.7, 8 As a result, there is an urgent need to identify safe and accessible non-pharmacological alternatives that could be implemented in primary healthcare settings.
In addition to their clinical consequences, MSDs generate substantial economic and systemic burdens. From the perspective of primary care, patients with MSDs frequently consult general practitioners (GPs), require diagnostic imaging, and often receive long-term pharmacotherapy.9, 10 These repeated interactions with the healthcare system result in increased costs, resource utilization, and administrative workload. Furthermore, MSDs contribute to absenteeism, reduced work productivity, and early retirement, particularly among working-age populations.9 This underscores the need for cost-effective interventions that can reduce symptom burden while minimizing healthcare resource utilization.
Massage therapy (MT) is one such intervention. It is a well-established component of physiotherapeutic practice and has demonstrated promising results in relieving pain and improving function in patients with various MSDs, particularly in the early or subacute stages of disease progression.11, 12, 13 Moreover, MT may be used as a preventive measure or as part of self-management strategies under professional guidance.14, 15, 16 Despite its accessibility, safety, and low cost, MT remains underutilized in standard medical care.
There are 2 primary reasons for this underuse. First, the lack of consistent, high-quality empirical evidence supporting the clinical efficacy of MT limits its acceptance among medical professionals and hinders its integration into routine primary care protocols.17, 18, 19 Second, the mechanisms through which MT exerts its therapeutic effects are not yet fully understood. Although evidence suggests that MT may influence biomechanical, neurological, and psychological processes, these effects remain insufficiently explained within a unified theoretical framework. Bridging this gap would require integration of disciplines such as anatomy, physiology, histology, and pathophysiology into MT research and training programs.16, 20 Importantly, the implementation of MT in primary care does not require highly specialized equipment or infrastructure. It may be delivered in a standard consultation room by a trained physiotherapist, either independently or in collaboration with family physicians. Such integration aligns with contemporary models of interdisciplinary care and is supported by national and international professional associations. Additionally, MT may serve as a form of autotherapy, contributing to self-management within the framework of social prescribing.21 Nevertheless, real-world data regarding the practical implementation of MT in family medicine – particularly in terms of feasibility, effectiveness, and impact on healthcare utilization – remain limited.
This study addresses this gap by examining the use of guideline-based MT in patients with selected MSDs in a primary care setting. It focuses on the collaborative role of physiotherapists and GPs in delivering MT and its potential to reduce both pain and healthcare utilization.
Objectives
This study aimed to assess the feasibility of implementing guideline-based MT in routine primary care practice, in line with the recommendations of the Polish Society of Physiotherapy, the Polish Society of Family Medicine, the College of Family Physicians in Poland, and the European Rural and Isolated Practitioners Association (EURIPA).
Specifically, the study explored whether MT, when delivered by physiotherapists in cooperation with family physicians, may contribute to reductions in both pain intensity and the number of GP consultations among patients with selected MSDs. The findings are intended to inform the potential integration of MT as a practical, non-pharmacological intervention into standard care pathways in family medicine.
Material and methods
Study design
This was a retrospective analysis of de-identified case records of primary care patients with selected MSDs. The project was conducted in accordance with the Declaration of Helsinki and was approved by the Senate Research Ethics Committee of the University of Physical Education in Wroclaw, Poland (approval No. 2/2018). The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.22
Setting
Data were collected between May 2019 and August 2023 at one of the medical centers in Wrocław. Data from patients treated with MT were obtained from the Dr Eryk medical database.
Participants
Participants’ records were included in the dataset if they: 1) were aged 40 years or older; 2) were diagnosed with an MSD by a GP; 3) experienced pain greater than 3 on the visual analogue scale (VAS) before MT; 4) were prescribed MT interventions by a GP; and 5) had continuous medical records for at least 6 months before MT and no less than 6 months afterward at the time of data extraction from the database.
Patients’ records were excluded from the dataset if they: 1) had a history of traumatic injuries, congenital musculoskeletal defects, deep vein thrombosis, myocardial infarction, or cancer within the past 5 years; 2) had undergone a surgical procedure within the past 5 years; 3) had acute inflammation of the respiratory, digestive, or genitourinary systems; 4) had incomplete medical records; or 5) were pregnant.
Variables
Pain assessment (primary endpoint)
Pain intensity was measured using the VAS. This is a continuous scale consisting of a 100-mm horizontal line anchored by “no pain” (score of 0) and “worst imaginable pain” (score of 10). The VAS is frequently used as an outcome measure to assess treatment effectiveness. Most studies have shown that the VAS is a valid and reliable scale.23, 24 Measurements were taken immediately before the intervention and after completion of the massage session.
Number of appointments (exploratory endpoint)
As an indicator of massage utility in primary healthcare, the number of appointments (NA) patients had with doctors during a 1-year period, including 6 months before and 6 months after MT, was analyzed. Consultations took place in doctors’ offices. In every case, the analyzed change in NA referred to the same disorder. Patients who developed other diseases within 6 months after MT were excluded from the study. The reported reduction in NA was therefore directly associated with the original health condition under investigation and was not influenced by other health issues.25
Data sources
Part of the data (sex, age, type of disease, and NA) was extracted from the Dr Eryk database, which contains patient records entered by GPs from general practices across Poland. The patient population within the database may be considered representative of the Polish population in terms of demographics and disease distribution. The database contains patients’ complete medical histories. In particular, information on the dates of registration with and withdrawal from the practice is collected. Information regarding referrals to secondary care, including specialty type, is also recorded. The database includes details on hospital admissions, discharge medications, diagnoses, outpatient consultations, investigations, and treatment outcomes. The database software is provided free of charge by the Polish National Health System. The authors did not have direct access to the database. Data on the number of massage sessions and pain intensity were extracted from the physiotherapy practice collaborating with the medical center operating the Dr Eryk database.
Bias
The NA indicator should not be considered a direct measure of massage efficacy. Rather, this indicator may suggest that MT is one of the factors positively influencing patients’ health conditions. However, other factors that may affect patients’ health status should also be taken into consideration. These include demographic factors (age, sex, education), psychosocial factors (beliefs, motivation), healthcare system factors (limited accessibility, long waiting times), socioeconomic factors (inability to take time off work, cost, and income), disease-related factors (symptoms and disease severity), as well as tobacco smoking and alcohol consumption.26
Exposure
The MT intervention applied in this study followed a structured protocol developed and endorsed by the Polish Society of Physiotherapy, the Polish Society of Family Medicine, the College of Family Physicians in Poland, and EURIPA. The detailed protocol, consistently implemented by the physiotherapist, is publicly available.16 To ensure adherence to the guidelines, a printed checklist was used during each session, listing the anatomical structures to be palpated and massaged. The therapist marked each completed step, thereby confirming adherence to the standardized procedure.
Unlike unstructured or practitioner-dependent massage practices, the protocol employed in this study was specifically designed for primary care settings. It required the therapist to target defined musculoskeletal structures – such as muscles, tendons, and ligaments – in a predetermined sequence. The approach aimed to restore functional balance in adjacent and interrelated anatomical areas. The protocol also included patient education and instruction in self-massage techniques to promote continuity of care and self-management between sessions. In contrast, unstructured MT often varies in technique, target areas, and therapeutic rationale depending on individual practitioner preferences or patient requests, which may limit reproducibility and consistency.
All treatments were delivered with the patient in a side-lying position, resting on the unaffected side. Supportive bolsters were placed under the head and upper and lower limbs to ensure comfort and proper alignment. The techniques used – effleurage, petrissage, friction, and compression – were based on Swedish massage methodology. According to Walton’s massage therapy pressure scale, level 4 pressure (strong) was consistently applied.27 Each session lasted 45 min. Massage was administered exclusively by a physiotherapist with more than 20 years of clinical experience and only when prescribed by a GP. Treatment continued until the patient reported a pain intensity of 3 or lower on the VAS, or until both the therapist and patient agreed to conclude therapy based on achievement of therapeutic goals and observed clinical progress.
Sample size
The sample size required to detect differences between 2 dependent means was calculated using G*Power software v. 3.1.9.7 (Heinrich Heine University (HHU), Düsseldorf, Germany). An effect size of Cohen’s d = 0.25, a 2-sided α = 0.01, and a statistical power of 90% were assumed. The required sample size was 242 participants. The number of extracted records was slightly higher than the predetermined sample size (n = 258).28
Statistical analyses
All statistical analyses were performed using IBM SPSS v. 29 (IBM Corp., Armonk, USA). Categorical variables are presented as frequencies and percentages (n, %). Continuous variables were assessed for normality of distribution using the Kolmogorov–Smirnov test (n > 50) or the Shapiro–Wilk test (n > 10) and are presented as mean ± standard deviation (SD) or median with interquartile range (Me; Q1–Q3), depending on the normality of distribution. Differences between measurements were analyzed using the χ2 test or Fisher–Freeman–Halton exact test (FFH) when variables were categorical. Changes between 2 related samples were analyzed using the Wilcoxon signed-rank test when differences between measurements were not normally distributed, whereas a paired t-test was used when differences were normally distributed. For unrelated samples, the Mann–Whitney U test was used to compare 2 groups when variables were continuous and not normally distributed, while the Kruskal–Wallis H test was applied when more than 2 groups were compared. Effect sizes were calculated using r for the Mann–Whitney U test and Wilcoxon test (r = Z/√n), φ for the χ2 test (φ = √(χ2/n)), and Cramér’s V for the FFH test. The significance level used for analysis was p < 0.05.
Results
Baseline characteristics of the participants are presented in Table 1. Briefly, 258 patients were reviewed (median age: 52 years; Q1–Q3 = 42–66 years); 159 (61.6%) were female and 99 (38.4%) were male. Based on the χ2 goodness-of-fit test, the sex distribution in the sample did not match that of the population (χ2(1) = 13.95, p < 0.001, φ = 0.23). A Mann–Whitney U test did not reveal a significant difference in age between women (Me = 54 years, n = 99) and men (Me = 49 years, n = 159) (U = 6644.5, p = 0.083, r = 0.108). On average, women were 5 years older than men. To analyze age as a potential variable, patients were divided into 3 age groups: 35 years and younger (15.5%), 36–55 years (39.5%), and 56 years and older (43.8%). A χ2 goodness-of-fit test revealed a statistically significant difference between groups (χ2(2) = 36.447, p < 0.001, φ = 0.38). Participants’ body height was Me = 168 cm (Q1–Q3: 162–175 cm), body weight was Me = 76.5 kg (Q1–Q3: 65–87 kg), and body mass index (BMI) was Me = 24.77 kg/m2 (Q1–Q3: 22.14–26.94 kg/m2).
Most patients in the study exhibited chronic symptoms. The majority of patients who received MT suffered from M54.5 (low back pain; 39.1%), M70 (soft tissue disorders related to use, overuse, and pressure; 27.5%), M47.9 (spondylosis, unspecified; 9.3%), and osteoarthritis of the knee (M17.5 and M17.9; 4.3%) according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10). The remaining cases were grouped into a category labeled “others” (19.8%). This group included the following ICD-10 codes: G54 (0.4%), M05 (0.4%), M06 (1.6%), M10 (0.8%), M15 (1.2%), M16 (1.9%), M18 (0.4%), M19 (1.2%), M41 (0.4%), M43 (0.8%), M48 (0.4%), M50 (2.3%), M53 (3.5%), M72 (0.4%), M75 (2.7%), M77 (0.8%), M79 (0.4%), and M81 (0.4%).
The results of the FFH test (p = 0.21, Cramér’s V = 0.15) did not indicate a significant association between sex and disease type. Additionally, the FFH test (p = 0.025, Cramér’s V = 0.189) demonstrated a significant association between disease type and age group.
The number of massage sessions
A total of 334 massage sessions were conducted in the analyzed group. The majority of patients (77.9%) experienced a significant reduction in pain after a single massage session (VAS < 3). Pain relief was achieved after 2 sessions in 17.1% of patients, while only 5.1% required 3 or more sessions for pain alleviation. Although the VAS threshold guided the intervention endpoint, therapy was limited to a maximum of 4 sessions to prevent indefinite continuation and ensure consistency across patients. A Mann–Whitney U test revealed the difference in the number of MT sessions between women (Me = 1, n = 99) and men (Me = 1, n = 159) in the group (U = 6824.5, p = 0.013, r = 0.154).
In terms of age, a Kruskal–Wallis H test revealed statistically significant differences between older patients who were 56 years old and older (Me = 1, n = 113), patients aged 36−55 years (Me = 1; n = 102) and patients aged 35 years and younger (Me = 1, n = 43) H (2) = 6.957, p = 0.031.
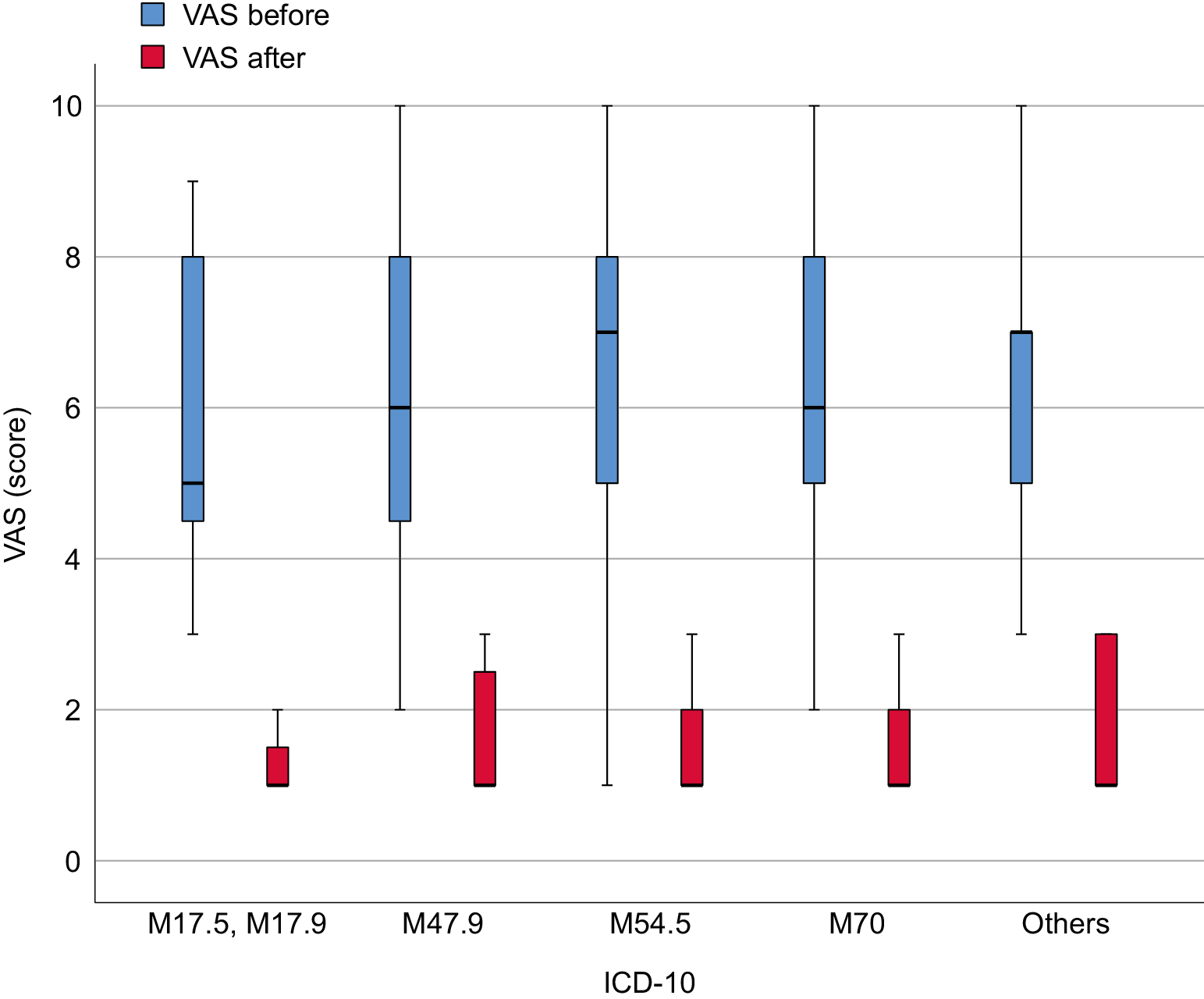
Visual analogue scale
The results of the VAS scores are presented in Table 2. Wilcoxon tests were used to compare VAS scores before and after MT. The results of the comparisons were reassessed using the Bonferroni correction. The analysis confirmed significant effects for all tested conditions: M54.5 (z = −8.664, p < 0.001, r = 0.862), M70 (z = −7.295, p < 0.001, r = 0.866), others (z = −6.124, p < 0.001, r = 0.857), M47.9 (z = −4.305, p < 0.001, r = 0.879), and M17 (z = −2.946, p = 0.003, r = 0.888) (Figure 1).
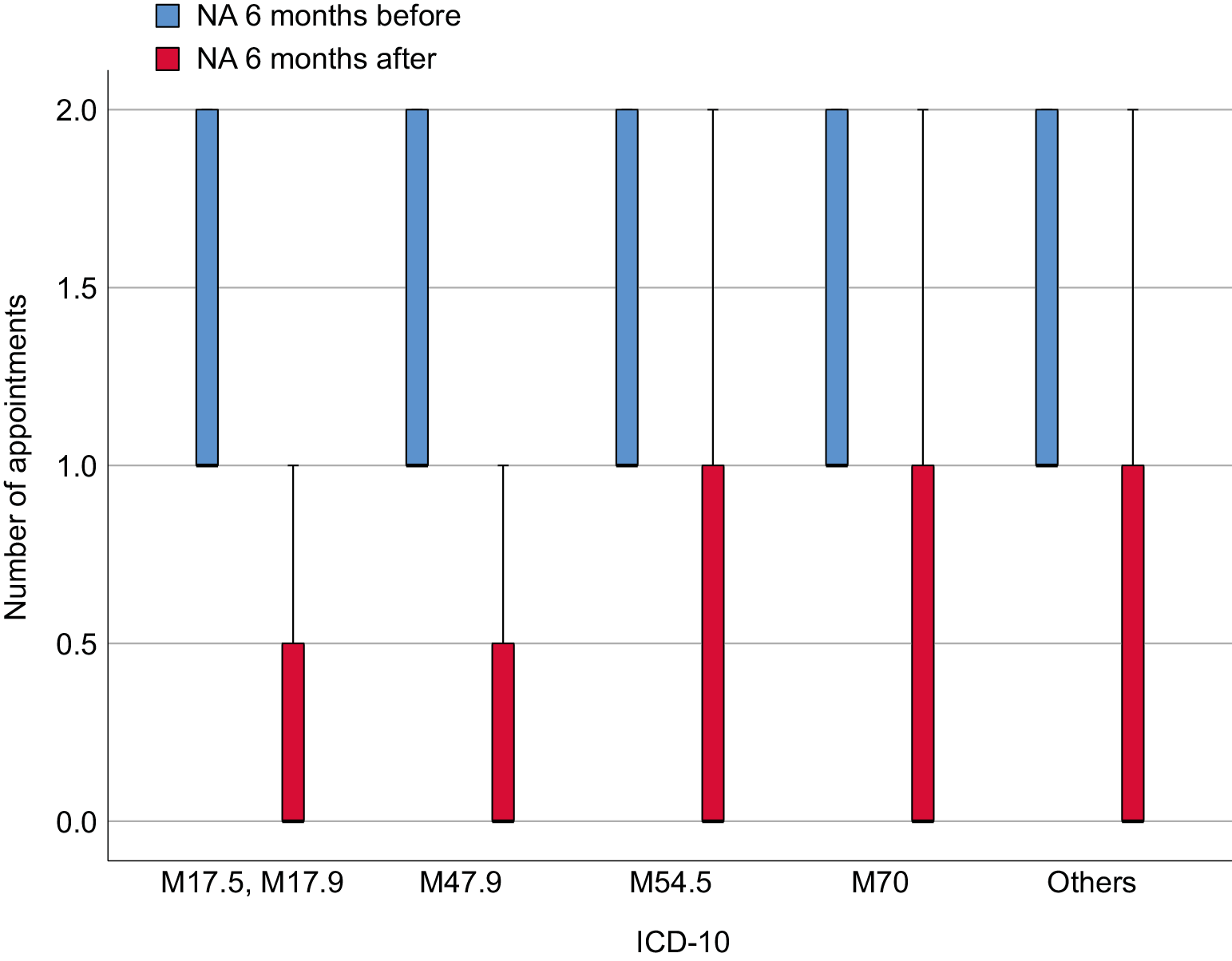
The number of appointments
A total of 285 appointments were recorded within 6 months before MT. Every patient attended at least 1 appointment with a GP, with a maximum of 4 appointments. Following MT, a reduction in NA was observed (Table 2). Patients booked 127 appointments.
Patients were divided into 5 subgroups, and the results were compared using Wilcoxon tests. After applying the Bonferroni correction for multiple comparisons, the significance of the results was reassessed. M54.5 (z = −7.978, p < 0.001, r = 0.794), M70 (z = −7.152, p < 0.001, r = 0.849), others (z = −5.124, p < 0.001, r = 0.717), M17 (z = −2.919, p = 0.004, r = 0.880), and M47.9 (z = −4.245, p < 0.001, r = 0.866) remained highly significant (Figure 2).
Discussion
This study assessed the implementation of guideline-based MT in a primary care setting among patients with selected MSDs, with particular focus on its association with reductions in pain intensity and the number of GP appointments. The use of a structured protocol developed and endorsed by national and European professional societies, and applied in cooperation between physiotherapists and family physicians, makes this study a relevant contribution to the ongoing discussion regarding the integration of non-pharmacological therapies into routine primary care.
The key findings of this study – namely, the reduction in both pain intensity and GP visits – suggest a potential role for structured MT as a supportive intervention in the management of MSDs. These outcomes are particularly noteworthy given the limited number of comparable studies examining both clinical and organizational indicators. The observed effect should not be attributed solely to the physical intervention itself, but rather to the consistency and rigor of the applied protocol. This aligns with evidence from other therapeutic disciplines, where standardization and integration into broader care pathways tend to enhance treatment effectiveness.
Importantly, the findings must be interpreted in the context of mixed evidence regarding the efficacy of MT. Although some previous studies suggest that MT may lack long-term benefit or produce only modest effects,29, 30 these results often stem from trials using heterogeneous methods, unstructured treatment plans, or insufficient control of confounding factors. In contrast, the present study applied a uniform, anatomically informed protocol monitored through checklists and delivered in collaboration with GPs – conditions that more closely resemble the intended setting of real-world implementation.
Still, MT should not be seen as a universal or standalone solution. While a substantial proportion of patients benefited from therapy, some reported persistent pain requiring additional or alternative forms of management. In such cases, MT may serve best as an adjunct to pharmacotherapy, structured exercise, or psychological interventions. Conversely, in patients who cannot tolerate pharmacological options or who present with contraindications to standard treatments, MT may represent a valuable therapeutic alternative. This interpretation corresponds with World Health Organization (WHO) guidelines, which recommend massage only as part of a broader management plan for chronic low back pain,31 and is also consistent with evidence of short- to medium-term efficacy reported by Furlan et al.32
The evidence supporting the effectiveness of MT in different MSD subtypes remains heterogeneous. For example, in knee osteoarthritis, Wu et al. and Perlman et al. provided differing assessments of MT, ranging from limited short-term benefit33 to functional improvement and pain reduction.34 Perlman et al. noted a clinically significant benefit using a whole-body massage protocol resembling the structured intervention applied in the present study.34 Similarly, Jurecka et al. demonstrated that soft tissue therapy, including MT, may be useful both as a primary and adjunctive approach.35 On the other hand, Yuan et al. concluded that the current evidence base remains inconclusive and that more rigorous research is needed.36
In spondylosis-related pain, findings are also variable. Cheng and Huang found moderate-quality evidence supporting the efficacy of MT in cervical spondylosis,37 while Al-Mutairi et al. and Gross et al. raised concerns regarding the insufficient quality of available studies.38, 39 For thoracic spondylosis, data remain scarce, although Srokowska et al. demonstrated promising effects of deep tissue massage in the management of thoracic spine pain.40 However, methodological differences between their protocol and the one used in the present study limit the comparability of the results.
The impact of MT on soft tissue disorders related to overuse, pressure, or poor posture has been relatively underexplored. While much of the literature focuses on athletes, primary care populations with work-related or degenerative soft tissue conditions remain understudied. Our findings suggest that MT may provide relief in these cases, particularly when pain is localized and not attributable to systemic inflammatory processes. Further research is warranted to validate its role in this subpopulation.14
From a broader perspective, the discussion regarding the utility of MT in primary care should also consider its feasibility and acceptability in routine practice. The protocol used in this study required minimal equipment and could be implemented in a standard medical consultation room. It was conducted by a physiotherapist with more than 20 years of experience and always upon GP referral. Although this enhances the internal validity of the findings, it may also limit generalizability, as not all practices have access to such highly trained personnel. Moreover, frequent application, as required in some chronic pain conditions, could place strain on healthcare resources and increase waiting times. As noted in previous studies, this logistical barrier may partially explain the limited effectiveness of MT in real-world settings.29, 30
Finally, although this study focused primarily on clinical and healthcare utilization outcomes, it is important to acknowledge the broader psychosocial benefits of MT, including reductions in anxiety, increased satisfaction with care, and perceived support from healthcare providers.41 These factors, although not formally assessed in the present analysis, may mediate or enhance the therapeutic effects of MT and merit inclusion in future studies.
This study provides preliminary yet promising evidence that structured, guideline-informed MT may be a feasible and potentially effective intervention for selected MSDs in primary care. When embedded in collaborative models involving GPs and physiotherapists, and when targeted at appropriate clinical indications, MT may offer both symptom relief and reductions in healthcare utilization. Further controlled studies with long-term follow-up and broader implementation contexts are needed to confirm these findings and inform policy and clinical guidelines.
Interpretation
The results suggest that MT, when provided by physiotherapists in collaboration with family physicians, may help reduce both pain intensity and the number of GP consultations in patients with selected musculoskeletal disorders. This highlights the potential value of including physiotherapeutic interventions directly in primary care settings. Although the retrospective nature of the study limits causal interpretation, the observed outcomes support further exploration of structured cooperation models between physiotherapists and primary care providers.
Generalizability
The study involved adult patients with chronic musculoskeletal complaints treated in a primary care setting. Massage therapy was delivered by a qualified physiotherapist operating in close coordination with a family physician, which reflects a feasible model of interdisciplinary care. However, the generalizability of the findings may be limited in contexts where such collaboration is not structurally supported or where physiotherapists are not integrated into primary care teams. The conclusions also pertain to a specific type of massage and cannot be extrapolated to all forms of manual therapy.
Limitations of the study
This study has several important limitations that should be considered when interpreting the findings. First, its retrospective design precludes causal inferences. As data were collected after the intervention had already taken place, the study is subject to potential selection and information biases, which may have influenced the observed associations. Second, the presence of uncontrolled confounding variables limits interpretation of the results. Patients may have used analgesics, participated in physical therapy, performed self-directed exercises, or received psychological support during the observation period. These co-interventions were not documented and could have contributed to the observed improvements independently of MT. Third, the number of GP NAs, used as an exploratory indicator of potential benefit, may be influenced by various non-clinical factors such as healthcare access, patient preferences, or organizational policies. Therefore, this metric should not be regarded as a direct measure of clinical effectiveness. Moreover, the study did not distinguish between acute and chronic presentations of musculoskeletal disorders, nor did it account for possible delayed effects of treatments initiated prior to the massage intervention. Finally, the generalizability of the findings is limited by the use of a single therapist following a specific protocol, and comparisons with other studies are constrained by methodological heterogeneity, including variations in massage techniques, diagnostic classifications, and outcome measures.
Conclusions
This study supports the potential integration of physiotherapy-led massage into routine primary care practice for the management of selected musculoskeletal disorders. When implemented in cooperation with family physicians, MT may reduce pain and decrease the need for additional GP visits. This underscores the importance of closer collaboration between physiotherapists and primary care providers in developing efficient, evidence-informed care pathways for patients with musculoskeletal complaints.
Data Availability Statement
The datasets supporting the findings of the current study are openly available in Figshare at https://doi.org/10.6084/m9.figshare.28716092.
Consent for publication
Not applicable.
Use of AI and AI-assisted technology
Not applicable.