Abstract
Background. Circulating tumor DNA (ctDNA) is a promising noninvasive biomarker in advanced breast cancer. In patients with advanced HER2-positive disease, responses to targeted therapy vary. The prognostic significance of ctDNA mutations across different genes and treatment regimens remains to be fully clarified.
Objectives. This meta-analysis evaluated the predictive role of ctDNA mutations in guiding anti-HER2 therapy.
Materials and methods. We searched PubMed, Embase, the Cochrane Library, and major oncology conference proceedings for studies evaluating associations between ctDNA and progression-free survival (PFS) or overall survival (OS) in breast cancer. Pooled hazard ratios (HRs) and odds ratios (ORs) were calculated using a pre-specified random-effects model. Study quality, publication bias, and robustness were assessed using the Newcastle–Ottawa Scale (NOS), funnel plots, Egger’s test, and leave-one-out analyses.
Results. A total of 12 studies involving 558 patients were included. Baseline ctDNA mutation status was significantly associated with shorter PFS (HR = 1.73, 95% confidence interval (95% CI): 1.06–2.82, p = 0.03). PIK3CA mutations correlated with worse PFS (HR = 2.12, 95% CI: 1.43–3.15, p = 0.002), whereas ERBB2 mutations showed no significant association. ctDNA mutations predicted poorer PFS in tyrosine kinase inhibitor (TKI)-treated patients (HR = 2.04, 95% CI: 1.29–3.24, p = 0.002), particularly in patients receiving pyrotinib (HR = 2.77, 95% CI: 1.96–3.92, p < 0.001), but not in those receiving non-pyrotinib TKIs. Worse PFS was also observed in monotherapy (HR = 2.65, 95% CI: 1.81–3.88, p < 0.001) and capecitabine-based combination regimens (HR = 2.07, 95% CI: 1.22–3.50, p = 0.007), but not in other combination therapies.
Conclusions. Circulating tumor DNA mutation status may serve as a prognostic biomarker in patients receiving HER2-targeted therapies. PIK3CA mutations were associated with worse outcomes, whereas ERBB2 mutations showed no significant effect. The prognostic significance of ctDNA was most pronounced in patients treated with TKIs, particularly pyrotinib, and remained evident in monotherapy and capecitabine-based regimens. These findings support the potential utility of ctDNA monitoring for risk stratification and personalized management in advanced HER2-positive breast cancer.
Key words: PIK3CA, ctDNA, breast cancer, anti-HER2 therapy, TKIs
Introduction
HER2-positive breast cancer, characterized by HER2 gene amplification or overexpression, leads to continuous activation of the PI3K/AKT/mTOR and RAS/MAPK signaling pathways, resulting in increased aggressiveness and poor prognosis.1, 2, 3, 4 The advent of HER2-targeted therapies has significantly improved patient outcomes; however, individual responses vary, with some patients experiencing primary or acquired resistance, leading to reduced efficacy and disease progression.5 Current HER2-targeted therapies include monoclonal antibodies such as trastuzumab and pertuzumab, antibody-drug conjugates (ADCs) such as T-DM1 and T-DXd, and tyrosine kinase inhibitors (TKIs) including lapatinib, pyrotinib, and neratinib. Despite their efficacy across various clinical stages, resistance mechanisms are complex and involve HER2 mutations, epithelial–mesenchymal transition (EMT), and alterations in the tumor microenvironment (TME).6 Therefore, accurately predicting the efficacy of HER2-targeted treatments and dynamically monitoring patient responses are crucial for optimizing personalized treatment strategies.
Circulating tumor DNA (ctDNA), a noninvasive biomarker reflecting tumor genetic alterations, has garnered attention in the diagnosis, prognosis, and therapeutic monitoring of breast cancer.7, 8, 9 Compared with traditional tissue biopsies, ctDNA can be obtained from blood samples, offering convenience and repeatability.10, 11 Studies have indicated that dynamic changes in ctDNA may correlate with the efficacy of HER2-targeted therapies; however, its role as a consistent predictive biomarker remains controversial, particularly with respect to different HER2-targeted agents.12, 13, 14
Amplification of HER2 (also known as ERBB2) in breast cancer, as detected through tissue biopsy, has long been established as a hallmark of aggressive disease and poor prognosis. Similarly, previous studies have suggested that PIK3CA mutations identified in tissue biopsies may contribute to resistance to HER2-targeted therapies and adverse clinical outcomes.15, 16, 17, 18 However, the clinical implications of HER2 amplification and PIK3CA mutations assessed through ctDNA remain uncertain. Unlike tissue-based findings, the predictive and prognostic value of ctDNA-detected genetic alterations, including HER2 amplification and PIK3CA mutations, lacks robust validation. These uncertainties highlight the need for further evaluation of ctDNA mutations in the context of HER2-targeted therapies to better understand their clinical relevance.
Objectives
This meta-analysis aims to systematically evaluate the prognostic significance of ctDNA mutations in advanced HER2-positive breast cancer treated with HER2-targeted therapies. Specifically, we aim to explore how different gene mutations influence treatment outcomes and to clarify the predictive value of ctDNA mutations across diverse therapeutic strategies. Our findings may support clinical decision-making and contribute to the advancement of precision medicine in advanced HER2-positive breast cancer.
Materials and methods
Protocol and registration
This study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Two researchers (J.L. and H.X.) developed the protocol for this study, which was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (registration No. CRD42025638752).
Search strategy
Two researchers (J.L. and H.X.) systematically searched PubMed, Embase, and the Cochrane Library for relevant studies published before September 1, 2024. Additionally, abstracts from major annual meetings – including those of the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), and the San Antonio Breast Cancer Symposium (SABCS) – were manually reviewed for the period from March 2022 to September 2024. Search terms included Medical Subject Headings (MeSH) such as “breast cancer,” “HER2,” “TKI,” “ADC,” and “circulating tumor DNA,” along with specific drug names and agents within these categories.
Selection criteria
The inclusion criteria for this study were as follows: 1) original research articles or conference abstracts presenting primary data, including observational studies (prospective or retrospective), randomized controlled trials (RCTs), or cross-sectional studies; 2) studies enrolling breast cancer patients treated with anti-HER2 therapies, in which treatment regimens incorporated HER2-targeted agents such as trastuzumab, TKIs, or ADCs; 3) documented assessment of ctDNA, with no restrictions on detection or analytical methods due to the absence of a universally accepted standard; 4) reporting of ctDNA positivity rates along with relevant clinical outcomes, specifically progression-free survival (PFS) and/or overall survival (OS); and 5) publications available in English.
To ensure consistency across patient populations, studies were included only if HER2-positive breast cancer was defined according to ASCO/CAP guidelines, specifically as immunohistochemistry (IHC) 3+ or HER2 gene amplification confirmed with in situ hybridization (ISH). Only studies involving administration of HER2-targeted agents, including monoclonal antibodies, TKIs, or ADCs, were considered eligible.
Exclusion criteria were as follows: 1) non-original publications, such as reviews, commentaries, or editorials; studies including fewer than 5 participants; or ongoing trials lacking publicly available results; 2) studies assessing only cell-free DNA (cfDNA) without specific analysis of ctDNA; and 3) investigations not involving HER2-targeted therapies.
Data extraction
Two researchers (J.L. and H.X.) independently extracted the following data from each eligible study: authors, publication year, study location, article format, study design, patient sample size, trial phase, details of the administered HER2-targeted regimen, and reported outcomes for patients with wild-type (WT) and mutant-type (MT) ctDNA receiving anti-HER2 treatment. Any disagreements between the 2 researchers were resolved through consultation with a 3rd investigator.
Quality assessment and statistical analysis
Study quality was assessed using the Newcastle–Ottawa Scale (NOS), covering selection, comparability, and outcome domains. Scores of 6–9, 3–5, and 0–2 indicated low, moderate, and high risk of bias, respectively.19
Because clinical and methodological heterogeneity was anticipated among the included studies (differences in populations, treatment lines, ctDNA assays, and follow-up durations), a random-effects model (DerSimonian–Laird τ2 estimator with Hartung–Knapp adjustment for confidence intervals) was pre-specified as the primary analysis model for all meta-analyses. Consistent with standard meta-analytic methodology, model selection was determined a priori rather than based on heterogeneity tests (I2 or Q). For comparison and sensitivity analyses, fixed-effect models (Mantel–Haenszel method) were additionally calculated and reported when I2 < 25% to illustrate result consistency under different assumptions.
Pooled hazard ratios (HRs) and odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated. When HRs were not directly reported, they were estimated from Kaplan–Meier curves using Tierney’s method.20, 21, 22 Between-study heterogeneity was quantified using Cochran’s Q test (p < 0.10) and Higgins’ I2 statistic.
Sensitivity analyses were conducted for all meta-analyses, including the overall and subgroup analyses, by sequentially omitting individual studies (leave-one-out approach) to evaluate the robustness of the findings. Publication bias was assessed using funnel plots for all meta-analyses. Egger’s regression test was performed when ≥10 studies were included; otherwise, only visual inspection was conducted.
All analyses were performed using R v. 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria) with the meta (v6.5-0), metafor (v4.2-0), and ggplot2 (v3.5.0) packages (https://CRAN.R-project.org/package=meta; https://CRAN.R-project.org/package=metafor; https://CRAN.R-project.org/package=ggplot2). Review Manager v. 5.3 (The Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Denmark) was also used for supplementary analyses. Two-sided p < 0.05 were considered statistically significant, and an upper 95% CI < 1.0 indicated a favorable prognostic effect of WT ctDNA.
Results
Searching and screening of studies
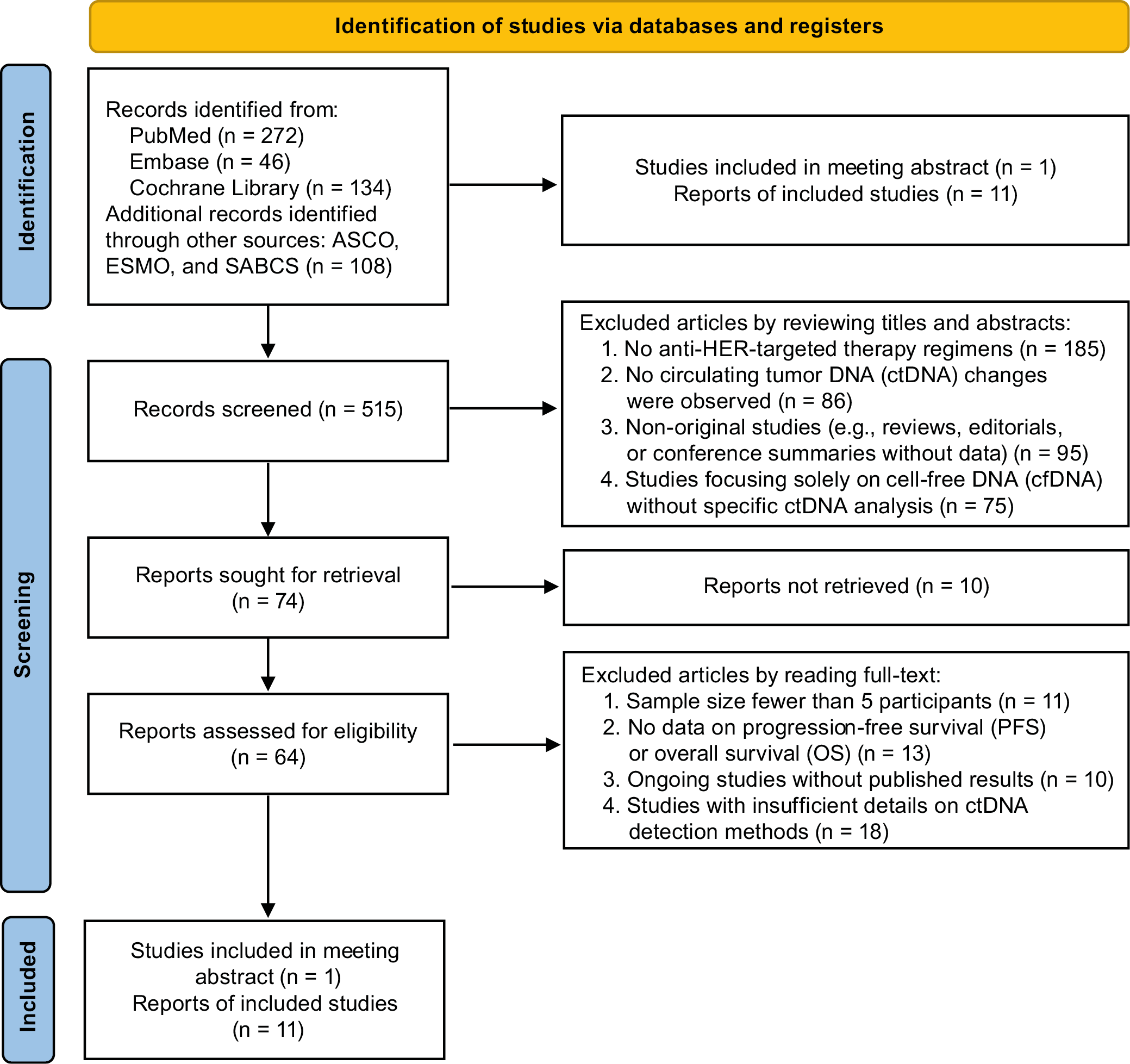
A total of 560 records were identified through the preliminary systematic literature search, and 45 duplicate records were automatically identified and removed. After assessment and screening, 515 records were considered irrelevant and excluded. Among the 12 included reports, 11 were published full-text articles and one was an abstract presented at an annual conference, comprising a total of 558 patients.23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34 The study selection process is depicted in Figure 1. The flow diagram was developed in accordance with the PRISMA guidelines.35
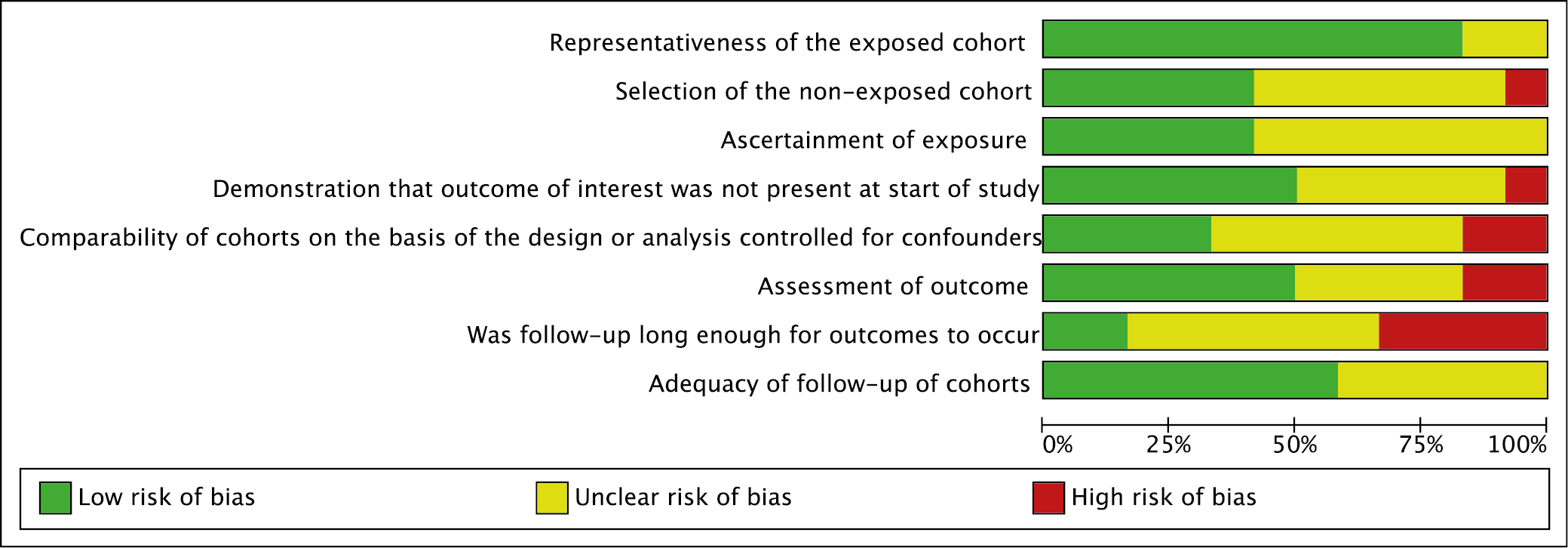
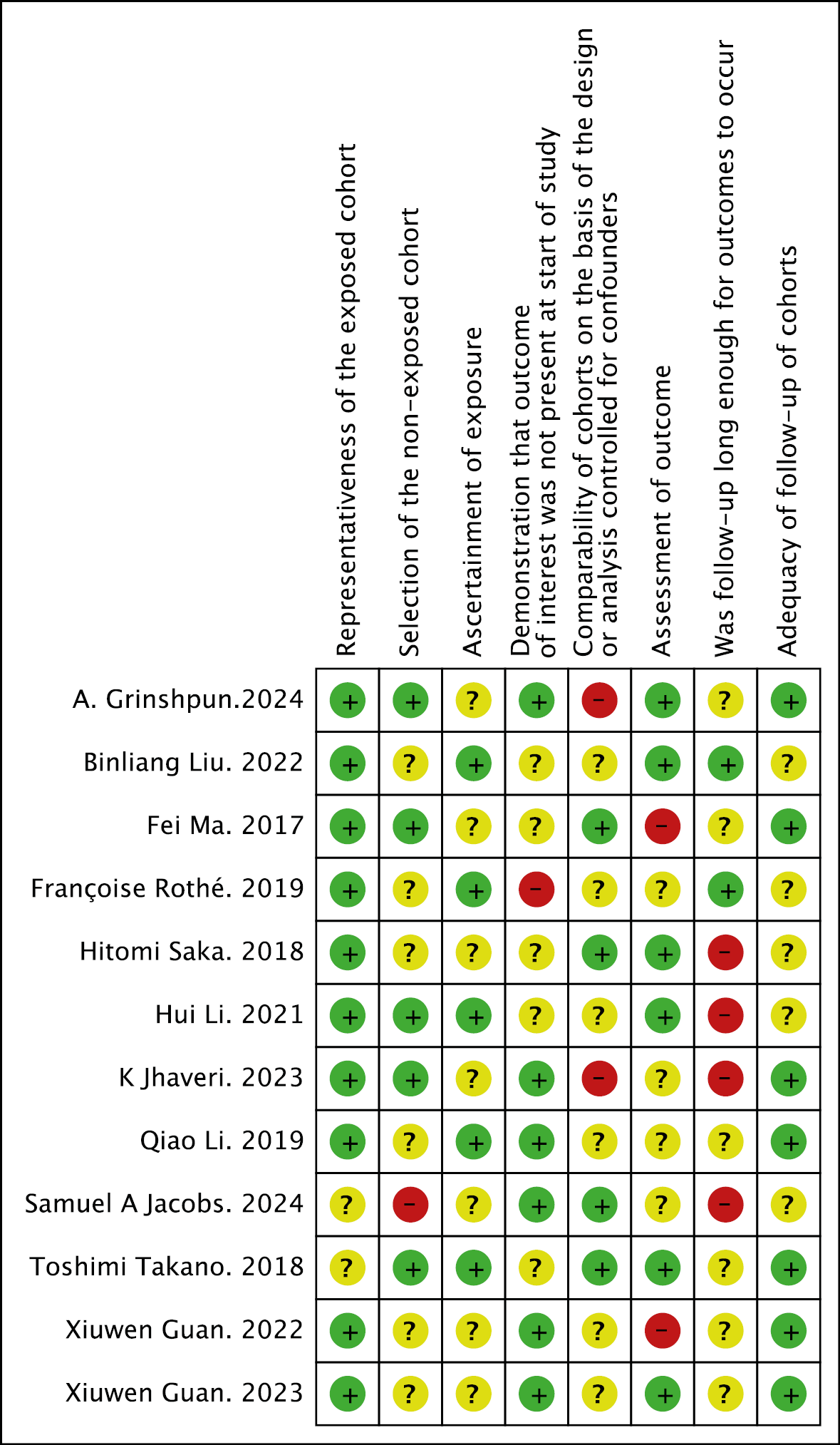
The NOS appraisal is illustrated in Figure 2 (study-level “risk-of-bias summary”) and Figure 3 (domain-level “risk-of-bias graph”). More than 80% of the judgments for core domains – such as representativeness of the exposed cohort, ascertainment of exposure, and outcome assessment – were rated as low risk (green bars). By contrast, approx. 40% of the ratings for selection of the non-exposed cohort fell into the unclear-risk category (yellow bars), reflecting the frequent absence of an explicitly matched comparison group. Truly high-risk assessments were rare, accounting for no more than approx. 10% of the scores and occurring mainly in the item related to control for additional confounders. Overall, these data indicate that the methodological quality of the included studies was acceptable: most investigations satisfied the principal NOS criteria, although future studies should improve cohort comparability and confounder adjustment.
Characteristics of the included studies
Supplementary Table 1 presents the characteristics and outcomes of 12 included studies encompassing a total of 558 patients. Most studies were retrospective or cohort studies (n = 10), with a median sample size of 42 (range: 16–107). Treatment regimens varied widely and included trastuzumab (n = 1 study), TKIs (n = 8 studies), and ADCs (T-DM1; n = 3 studies), frequently combined with capecitabine or taxanes. Circulating tumor DNA mutations were detected in 8.57% to 84.20% of patients. Patients with ctDNA mutations consistently exhibited shorter PFS, with HRs ranging from 0.33 to 5.62 across different therapies. In contrast, WT ctDNA was associated with better clinical outcomes, highlighting its prognostic significance.
Prognostic association of ctDNA mutation status with PFS in HER2-targeted therapy
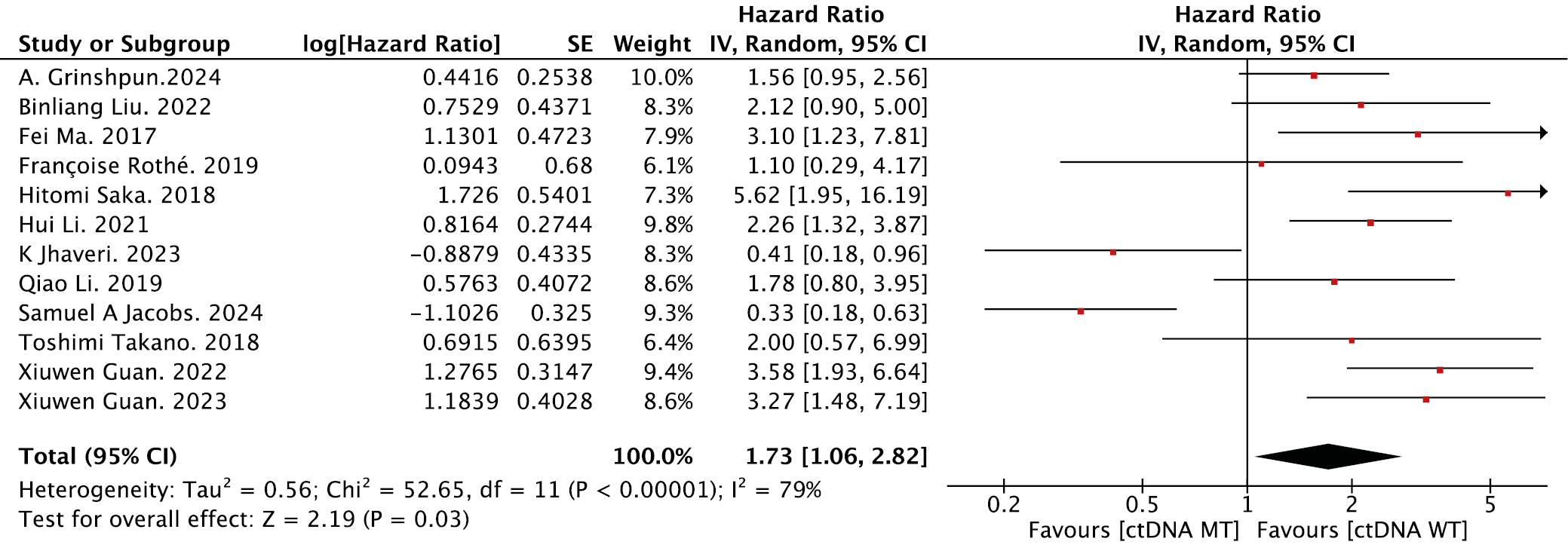
As shown in Figure 4, the forest plot illustrates the association between ctDNA mutation status and PFS in patients receiving HER2-targeted therapy. Using a pre-specified random-effects model, the pooled HR was 1.73 (95% CI: 1.06–2.82, p = 0.03), indicating that patients with ctDNA mutations had significantly shorter PFS compared with those harboring WT ctDNA.
Prognostic impact of ctDNA mutation subtypes in HER2-positive breast cancer
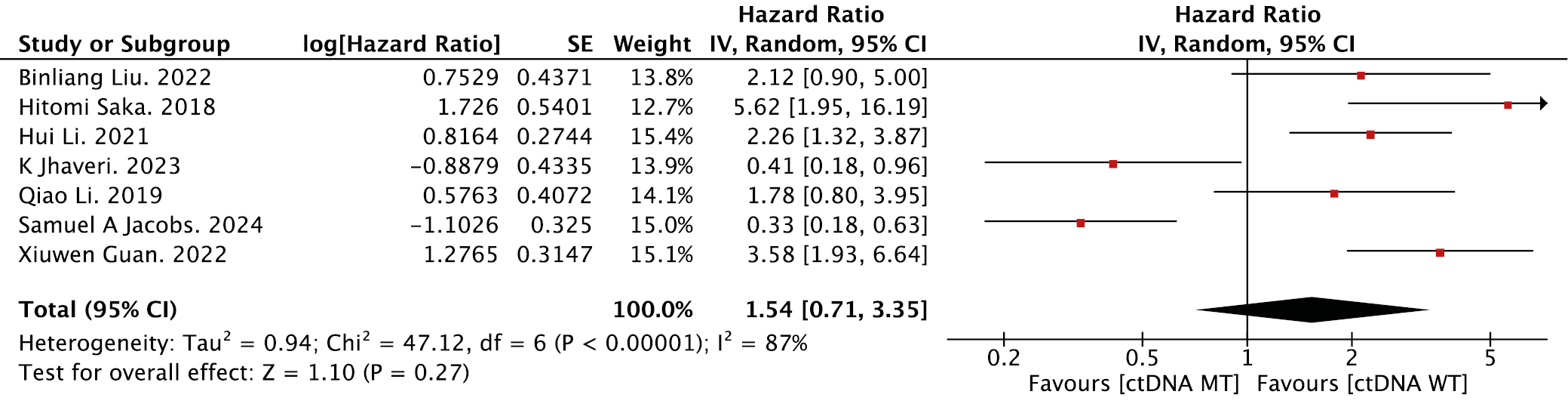
As shown in Figure 5, PIK3CA mutations were significantly associated with reduced PFS in patients receiving HER2-targeted therapy (pooled HR = 2.12, 95% CI: 1.43–3.15, p = 0.002). This finding suggests that PIK3CA mutation status may serve as a biomarker for predicting early disease progression during HER2-targeted therapy. In contrast, ERBB2 mutation status showed no statistically significant association with PFS (HR = 1.54, 95% CI: 0.71–3.35, p = 0.27; Figure 6).
Prognostic value of ctDNA mutations in TKI-based treatment regimens
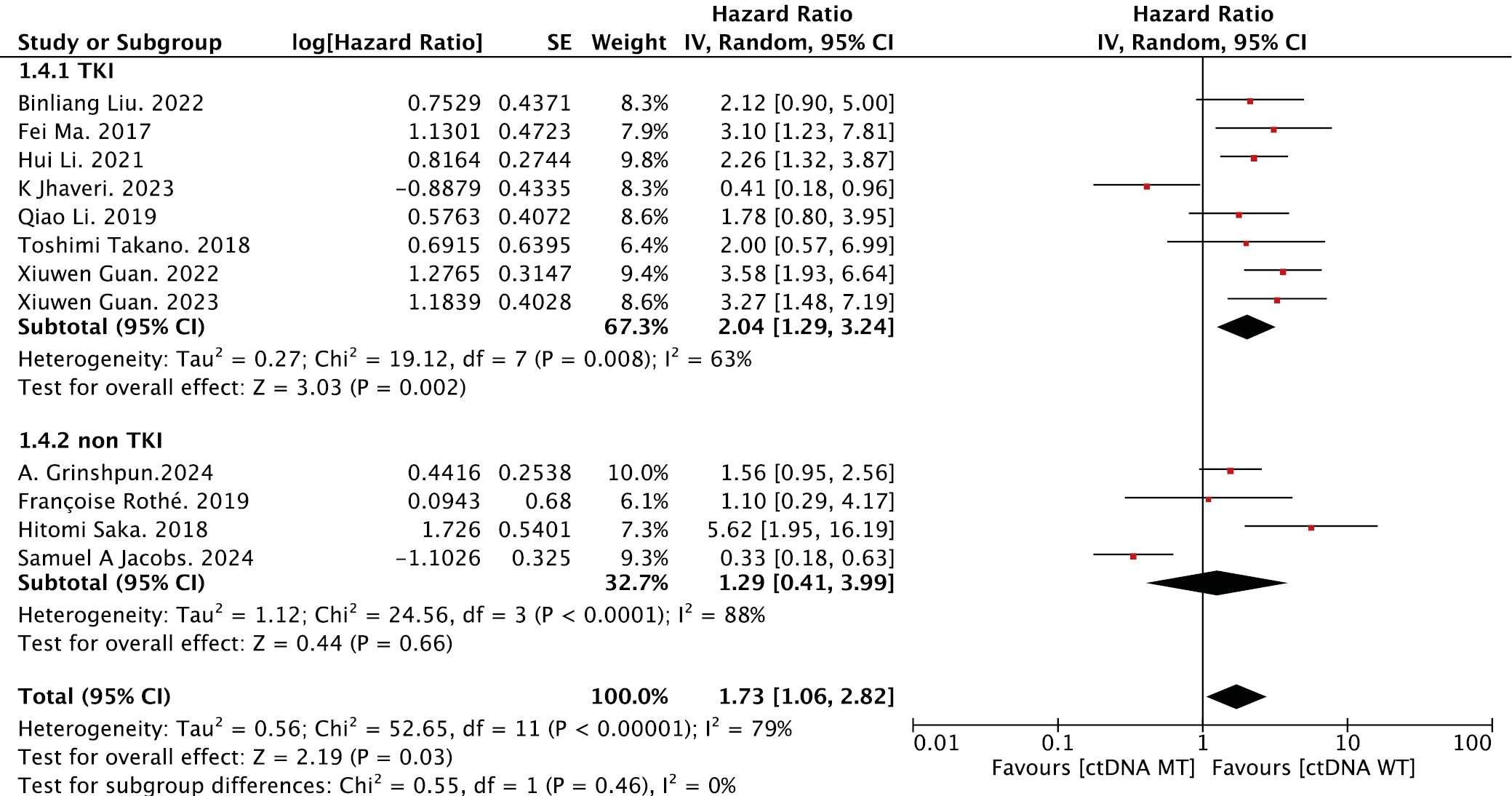
The prognostic role of ctDNA mutations was further analyzed in the context of TKI regimens (Figure 7). In the overall TKI-treated cohort (n = 8 studies), ctDNA mutation positivity was significantly associated with shorter PFS (HR = 2.04, 95% CI: 1.29–3.24, p = 0.002), whereas no such association was observed in non-TKI-treated patients (HR = 1.29, 95% CI: 0.41–3.99, p = 0.66). Notably, this predictive effect differed substantially between TKI subtypes. For patients receiving pyrotinib (n = 5 studies), ctDNA mutations strongly predicted reduced PFS (HR = 2.77, 95% CI: 1.96–3.92, p < 0.001), with consistent directional trends across studies (Figure 8). In contrast, non-pyrotinib TKIs (e.g., lapatinib and neratinib; n = 3 studies) showed no significant association between ctDNA status and PFS (HR = 1.23, 95% CI: 0.38–3.91, p = 0.73). These findings demonstrate subtype-specific associations between ctDNA mutations and PFS in TKI-treated cohorts, with the strongest effect observed in the pyrotinib subgroup.
Prognostic significance of ctDNA mutations across treatment combinations
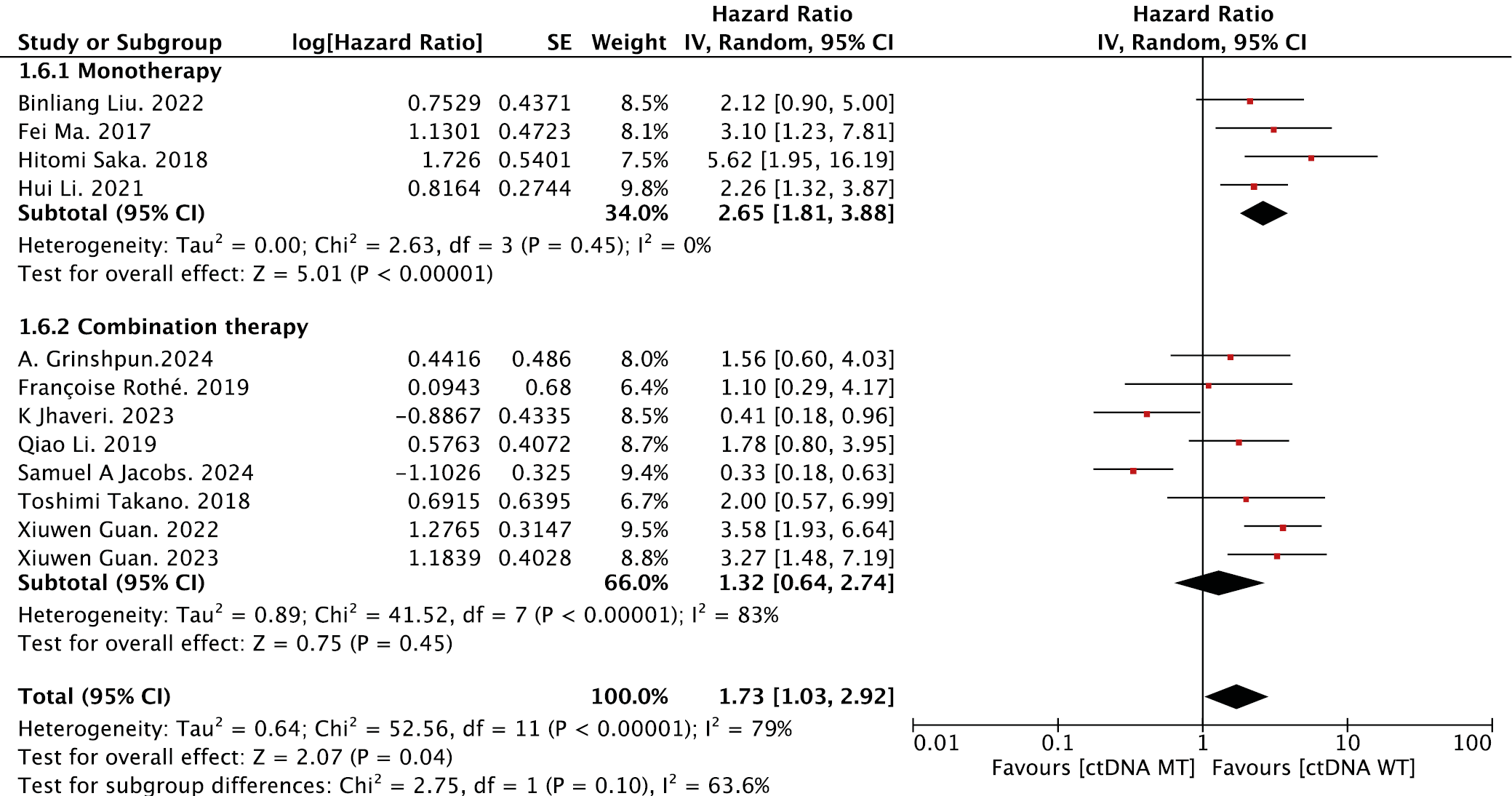
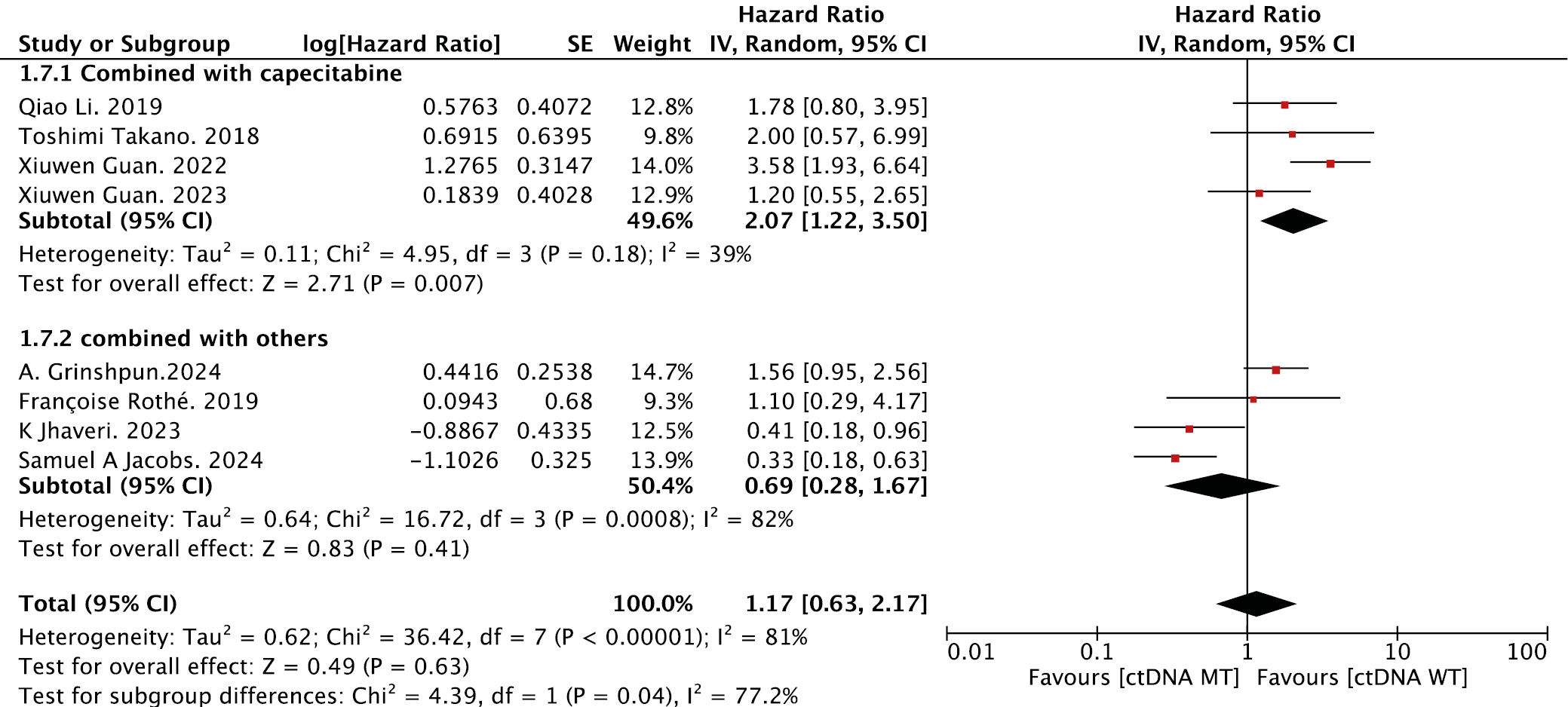
The prognostic value of ctDNA mutations was evaluated across treatment strategies (Figure 9). In monotherapy cohorts, ctDNA mutation positivity was strongly associated with shorter PFS compared with WT cases (HR = 2.65, 95% CI: 1.81–3.88, p < 0.001). In contrast, combination therapy overall showed no significant difference in PFS between mutation-positive and mutation-negative groups (HR = 1.32, 95% CI: 0.64–2.74, p = 0.45). Further stratification of combination regimens revealed divergent effects. For capecitabine-based combinations (n = 4 studies), ctDNA mutations predicted markedly reduced PFS (HR = 2.07, 95% CI: 1.22–3.50, p = 0.007), whereas non-capecitabine combinations (e.g., taxane- or paclitaxel-based regimens; n = 4 studies) showed no association (HR = 0.69, 95% CI: 0.28–1.67, p = 0.41; Figure 10).
Sensitivity and publication-bias analyses for the overall and subgroup meta-analyses
The leave-one-out sensitivity analysis demonstrated that sequential omission of any single study did not materially change the effect direction or statistical significance of the pooled estimate (Supplementary Fig. 1). The overall estimates remained stable and within a narrow confidence interval (95% CI: 1.01–2.97), with no significant shifts in the hazard ratio (HR = 1.73). Publication bias assessment is shown in Supplementary Fig. 2. Egger’s linear regression test detected no significant funnel plot asymmetry (t = 0.32, degrees of freedom (df) = 10, p = 0.796), indicating no evident small-study effects; the bias estimate was 0.7605 (standard error (SE) = 2.3438).
For all 10 predefined subgroups, the same leave-one-out sensitivity analyses and funnel plot evaluations were performed (Supplementary Fig. 3–22; mapping: ERBB2 (Supplementary Fig. 3,4), PIK3CA (Supplementary Fig. 5,6), TKI (Supplementary Fig. 7,8), non-TKI (Supplementary Fig. 9,10), pyrotinib (Supplementary Fig. 11,12), non-pyrotinib (Supplementary Fig. 13,14), monotherapy (Supplementary Fig. 15,16), combination therapy (Supplementary Fig. 17,18), capecitabine-based combinations (Supplementary Fig. 19,20), and other combinations (Supplementary Fig. 21,22). Across subgroups, the pooled HRs remained directionally consistent, and significance judgments were not materially altered after omission of any single study, supporting the robustness of the findings. Because each subgroup included ≤10 studies, visual inspection of funnel plots was performed without formal Egger testing; no obvious asymmetry was observed.
Discussion
This meta-analysis evaluated the clinical significance of ctDNA mutations in assessing the efficacy of anti-HER2 therapies in breast cancer, providing important insights into their potential role as biomarkers of therapeutic response and prognosis. The pooled analysis demonstrated a significant association between ctDNA mutations and shorter PFS across HER2-targeted therapies. These findings align with previous studies reporting that ctDNA mutations correlate with poor clinical outcomes, reinforcing their potential role in guiding personalized treatment strategies.36 Among these, PIK3CA mutations showed a strong correlation with reduced PFS, which is consistent with existing evidence suggesting that activation of the PI3K/AKT/mTOR signaling pathway contributes to resistance to HER2-targeted therapies.37
This underscores the clinical relevance of detecting PIK3CA mutations via liquid biopsy as predictive biomarkers and suggests that patients harboring these mutations may benefit from treatment intensification, such as the incorporation of PI3K inhibitors. Notably, several ongoing clinical trials (e.g., NCT04208178 and NCT02038010) are investigating combinations of HER2-targeted agents and PI3K inhibitors, supporting the concept that dual blockade may help overcome resistance and improve patient outcomes. A key finding of this study is that the predictive value of ctDNA mutations was particularly evident in patients receiving TKI therapy, especially those treated with pyrotinib, suggesting that ctDNA analysis may assist in optimizing patient selection and informing timely treatment adjustments in this context. In contrast, this predictive effect was not observed in patients receiving T-DM1, which is consistent with previous studies reporting the limited predictive value of ctDNA mutations in this treatment setting.38, 39 This may be attributed to the cytotoxic mechanism of T-DM1, which depends predominantly on intracellular drug release rather than HER2 signaling inhibition, thereby diminishing the impact of PIK3CA mutations on therapeutic efficacy.
Additionally, ctDNA mutations exhibited stronger predictive value in monotherapy than in combination therapies, where their predictive role was less pronounced. This may be attributed to the ability of combination treatments to counteract the effects of single-gene alterations through multiple mechanisms. However, in capecitabine-based regimens, ctDNA mutations remained a significant predictor of shorter PFS, suggesting that certain resistance mechanisms persist in this therapeutic setting.
Although ERBB2 mutations detected in tissue biopsies have been well established as markers of resistance and poor prognosis in HER2-positive breast cancer, our analysis did not demonstrate a significant association between ERBB2 mutations identified in ctDNA and PFS. This discrepancy likely reflects the inherent limitations of liquid biopsy compared with tissue-based methods. While tissue biopsy offers a static, localized snapshot of tumor genomic alterations, ctDNA reflects dynamic tumor burden and clonal evolution, which may be influenced by tumor heterogeneity, variable cfDNA shedding, assay sensitivity, and the type of therapy administered (such as TKIs or ADCs).40, 41 The use of pan-HER TKIs, particularly pyrotinib, may partially overcome downstream HER2 pathway alterations, thereby mitigating the negative prognostic impact of ERBB2 mutations detected in plasma. Additionally, methodological heterogeneity, variability in therapeutic regimens, and limited sample sizes in the included studies could have contributed to these findings. Future research involving larger cohorts, standardized ctDNA detection protocols, and stratification by treatment type will be necessary to clarify the predictive value of ERBB2 mutations in liquid biopsy. Nevertheless, ctDNA testing offers unique advantages over tissue biopsy, including its noninvasive nature, the ability to capture real-time tumor dynamics, and the potential for longitudinal monitoring of resistance mechanisms in clinical practice.42, 43
From a clinical perspective, liquid biopsy offers distinct advantages over traditional tissue biopsy by enabling real-time and repeatable assessment of treatment response and resistance development. This study supports the potential role of ctDNA in guiding treatment decisions, particularly in TKI- and pyrotinib-treated patients. However, the predictive value of ctDNA varies across treatment regimens; therefore, integration of multiple biomarkers may improve predictive accuracy in the future.44, 45 Additionally, previous studies have reported that ctDNA detection rates correlate with metastatic tumor burden, with higher detection frequencies observed in patients with multiple or visceral metastases.46, 47, 48, 49 Our meta-analysis focused on the predictive role of ctDNA mutations and did not include tumor burden analysis. Future research should consider incorporating this factor to enhance the clinical utility of ctDNA. Future studies should also focus on standardizing ctDNA detection methods, validating these findings through prospective clinical trials, and leveraging longitudinal monitoring to refine precision oncology approaches for HER2-positive breast cancer.
Limitations of the study
Several limitations should be acknowledged. First, the included studies predominantly enrolled patients with advanced HER2-positive breast cancer, but variations in disease stage and prior treatments may have introduced heterogeneity. Second, ctDNA detection methods varied across studies, potentially affecting mutation rates and prognostic interpretation. Third, limited sample sizes and inconsistent reporting of baseline tumor burden reduced the ability to perform subgroup analyses for certain regimens. Fourth, ERBB2 mutation analysis lacked statistical significance, possibly due to low mutation frequency and variable detection sensitivity. Finally, the observational nature of most included studies limits causal inference. Future prospective trials with standardized ctDNA methodologies and larger cohorts are needed to validate these findings in the context of advanced disease.
Conclusions
The mutational status of ctDNA holds promise as a prognostic biomarker in patients with HER2-positive breast cancer receiving targeted therapy. Specifically, PIK3CA mutations were consistently associated with worse survival outcomes, whereas ERBB2 mutations did not demonstrate independent prognostic significance based on current evidence. The prognostic impact of ctDNA was most evident in patients treated with TKIs, particularly those receiving pyrotinib. Notably, this association remained significant in both monotherapy and capecitabine-based combination regimens. These findings support the use of ctDNA mutation profiling for risk stratification and personalized decision-making in the context of HER2-targeted therapy.
Supplementary data
The supplementary materials are available at: https://doi.org/10.5281/zenodo.17541159. The package contains the following files:
Supplementary Table 1. Summary of included studies evaluating the prognostic value of ctDNA mutation status in HER2-targeted therapy for breast cancer.
Supplementary Fig. 1. Leave-one-out sensitivity analysis for the overall PFS meta-analysis.
Supplementary Fig. 2. Funnel plot for publication bias in the overall PFS meta-analysis.
Supplementary Fig. 3. Sensitivity analysis of ERBB2 subgroup.
Supplementary Fig. 4. Funnel plot of ERBB2 subgroup.
Supplementary Fig. 5. Sensitivity analysis of PIK3CA subgroup.
Supplementary Fig. 6. Funnel plot of PIK3CA subgroup.
Supplementary Fig. 7. Sensitivity analysis of the TKI subgroup.
Supplementary Fig. 8. Funnel plot of the TKI subgroup.
Supplementary Fig. 9. Sensitivity analysis of the non-TKI subgroup.
Supplementary Fig. 10. Funnel plot of the non-TKI subgroup.
Supplementary Fig. 11. Sensitivity analysis of the pyrotinib subgroup.
Supplementary Fig. 12. Funnel plot of the pyrotinib subgroup.
Supplementary Fig. 13. Sensitivity analysis of the non-pyrotinib subgroup.
Supplementary Fig. 14. Funnel plot of the non-pyrotinib subgroup.
Supplementary Fig. 15. Sensitivity analysis of monotherapy subgroup.
Supplementary Fig. 16. Funnel plot of monotherapy subgroup.
Supplementary Fig. 17. Sensitivity analysis of combination subgroup.
Supplementary Fig. 18. Funnel plot of combination subgroup.
Supplementary Fig. 19. Sensitivity analysis of capecitabine-based subgroup.
Supplementary Fig. 20. Funnel plot of capecitabine-based subgroup.
Supplementary Fig. 21. Sensitivity analysis of other combination subgroup.
Supplementary Fig. 22. Funnel plot of other combination subgroup.
Use of AI and AI-assisted technologies
Not applicable.