Abstract
Background. Postoperative urinary tract infection (UTI) following pyeloplasty remains a significant complication and continues to pose challenges in pediatric urological care.
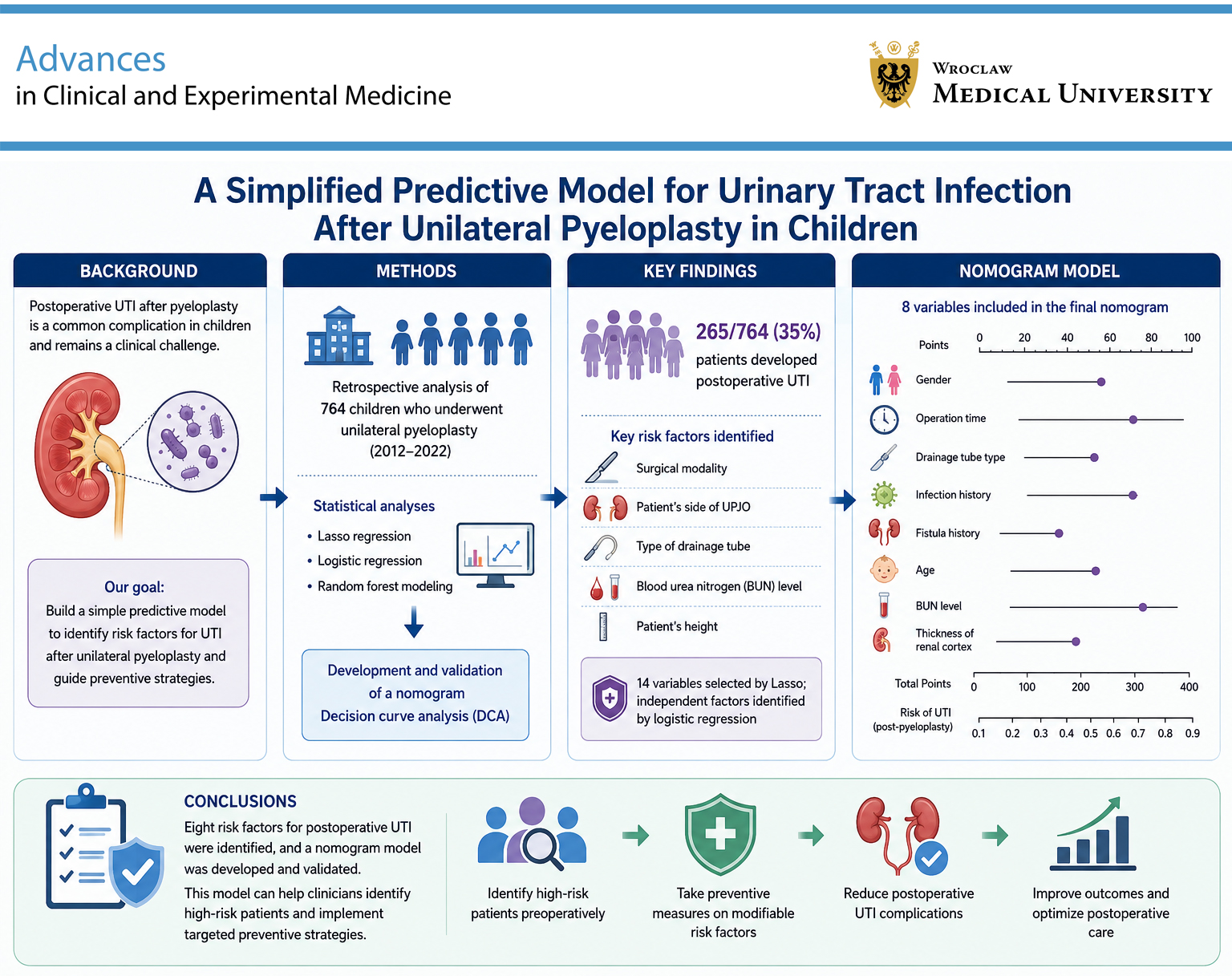
Objectives. This study aimed to develop a simplified predictive model to identify risk factors for postoperative UTI after unilateral pyeloplasty and to support clinicians in implementing preventive strategies targeting modifiable risk factors.
Materials and methods. Clinical data from children who underwent unilateral pyeloplasty at the Children’s Hospital of Capital Institute of Pediatrics (Beijing, China) between January 2012 and January 2022 were retrospectively analyzed. Variables including sex, age, body mass index (BMI), surgical modality, drainage tube type, and parameters from blood and urine tests were evaluated. Statistical analyses, including least absolute shrinkage and selection operator (LASSO) regression, logistic regression, and random forest modeling, were performed to identify significant predictive factors. Variables with the greatest predictive importance were used to develop a nomogram, and its clinical utility was evaluated using decision curve analysis (DCA).
Results. Among 764 patients, 265 (35%) developed postoperative UTI. Key risk factors included surgical modality, laterality of ureteropelvic junction obstruction (UPJO), drainage tube type, blood urea nitrogen (BUN) level, and patient height. LASSO regression identified 14 predictive variables, while logistic regression determined independent risk and protective factors. Ultimately, 8 variables (e.g., sex, operative time, drainage tube type, history of infection, history of fistula, age, BUN level, and renal cortical thickness) were selected for development of the nomogram predicting postoperative UTI risk after unilateral pyeloplasty.
Conclusions. This study identified 8 factors associated with postoperative UTI following unilateral pyeloplasty in children. The developed predictive model may assist clinicians in identifying high-risk patients, thereby supporting improved perioperative planning and postoperative management.
Key words: risk factors, urinary tract infection, prediction model, unilateral pyeloplasty
Background
Ureteropelvic junction obstruction (UPJO) is defined as an obstruction at the junction between the kidney and ureter, resulting in decreased urine flow from the renal pelvis to the ureter. Ureteropelvic junction obstruction is one of the main causes of infantile hydronephrosis. If left untreated, it may lead to hydronephrosis, chronic infection, or urolithiasis and may ultimately result in progressive renal insufficiency.1 Ureteropelvic junction obstruction may be either congenital or acquired, and endogenous and exogenous risk factors include urolithiasis, postoperative, inflammatory, or ischemic stenosis, fibroepithelial polyps, adhesions, and malignant tumors.
A variety of treatment options are available for UPJO; however, surgery remains the gold standard, particularly when urinary drainage does not improve after 18 months of age. Surgical management of UPJO has advanced considerably over recent decades, evolving from open pyeloplasty (OP) to laparoscopic pyeloplasty (LP) and robotic-assisted laparoscopic pyeloplasty (RALP). Although minimally invasive approaches have gained increasing acceptance in the treatment of UPJO, OP as originally described by Anderson and Hynes, remains the standard surgical treatment, with reported long-term success rates exceeding 90%.2 Compared with traditional OP, LP offers advantages such as faster recovery, shorter hospitalization, and fewer complications, whereas OP is often associated with shorter operative time.3 However, some studies have reported shorter operative times for LP compared with OP.4 Indications for surgical treatment of UPJO include worsening hydronephrosis during surveillance, patient-reported symptoms such as flank pain, recurrent urinary tract infection (UTI), persistent or poorly controlled hypertension, and reduced or declining differential renal function, typically defined as ipsilateral renal function <40% on diuretic renography.5, 6
However, despite its high success rate, surgical treatment of UPJO is not without complications. The main postoperative complications include UTI, urinary extravasation or leakage, pyelonephritis, bleeding, and recurrent UPJO.7 Among these, postoperative UTI remains a frequent and clinically challenging complication for pediatric urologists.
Urinary tract infection, most commonly caused by Escherichia coli, is one of the most common bacterial infections in children.8 Its incidence is higher in boys than in girls during the 1st year of life (3.7% vs 2.0%), whereas after infancy it becomes more common in girls.9 Previous studies have identified several risk factors for pediatric UTI, including male sex, body weight, elevated blood urea nitrogen (BUN) levels, recurrent UTI within 3 months, prolonged catheter retention, double-J stent placement, and bilateral double-J stent retention.10, 11 However, relatively few studies have specifically investigated risk factors for UTI following unilateral pyeloplasty, particularly in large pediatric cohorts.
Objectives
We aimed to develop a predictive model for UTI after unilateral pyeloplasty in children at a large Chinese center, which may help reduce the incidence of postoperative UTI and provide a reliable reference for the management of UTI in children after unilateral pyeloplasty.
Materials and methods
Patients
Clinical data of children who underwent unilateral pyeloplasty at the Children’s Hospital of the Capital Institute of Pediatrics (Beijing, China) between January 2012 and January 2022 were retrospectively analyzed. Patient data were retrieved in May 2023. Inclusion criteria were as follows: 1) children undergoing unilateral pyeloplasty for the first time; 2) patients meeting the diagnostic criteria for UPJO according to the European Association of Urology (EAU) guidelines; and 3) patients with complete follow-up data. Exclusion criteria were as follows: 1) patients with bilateral hydronephrosis; 2) patients who received a double-J stent (internal drainage) and temporary pyelostomy fistula (external drainage) simultaneously; 3) patients with multiple congenital urinary tract strictures; 4) patients with duplicated kidneys or double ureters; 5) patients whose parients or legal guardians refused participation in the study or declined to sign the informed consent form; and 6) patients with incomplete follow-up data. The study protocol was approved by the Institutional Review Board of the Children’s Hospital of the Capital Institute of Pediatrics (approval No. SHIERILM2025005) before commencement of the study, and all patients’ guardians signed informed consent forms. Written informed consent for participation in the study and publication of potentially identifiable images or data was obtained from all parents.
Variables
Variables including sex, age, height, weight, body mass index (BMI), surgical modality, indwelling drainage tube type (double-J stent or pyelostomy fistula), serum creatinine (Cr), BUN, estimated glomerular filtration rate (eGFR), neutrophil percentage (N%), lymphocyte percentage (L%), neutrophil-to-lymphocyte ratio (N/L), anterior-posterior diameter of the renal pelvis (APD), caliectasis, and renal cortical thickness were analyzed in this study.
Postoperative UTI definition
Postoperative UTI was defined according to the 2015 EAU guidelines on UTI12 and the 2016 evidence-based guidelines on UTI issued by the Urology Branch of the Chinese Medical Association.13 Specifically, postoperative UTI included patients presenting with symptoms such as fever, turbid urine, abnormal urine color, hematuria, urinary retention, urinary incontinence, urinary frequency, urinary urgency, dysuria, or interrupted urination. In addition, the definition required 2 consecutive routine urine test results showing a white blood cell (WBC) count >5/high-power field (HPF). Furthermore, at least 1 of the following criteria had to be fulfilled: 1) urine culture showing >103 colony-forming units (CFU)/mL of uropathogens in patients with urinary catheters; or 2) urine culture showing >105 CFU/mL of uropathogens regardless of catheter use. Asymptomatic bacteriuria was defined as the presence of a positive urine culture in patients without symptoms, accompanied by a urine test showing a WBC count >5/HPF.
Preventative measures
All patients received cefuroxime sodium (30 mg/kg/day divided into 3–4 doses) and ceftriaxone sodium (20–80 mg/kg/day) for 2 days before surgery. In addition, all patients received postoperative intravenous anti-inflammatory treatment. A Foley catheter was retained during surgery and removed 3–5 days postoperatively. A double-J stent was placed during surgery and removed 8 weeks postoperatively. In this study, postoperative UTI was defined as UTI occurring within 8 weeks after surgery.
Statistical analyses
The statistical analysis was carried out using R v. 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) and IBM SPSS v. 23.0 (IBM Corp., Armonk, USA). Prior to model construction, comprehensive assumption checks were performed. Variance inflation factors (VIFs) were calculated for all variables, with generalized VIF values for categorical variables ranging from 1.12 to 3.47 (Supplementary Table 1), confirming the absence of multicollinearity (VIF < 5). Box–Tidwell tests demonstrated linearity in the logit for continuous variables (p = 0.213–0.586), and Shapiro–Wilk tests confirmed normality for all continuous variables (p > 0.05). Results of these tests are presented in Supplementary Table 1. Continuous variables with skewed distributions are presented as median [Q1–Q3], whereas normally distributed variables (e.g., albumin) are shown as mean ± standard deviation (SD).
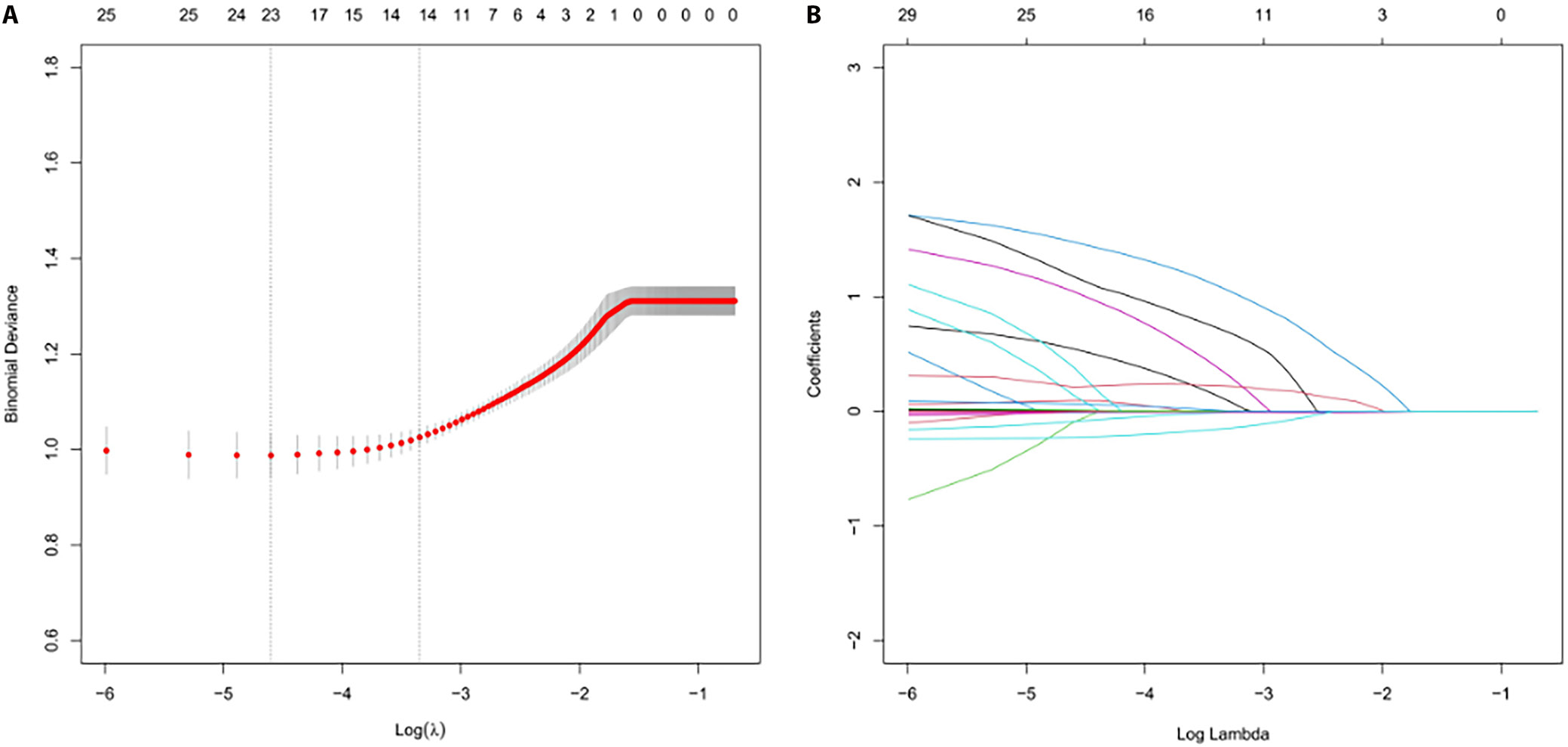
Participants were randomly divided into training (70%) and validation (30%) datasets. The random seed was set to 20230815 (set.seed(20230815) in R) prior to data partitioning to ensure reproducibility. The least absolute shrinkage and selection operator (LASSO) regression was applied exclusively for variable selection. Ten-fold cross-validation was used to optimize the penalty parameter (λ), with the optimal λ (λ_min = 0.032) selected according to the minimum partial likelihood deviance. LASSO model settings included a maximum of 1,000 iterations and a convergence tolerance of 1 × 10–4. All 23 candidate variables (listed in Table 1) were included, and variables with non-zero coefficients were retained.
Variables selected with LASSO were entered into a multivariable logistic regression model. Univariable analysis was intentionally omitted to avoid biased variable selection and contradictory results. Model discrimination was assessed using the area under the receiver operating characteristic (ROC) curve (AUC). Calibration was evaluated using the Hosmer–Lemeshow test and calibration plots with 1,000 bootstrap resamples. Clinical utility was quantified through decision curve analysis (DCA) across probability thresholds ranging from 0% to 100%. Post hoc power analysis using G*Power 3.1 demonstrated 98.7% power to detect an odds ratio (OR) >2.0 at α = 0.05. Bootstrap validation using 1,000 resamples showed consistent OR estimates within ±5% of the original values.
Results
Patients’ demographic and clinical characteristics
A total of 764 patients were included, of whom 265 (34.7%) developed postoperative UTI. The UTI group consisted predominantly of males (86.0% vs 79.4% in the non-UTI group) and younger children (median age: 7.3 months [3.9–24.0] vs 36.0 months [11.0–72.0]). Laparoscopic pyeloplasty was performed more frequently in patients with UTI (58.9% vs 37.9%), whereas OP was more common in the non-UTI group (62.1% vs 41.1%). Double-J stent use was markedly higher in the UTI group (79.2% vs 44.1%), and renal cortical thickness was lower (median: 1.9 mm [1.3–2.5] vs 2.4 mm [2.0–3.4]). Key biochemical differences were also observed. Patients with UTI showed lower median BUN levels (3.2 mmol/L [2.3–4.5] vs 4.3 mmol/L [3.2–5.4]) and eGFR values (10.29 mL/min/m2 [4.9–35.6] vs 49.13 mL/min/m2 [24.9–67.6]). The N/L ratio was lower in UTI cases (0.43 [0.27–0.88] vs 0.71 [0.41–1.10]), whereas the L% was higher (62.8% [48.0–71.0] vs 53.0% [42.7–63.8]). No notable differences were observed in albumin levels (43.5 g/L [41.4–45.9] vs 43.7 g/L [41.9–45.5]) or renal pelvis APD (3.4 cm [2.7–4.3] vs 3.3 cm [2.7–3.8]). Full baseline characteristics are presented in Table 1.
Identification of predictive variables for UTI after unilateral UPJO through LASSO regression analysis
In the present study, the LASSO regression method was employed to identify significant predictive variables. By applying a penalty parameter (λ) and using 10-fold cross-validation, an optimal set of variables was selected. At the minimum value of log(λ), denoted as log(λ)_min, a random seed was set to ensure reproducibility of the results. The final model included 14 predictive variables, with coefficients presented in Table 1. The intercept coefficient was −0.610070252. The coefficient for sex (gender1) was 0.115231168, suggesting that changes in this variable were associated with changes in the risk of postoperative UTI following unilateral UPJO, while other variables remained constant. The coefficient for operative time was 0.003582231, indicating a slight increase in postoperative UTI risk with longer operative duration. The coefficient for drainage type (drainage1, 1.077044923) was the highest among all variables, indicating a strong association with postoperative UTI risk. The coefficients for infection history and fistula history were 0.351245843 and 0.71021905, respectively, suggesting positive associations with postoperative UTI risk. LASSO coefficients are regularized estimates for variable selection; their magnitude differs from logistic regression coefficients. Direction and significance were confirmed in the final model.
The coefficients for age and height were −0.00270678 and −0.004534245, respectively, indicating negative associations with postoperative UTI risk, with age showing a relatively small effect size. Other biochemical indicators, including TP, albumin/globulin (A/G) ratio, Cr, BUN, and eGFR, also had negative coefficients, suggesting that higher values were associated with lower postoperative UTI risk. The coefficient for APD was 0.006521787, indicating a positive association with postoperative UTI risk, whereas the coefficient for renal cortical thickness was −0.152582245, suggesting that thinner renal cortex was associated with increased postoperative UTI risk. Further results are presented in Table 2 and Figure 1.
Variable selection and multivariable logistic regression analysis
Employing LASSO regression with 10-fold cross-validation, 8 predictive variables were selected from 23 candidate features (Figure 1A,B). These variables were subsequently included in a multivariable logistic regression model. Double-J stent placement emerged as the strongest risk factor (OR = 6.41, 95% confidence interval (95% CI): 3.78–10.89, p < 0.001), followed by male sex (OR = 2.15, 95% CI: 1.28–3.63, p = 0.004) and history of fistula (OR = 4.26, 95% CI: 1.85–9.81, p = 0.001). Protective factors included age (OR = 0.98 per month, 95% CI: 0.97–0.99, p < 0.001), BUN level (OR = 0.85 per mmol/L, 95% CI: 0.74–0.98, p = 0.030), and renal cortical thickness (OR = 0.77 per mm, 95% CI: 0.61–0.96, p = 0.023). Variables such as A/G ratio and APD did not reach statistical significance (p > 0.05). Complete results are presented in Table 2.
Development, performance, and internal validation of the predictive nomogram
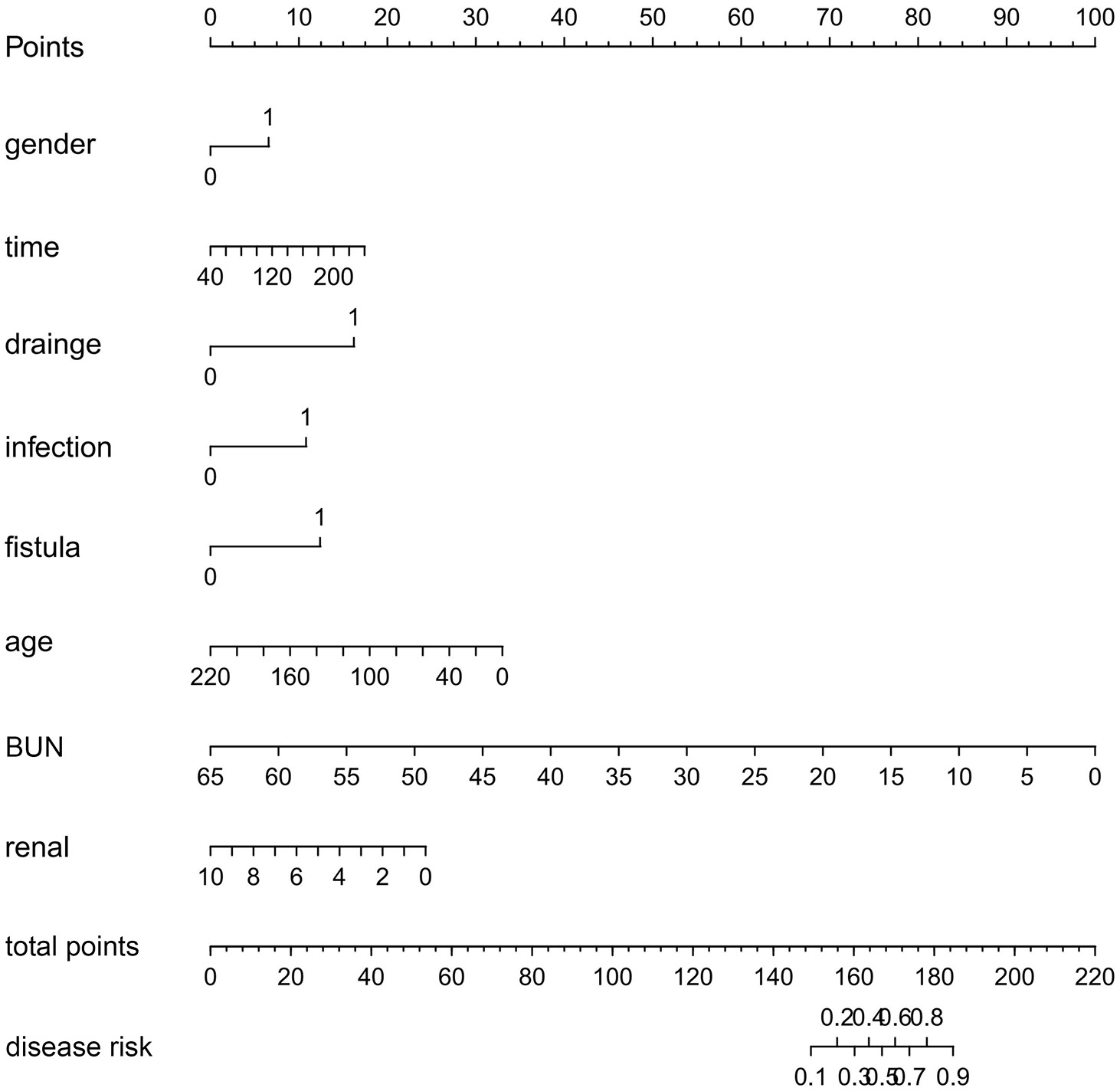
Utilizing the 8 identified predictive factors, a nomogram was developed to assess the risk of UTI after unilateral UPJO, as shown in Figure 2. The nomogram assigned scores to each variable, and the total score was calculated as the sum of the individual scores for all 8 variables. At the bottom of Figure 2, a predictive scale correlates total scores with the corresponding probabilities of postoperative UTI after unilateral UPJO. An increase in the total score indicates a higher risk of postoperative UTI.
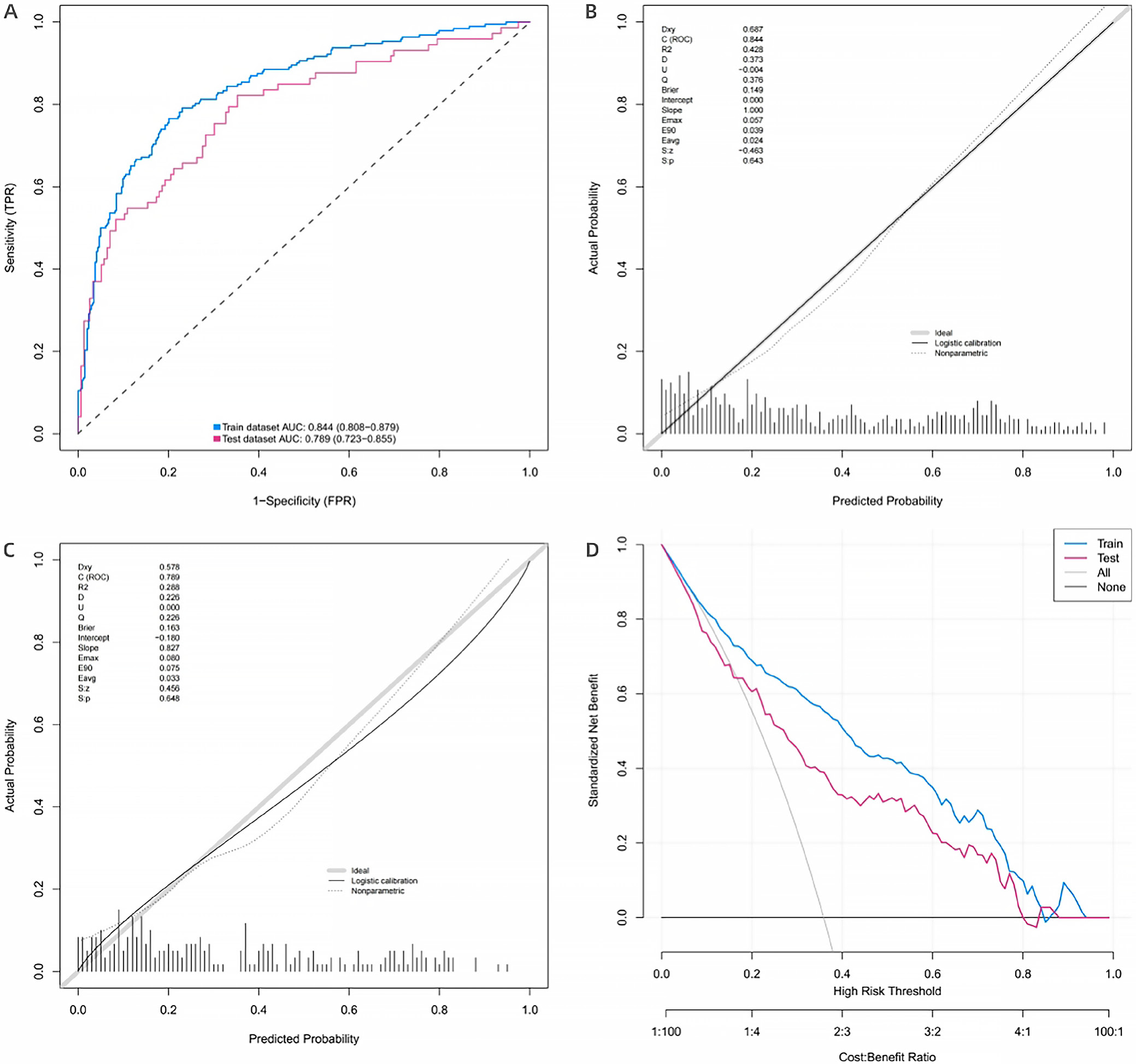
The nomogram demonstrated AUC values of 0.844 (95% CI: 0.808–0.879) and 0.789 (95% CI: 0.723–0.855) in the training and validation datasets, respectively (Figure 3A). Calibration plots for both cohorts closely aligned with the ideal curve after bias correction, indicating good agreement between predicted probabilities and observed outcomes (Figure 3B,C). Furthermore, the Hosmer–Lemeshow test yielded a p-value of 0.666, supporting adequate model calibration. The DCA demonstrated significant net clinical benefit across threshold probabilities ranging from 9% to 89% (Figure 3D). Collectively, these findings support the discriminative performance, calibration, clinical utility, and potential generalizability of the nomogram.
Discussion
Ureteropelvic junction obstruction is defined as a blockage at the junction between the renal pelvis and the ureter, with an estimated incidence of 1 per 1,000–1,500 individuals.7 It is more common in boys than in girls and represents the most frequent cause of antenatally detected hydronephrosis, accounting for approx. 80% of cases.14 At present, surgical treatment remains the gold standard for UPJO, with reported long-term success rates exceeding 90%. Surgical management of UPJO has advanced considerably over recent decades, from the introduction of OPin 189215 to the development of LP in 1993,16 followed by RALP in 2002.17
Despite the high success rate of pyeloplasty, postoperative complications remain clinically important. The 2 most common complications include UTI and prolonged urinary leakage. Among these, postoperative UTI remains a frequent and challenging complication in pediatric urology. Therefore, identifying children at high risk of postoperative UTI before pyeloplasty is important for implementing preventive strategies targeting modifiable risk factors and improving postoperative management.
The present study developed a simplified predictive model to identify risk factors for postoperative UTI and assist clinicians in implementing preventive strategies. To our knowledge, this study includes one of the largest datasets evaluating pediatric UTI following unilateral pyeloplasty. The predictive model identified open surgery, left-sided UPJO, double-J stent placement, low BUN levels, and shorter height as major factors associated with postoperative UTI risk. Previous studies have reported double-J stent placement, elevated BUN levels, and shorter height as potential risk factors.18, 19 However, laterality has not previously been reported as a risk factor. In the present study, patients with left-sided UPJO were more likely to develop postoperative UTI. One possible explanation is that approx. 60% of UPJO cases are left-sided,20 which is consistent with the findings of this study (right-sided UPJO: 33%; left-sided UPJO: 67%). Furthermore, the left ureter is generally slightly longer than the right ureter, which may contribute to greater urinary stasis and increased susceptibility to urinary reflux and infection.
In the present study, 265 (35%) children developed postoperative UTI, which is markedly higher than the previously reported rates of 7.8–10%,21, 22 but slightly lower than the 37.30% reported by Wang et al.,19 who attributed the high incidence to the exclusion of pediatric patients receiving intraoperative antibiotics. Consistent with the findings of the present study, previous reports have suggested that indwelling double-J stents may represent a major risk factor for bacteriuria (3–10%) and may increase the risk of infection by 10–25%.23
According to Kabbani et al., the presence of an indwelling internal tube was identified as a significant risk factor for postoperative UTI in children after cardiac surgery, with an infection density rate of 18 per 1,000 urinary catheter-days.24 Similarly, Wang et al. found that infants with indwelling double-J catheters were at higher risk of UTI.7 In addition, Kitano et al. demonstrated that indwelling drainage tubes, hydronephrosis, and kidney stones were associated with an increased risk of UTI.25 Furthermore, previous studies have suggested that prolonged indwelling drainage tube duration is associated with an elevated risk of UTI in pediatric intensive care unit (PICU) patients.23, 25 This association may result from bacterial adherence to the tube wall and subsequent biofilm formation during catheterization. Strategies such as appropriate indications for tube insertion, effective management of catheter leakage, and prompt tube removal may help reduce the risk of catheter-associated UTIs.25
In the present study, low BUN levels (<3.34 mmol/L) were identified as a risk factor, which is inconsistent with the findings reported by Wang et al.19 Wang et al. suggested that BUN levels >4.3 mmol/L may also represent a risk factor, whereas the present study identified lower BUN levels (<3.4 mmol/L) as being associated with increased postoperative UTI risk. In addition, children undergoing OP were found to be at higher risk of postoperative UTI than those receiving LP. This finding is consistent with a meta-analysis of 14 studies,18 which reported that OP (6.06%) was associated with a higher complication rate than LP (4.76%), including urinary leakage and UTI. In that analysis, urinary leakage occurred in 15 LP cases and 12 OP cases, whereas UTI developed in 9 LP cases and 14 OP cases. Similarly, Wang et al. reported that OP was associated with a higher risk of postoperative UTI compared with LP.19
In this investigation, LASSO regression followed by multivariable logistic regression was used to identify predictive factors associated with the risk of UTI following unilateral UPJO surgery. The integration of these statistical methods provided a comprehensive approach to model development and variable selection, enhancing the robustness and reliability of the findings. The results highlighted the importance of variables such as sex, operative time, drainage tube type, infection history, fistula history, age, BUN level, and renal cortical thickness.
Previous studies have suggested that preoperative drug susceptibility testing and prophylactic antibiotics should be considered in children at moderate or high risk of postoperative UTI.19, 26, 27, 28 However, in the present study, the incidence of infection remained high despite the use of prophylactic antibiotics. In addition, cranberry products have been reported as a potential prophylactic strategy against UTI in otherwise healthy children.29
Most importantly, a predictive nomogram was developed and demonstrated good discriminatory performance and calibration, as reflected by the AUC values, calibration plots, and DCA results. This nomogram may provide a useful tool for clinical risk assessment and perioperative decision-making in children undergoing unilateral UPJO surgery. Overall, the analysis of these predictive factors highlights their potential contribution to postoperative UTI risk and may support future optimization of patient management strategies.
Limitations of the study
This study has several limitations. First, this was a single-center rather than a multicenter study, and its retrospective design may have introduced bias into the results. Second, external validation was lacking. Third, there is a lack of globally representative data. As the number of patients increases, additional risk factors may be identified and more effective predictive models may be developed. Therefore, further large-scale multicenter studies are needed to validate these findings.
Conclusions
Eight risk factors, including surgical modality, laterality, drainage tube type, BUN level, and height, were identified and used to develop a predictive model for postoperative UTI in children undergoing unilateral pyeloplasty. This simplified risk-scoring model may be useful in clinical practice by helping surgeons identify relevant preoperative risk factors, monitor children at high risk of postoperative UTI, and improve postoperative management of affected patients.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.17018533. The package contains the following files:
Supplementary Table 1. Generalized variance inflation factors (GVIF) and adjusted GVIF for variables, along with Box–Tidwell and Shapiro–Wilk test results.
Availability of data and materials
The datasets supporting the findings of the current study are openly available in Zenodo repository at https://doi.org/10.5281/zenodo.14862979.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.