Abstract
Background. Oncology trends are based on data coming from different countries and ocular melanoma is the most common primary eye cancer in adults.
Objectives. To investigate the incidence and characteristics of ocular melanoma in the overall population of Poland.
Materials and methods. The retrospective survey of both the National Cancer Registry (NCR) and National Health Fund (NHF) databases was performed to identify all ocular melanoma cases in Poland in 2010–2017.
Results. The mean incidence of ocular melanoma was 8.76/1,000,000 person-years; the lowest incidence was observed in the 19–29 age group (1.17/1,000,000 person-years) and the highest in the group over 70 (22.88/1,000,000 person-years). There were no statistically significant trends in the incidence rates over the study period. The overall incidences of uveal, eyelid and conjunctival melanoma were 6.67/1,000,000, 0.47/1,000,000 and 0.28/1,000,000 person-years, respectively. The 5-year overall survival (OS) was 60.76%; the higher risk of death was associated with male sex (hazard ratio (HR) = 1.2959), older age at diagnosis (HR = 1.0379), chemotherapy treatment (HR = 1.6774), metastasis (HR = 1.5716), loco-regional hyperplasia (HR = 1.5936), and systemic tumor spread (HR = 3.9872), compared to the carcinoma in situ. The risk of death was reduced by radiotherapy treatment (HR = 0.6645).
Conclusions. The incidence rate of ocular melanoma in Poland is in the middle of the range worldwide, and the 5-year OS is relatively low.
Key words: radiotherapy, patient survival, ocular melanoma
Background
Ocular melanoma is the most common primary eye cancer in adults arising from melanocytes located in the conjunctival membrane and uveal tract of the eye, which accounts for 3.7% of all melanoma cases. Among ocular melanomas, 83% arise from the uvea, 5% from the conjunctiva and 10% from other sites in the eye. Uveal melanoma is the most common primary intraocular cancer in adults.1, 2, 3, 4, 5 The incidence of ocular melanoma varies across ethnicities and regions worldwide, with the highest rates in Northern Europe and Australia and the lowest rates in Asian, Hispanic and black populations (i.e., the incidence of uveal melanoma ranges from 0.31 in Black and 0.38 in Asian populations to 11.7/1,000,000 person-years in Northern Europe). However, the incidence rate of uveal melanoma remained stable over the recent decades, while conjunctival melanoma showed an increase in the incidence rate among white men and individuals over 60.1, 4, 6, 7, 8, 9, 10 The occurrence rate of ocular melanoma is positively correlated with older age, with a peak around the age of 70. However, the mean age of the ocular melanoma diagnosis also varies in different populations, i.e., in Asia, as it affects younger individuals than in Europe or the USA, where it usually presents around the age of 60. The anterior uveal melanoma is also more common in young patients. It represents more than 20% of all uveal melanomas in the age group under 20 compared to 4% and 2% in patients aged 20–60 and over 60, respectively.1, 3, 6 Other risk factors associated with ocular melanoma include sex, Caucasian origin, light skin and iris pigmentation, genetic predisposition (BAP1 mutation), environmental factors, and certain dermatological conditions like dysplastic nevus syndrome or nevus of Ota.11, 12, 13, 14 Despite the fact that the treatment of ocular melanoma has evolved with a therapeutic shift to eye-conserving treatment options, it is estimated that still more than 50% of patients develop metastases within 25 years from the initial diagnosis. Poor prognosis indicators include older age at diagnosis, large tumor diameter, anterior location, extraocular extension, histopathological type, and cytogenetic abnormalities.3, 8, 15, 16, 17, 18, 19 Although the local data from Poland concerning conjunctival and uveal melanomas were analyzed by the RARECAREnet and the European Cancer Registry (EUROCARE) working groups,4, 7, 20 data from the entire population of Poland are lacking.
Objectives
The present study aims to analyze the incidence and characteristics of ocular melanoma in the overall population of Poland in 2010–2017, and to report the patient survival and coexisting risk factors.
Materials and methods
Data sources, disease codes
and definitions
The present study was a part of the project “Maps of Healthcare Needs – Database of Systemic and Implementation Analyses” coordinated by the Polish Ministry of Health and co-financed by the European Union funds through the European Social Fund under the Knowledge, Education and Development Operational Program (EU grant No. POWR 05.02.00-00-0149/15-01).21, 22, 23, 24 The study design was a retrospective and nationwide survey concerning patients with ocular melanoma diagnosed between January 1, 2010 and December 31, 2017. Patients were identified in the National Cancer Registry (NCR) using personal identification number (PESEL), the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), and the 3rd edition of the International Classification of Diseases for Oncology (ICD-O-3) codes. The ICD-10 codes defining ocular neoplasms are C43.1 and C69 with extensions. Ocular melanomas were found in this group of patients using ICD-O-3 codes 872–877 with extensions. Therefore, all patients with both the ICD-10 and ICD-O-3 codes (as mentioned above) were included in the study group. The analysis of the study group also included demographic data from the National Health Fund (NHF) database, such as patient sex, age at diagnosis and area code. As both the NCR and the NHF databases cover the entire population of Poland, we believe that all ocular melanoma cases diagnosed in Poland between 2010 and 2017 were included in the statistical analysis. In addition, population data for Poland and patient death records were obtained from Statistics Poland.25, 26, 27
Data analyses
In the 1st part of the study, the descriptive statistics and demographic characteristics of the study group and the incidence analysis of ocular melanoma were performed for each year of the study period, separately. Then, the analysis of patients diagnosed with ocular melanoma in 2010–2014 with 5 years of follow-up was carried out, allowing the performance of survival analysis. The 1-year and 5-year overall survival (OS) rates were calculated. The Cox proportional hazards model was applied, and hazard ratios (HRs) with a 95% confidence interval (95% CI) were computed. A value of p < 0.05 was considered statistically significant. The Kaplan–Meier curve was employed to present the 5-year survival. Many different factors were considered in the survival analysis, including patient sex, age at the time of diagnosis, place of residence, and treatment method. Data on the general treatment schedule were available in the NCR database; these data concern surgical treatment, radiotherapy, chemotherapy, and other therapies. Additionally, detailed therapies were identified using the ICD-9 codes according to the ICD-9-CM Volume 3 classification (a subset of the International Statistical Classification of Diseases and Related Health Problems (ICD)-9-CM) and obtained from the NHF database of medical services. They were matched with the study group from NCR. The ICD-9 codes, namely 16.31, 16.39, 16.41, 16.42, 16.49, 16.51, and 16.52, were used to identify surgical treatment by enucleation, and ICD-9 codes 14.26, 14.27 and 92.4 with extensions were applied to identify radiotherapy by plaque brachytherapy. Other therapies indicated in the NCR database included laser therapy and targeted therapy. Other clinical factors obtained from the NCR database were also taken into account, including metastases or advancement stages. Tumor growth advancement was divided into 4 categories: in situ, local, loco-regional, and systemic. The reference group was the tumor in situ. The R statistical software v. 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for all analyses. The demographic characteristics of patients are presented with the mean and standard deviation (SD).
Since our study did not require ethics committee approval, it adhered to the tenets of the Declaration of Helsinki for research involving human subjects (socio-demographic data, including age, sex and place of residence, were recorded anonymously). Furthermore, the study protocol was approved by the Polish Ministry of Health, which is entitled by the laws of the Republic of Poland to process the NHF data. The informed consent was waived.
Results
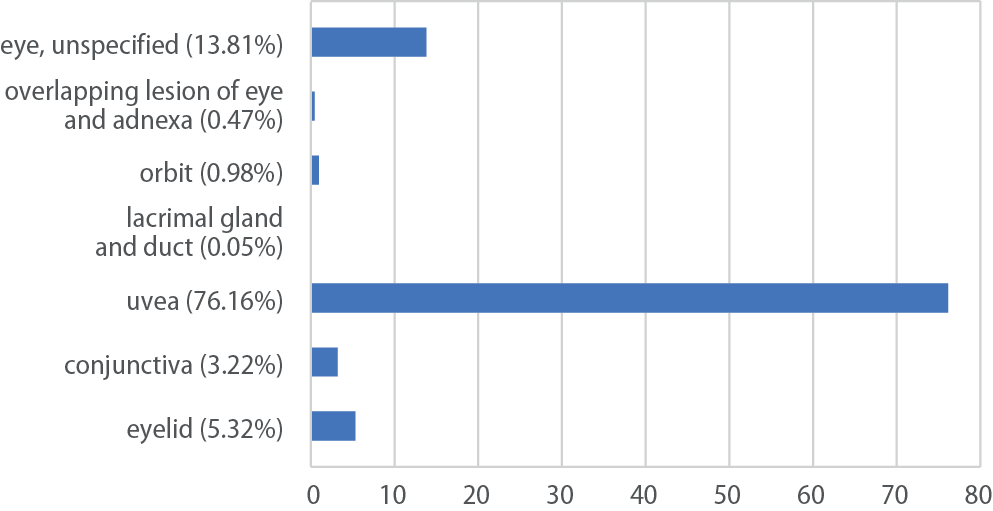
In total, 2143 patients with ocular melanoma were identified in Poland between January 1, 2010 and December 31, 2017. The incidence rates for each age group in the study period are presented in Table 1 and Figure 1. The mean incidence of ocular melanoma was 8.76/1,000,000 person-years (95% CI: [6.94; 10.58]). The incidence of ocular melanoma increased with age: the lowest incidence was observed in patients aged 19–29 (1.17/1,000,000 person-years) and the highest in patients over 70 (22.88/1,000,000 person-years). The number of ocular melanoma diagnoses by anatomical localization is presented in Figure 2. The uveal melanoma (iris, ciliary body and choroid localizations) was the most common and was diagnosed in 1632 (76.16%) patients. Eyelid melanoma was the 2nd most common and was diagnosed in 114 (5.32%) patients. The 3rd most common was conjunctival melanoma, which was diagnosed in 69 (3.22%) patients. The other melanomas were localized in orbit (21 patients (0.98%)), overlapping lesion of eye and adnexa (10 patients (0.47%)) and lacrimal gland and duct (1 patient (0.05%)). At the same time, unspecified ocular melanoma was diagnosed in 296 (13.81%) patients. The overall incidences of uveal, eyelid and conjunctival melanoma were 6.67/1,000,000, 0.47/1,000,000 and 0.28/1,000,000 person-years, respectively.
The demographic characteristics of patients with ocular melanoma in Poland are presented in Figure 1 and Table 1, Table 2. The mean age at the time of diagnosis was 62.73 ±14.43 years, and there was a slight increase in the mean age of diagnosis over the study period. The majority of patients were female (53.57%), and the proportion of women in each analyzed year was more than half. In addition, the vast majority of patients (65%) were urban residents. The overall ocular melanoma incidence rate was also higher in women (8.96/1,000,000 person-years) than in men (8.54/1,000,000 person-years).
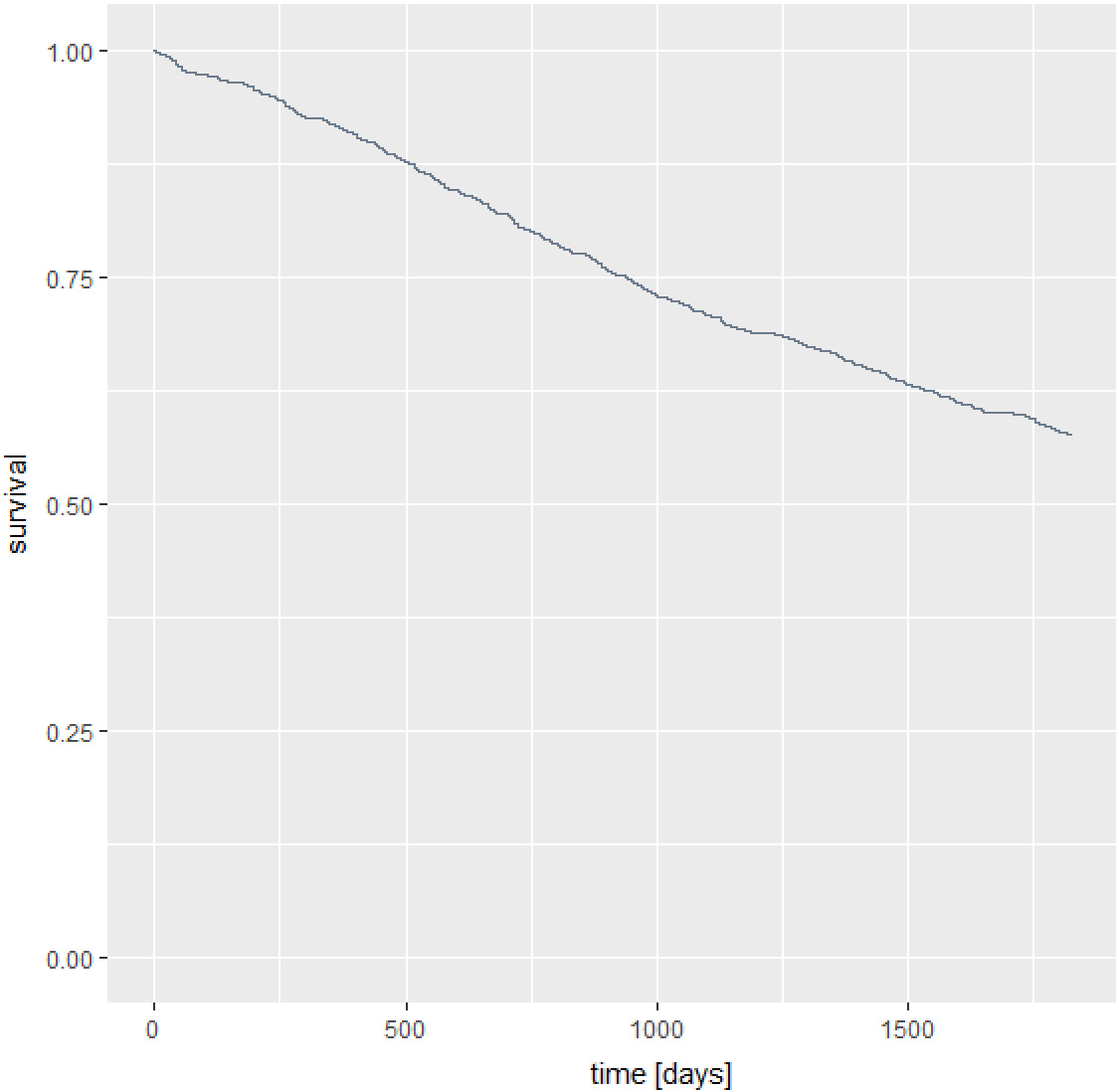
The OS analysis included 1192 patients diagnosed in 2010–2014. One hundred patients (8.39%) died within 1 year and 507 patients (39.24%) died within 5 years from ocular melanoma diagnosis. The 1-year and 5-year OS rates were 91.61% and 60.76%, respectively. Among statistically significant variables, a higher risk of death within 5 years was associated with male sex (HR = 1.2959; 95% CI: [1.086; 1.547]), older age at diagnosis (HR = 1.0379; 95% CI: [1.03; 1.046]), chemotherapy treatment (HR = 1.6774; 95% CI: [1.317; 2.136]), metastasis (HR = 1.5716; 95% CI: [1.056; 2.340]), loco-regional hyperplasia (HR = 1.5936; 95% CI: [1.111; 2.286]), and systemic tumor spread (HR = 3.9872; 95% CI: [3.021; 5.263]) compared to the carcinoma in situ. The risk of death was statistically reduced by radiotherapy treatment (HR = 0.6645; 95% CI: [0.529; 0.835]). However, place of residence, surgery treatment and local tumor growth (compared to the tumor in situ) were not associated with the mortality rate. All results of survival analysis are presented in Table 3. The Kaplan–Meier curve shows the patient survival (Figure 3). The results of the test for the proportional hazards assumption are presented in Table 4.
Discussion
This study evaluates for the first time the incidence and characteristics of ocular melanoma in the overall population of Poland. The analysis included both the age-standardized incidence of ocular melanoma (the unit of incidence is captured by 1,000,000 person-years) in 2010–2017 and the survival analysis of patients diagnosed with ocular melanoma in 2010–2014, with 5 years of follow-up. The mean incidence of ocular melanoma was 8.76/1,000,000 person-years, and the mean age at the time of diagnosis was 62.73 ±14.43 years. The overall incidences of uveal, eyelid and conjunctival melanoma were 6.67/1,000,000, 0.47/1,000,000 and 0.28/1,000,000 person-years, respectively. Our results were in the middle of the range of ocular melanoma incidence worldwide, which is much higher among Whites than Blacks and Asians.1, 2, 3 Our age-standardized incidence of uveal melanoma was similar to that reported earlier in Poland by the EUROCARE working group for the 1983–1994 period.7 It was also similar to that reported in Central Europe (Slovakia, Slovenia and Switzerland), higher than that reported in South Korea, Singapore, USA, and Southern Europe (Italy and Spain) but lower than in Northern Europe (Denmark, Norway, Sweden, and Estonia), Ireland and Australia.6, 7, 9, 11, 15 However, we cannot exclude the misclassification bias. The number of uveal melanoma cases might have been underestimated, while unspecified ocular melanoma might have been overestimated. Errors in using specific ICD-10 codes might have occurred at different levels (hospitals, outpatient clinics, and NCR and NHF offices). However, we believe that such errors had only minor impact on the study findings. Our age-standardized incidence of conjunctival melanoma was similar to that reported earlier in Eastern Europe by the EUROCAREnet working group for the 1995– 2007 period and higher than that reported among Blacks in the USA and whole population in Southern Europe but lower than among Whites in the USA and the whole population in Northern Europe.4 The north-to-south decreasing gradient in the uveal melanoma incidence in Europe might be related to the protective effect of ocular pigmentation in the southern populations with respect to higher exposure to ultraviolet light at lower latitudes. Moreover, Eastern European countries like Poland have the lowest rates of both conjunctival and skin melanomas in Europe.4, 7 Most of the previous studies showed an increased age-adjusted incidence rate of ocular melanoma among men,6, 9, 11, 12, 14, 15, 17 but in other large cohort clinical studies with no age adjustment, no sex-based differences were reported.3 In contrast to those studies, the incidence rate of ocular melanoma in Poland was higher in women, which might be attributable to the excess male death rate, characteristic to the Eastern European countries, which is visible in Poland.27, 28, 29
Since the Collaborative Ocular Melanoma Study (COMS) showed no survival advantage of enucleation over brachytherapy for medium-size tumors, the therapeutic shift to eye-conserving treatment options was observed worldwide.17, 19 However, medical management of ocular melanoma depends on the tumor location, size, local extension, visual acuity at presentation, and systemic status. Most patients with posterior tumors are currently treated with plaque brachytherapy. Other available options include laser photocoagulation, transpupillary thermotherapy, particle beam radiotherapy, gamma knife radiosurgery, local surgical resection, and/or enucleation (with or without orbital exenteration). The current standard for anterior tumors management is a surgical treatment with adjuvant therapy, including brachytherapy. Other management methods for both anterior and posterior tumors include targeted therapy and/or chemotherapy (in case of metastases). Although more than 90% of primary tumors are managed with surgery or eye-conserving therapies, more than 50% of patients develop metastases, usually involving the liver.1, 3, 16, 30
The OS analysis revealed that 100 patients (8.39%) died within 1 year and 507 patients (39.24%) died within 5 years from the initial diagnosis of ocular melanoma in Poland, which gives the 1-year and 5-year mortality rates of 8.39% and 39.24%, respectively. The 1-year OS was 91.61%, and the 5-year OS was 60.76%, which is comparable to the data from an epidemiological study of uveal melanoma from US Surveillance, Epidemiology and End Results Program for 2010–2015, where the 5-year OS was 61.8%. However, our mortality rate was higher than that found in the UK, Denmark, Sweden, Singapore, or Israel.2, 10, 14, 20, 31, 32 The Cox proportional hazards model showed that the higher risk of death within 5 years from the initial ocular melanoma diagnosis in Poland was associated with male sex, older age at diagnosis, chemotherapy treatment, metastasis, loco-regional hyperplasia, and systemic tumor spread compared to the carcinoma in situ. The risk of death was statistically reduced by radiotherapy treatment. However, chemotherapy treatment increased the risk of death in our model. It should be assumed that the treatment method depends on the carcinoma stage and chemotherapy is used in more severe stage of tumor. Our results were consistent with previously published studies that showed older age at diagnosis, severe stage of the tumor, distant metastasis, and no radiation to be associated with the mortality risk. Those studies also revealed that beyond 15 years from diagnosis, a patient with uveal melanoma is more likely to die from other causes than uveal melanoma metastasis itself.14, 31, 32
Limitations
The limitations of the present study include selection bias as there is an increasing proportion of cases without histopathological proof of diagnosis. In addition, both NHF and NCR databases do not cover the family history and genetic information of ocular melanoma patients in Poland, with disease laterality also not available for all included subjects. Therefore, we might have missed some data and the investigation of potential risk factors of mortality was not complex. However, this likely had only a minor impact on our findings. The most important strengths of the present study are the population size, nationwide recruitment, and the usefulness of its results for clinicians and healthcare providers in Poland.
Conclusions
This study found that the incidence rate of ocular melanoma in Poland is in the middle range of worldwide incidence, and the 5-year OS is relatively low. Furthermore, a higher risk of mortality from ocular melanoma in Poland is associated with male sex, older age at diagnosis, chemotherapy treatment, metastasis, loco-regional hyperplasia, and systemic tumor spread compared to carcinoma in situ.