Abstract
Metabolic dysfunction-associated steatohepatitis (MASH) represents a progressive form of metabolic dysfunction-associated steatotic liver disease (MASLD) and contributes significantly to morbidity and mortality in developed countries. Current clinical practice primarily relies on dietary and lifestyle modifications, while specialized obesity management is used less frequently. However, the long-term efficacy of these approaches remains unsatisfactory. Among pharmacological options, gliflozins have emerged as a promising class of agents with potential benefits in reducing histological activity and improving the prognosis of MASLD/MASH. The beneficial effects of gliflozins in diabetes, cardiology, and nephrology have already been demonstrated, and their use is becoming increasingly common across various clinical indications. However, their role in the treatment of MASLD/MASH has not yet been fully clarified. Preliminary studies suggest that gliflozins may positively influence disease progression in these conditions. This article provides a comprehensive overview of MASLD/MASH and reviews current evidence regarding the therapeutic effects of gliflozins on these liver diseases.
Key words: non-alcoholic fatty liver disease (NAFLD), metabolic dysfunction-associated steatohepatitis (MASH), metabolic dysfunction-associated steatotic liver disease (MASLD), sodium-glucose transporter 2 inhibitors (SGLT2 inhibitors), type 2 diabetes mellitus (T2DM)
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) is currently the most common liver disease worldwide. Available estimates suggest that up to 1/3 of the global population may be affected by this condition. Metabolic dysfunction-associated steatotic liver disease is considered the hepatic component of metabolic syndrome and contributes significantly to morbidity and mortality in developed countries.1 The diagnostic criteria include hepatic steatosis detected through imaging and/or histology, together with the presence of at least 1 of 5 cardiometabolic risk factors (Table 1).2 The change in nomenclature and introduction of the term MASLD are intended to place greater emphasis on metabolic dysregulation, such as type 2 diabetes mellitus (T2DM) or obesity, compared with the former term non-alcoholic fatty liver disease (NAFLD). At the same time, the new nomenclature acknowledges the synergistic effect of alcohol consumption. This change in terminology reflects key findings regarding hepatic and extrahepatic mortality risk, disease associations, and the identification of high-risk individuals.3
Recent studies suggest that excess body weight and metabolic dysfunction independently affect the development of MASLD and cardiometabolic outcomes. In clinical practice, MASLD is commonly associated with overweight/obesity and T2DM, with more than 70% of patients with T2DM having some form of MASLD. However, studies suggest that even patients with metabolically healthy obesity, defined as the absence of metabolic disorders and/or cardiovascular disease (CVD), remain at high risk of developing significant hepatic fibrosis. Lean individuals are also not protected against MASLD development, and no difference in histological severity has been observed between patients with a body mass index (BMI) <23 kg/m2 and those with a BMI > 25 kg/m2. These findings indicate that both metabolic health and metabolic dysfunction, which may vary throughout a patient’s life, are important factors to consider.3, 4 Metabolic dysfunction-associated steatotic liver disease is further subdivided into metabolic dysfunction-associated steatosis (MASL) and metabolic dysfunction-associated steatohepatitis (MASH). These subgroups differ substantially in clinical course and prognosis. While MASL is more commonly observed as a concomitant condition in patients with metabolic syndrome, MASH represents a progressive form that may eventually lead to hepatocyte apoptosis, fibrosis, loss of functional liver tissue, and ultimately liver cirrhosis with its associated complications.1
In current clinical practice, the Fibrosis-4 (FIB-4) score (age, aspartate transaminase (AST), alanine transaminase / lanine aminotransferase (ALT), and platelet count) is used to screen at-risk patients for liver fibrosis.5
If the FIB-4 value is between 1.3 and 2.6, noninvasive liver stiffness measurement (LSM) is recommended.5, 6 If the score exceeds 2.6, direct referral to a hepatogastroenterology specialist is indicated. The diagnosis of MASH is based on histological examination of liver tissue.6, 7
Objectives
With the rising use of SGLT2i, their effects on MASLD/MASH should be established. This short review provides an overview of the topic and attempts to link original studies and recommendations from professional societies with recent studies and meta-analyses, without using a specific sampling protocol. The aim of this article is to provide a brief introduction to the issue, promote further research in this area, and indicate where it is most needed.
Pathogenesis of MASH
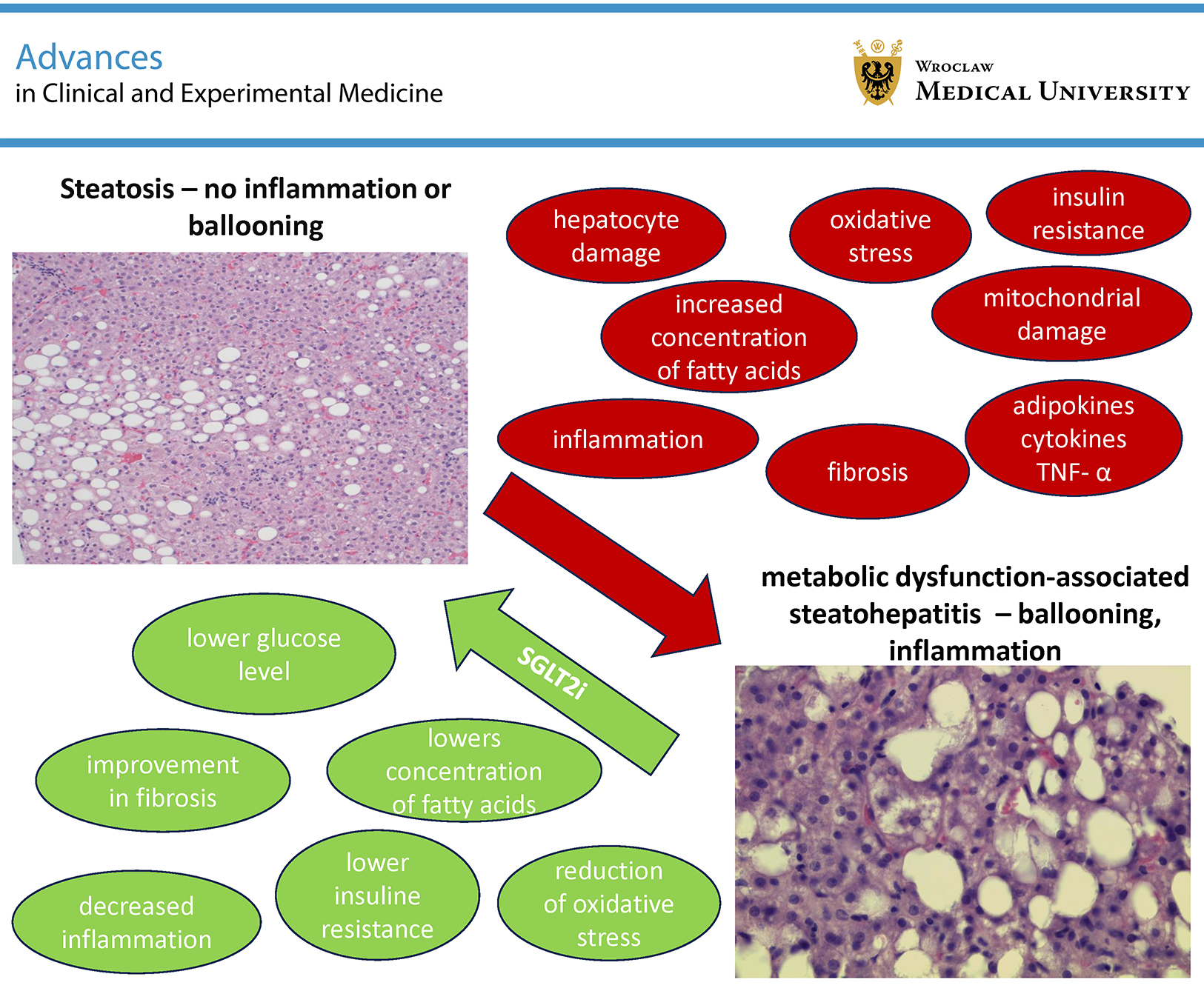
The exact pathogenesis of MASH and the mechanisms underlying its progression have not yet been fully elucidated, and a multifactorial etiology is assumed. Increased concentrations of fatty acids accumulated in hepatic adipose tissue lead to oxidative stress, mitochondrial damage, hepatocyte injury, and, consequently, the development of insulin resistance. Furthermore, insulin resistance contributes to macrophage activation and the development of inflammation. The roles of genetics, epigenetics, and the gut microbiome remain incompletely understood. Diagnosis is additionally complicated by the difficulty in accurately assessing the quantity and frequency of alcohol consumption.
There is growing evidence that a high-fat diet, insulin resistance, obesity, dysregulation of peripheral lipolysis, and other metabolic risk factors contribute to increased hepatic deposition of free fatty acids. Progressive accumulation of triacylglycerols within hepatocyte cytoplasm leads to steatosis that is not attributable to excessive alcohol consumption or drug-induced liver injury. Repeated liver injury, endoplasmic reticulum oxidative stress, reactive oxygen species (ROS), and mitochondrial dysfunction subsequently promote inflammation. Insulin resistance further contributes to de novo lipogenesis and adipose tissue dysfunction, resulting in the release of inflammatory adipokines and cytokines, including tumor necrosis factor alpha (TNF-α).8
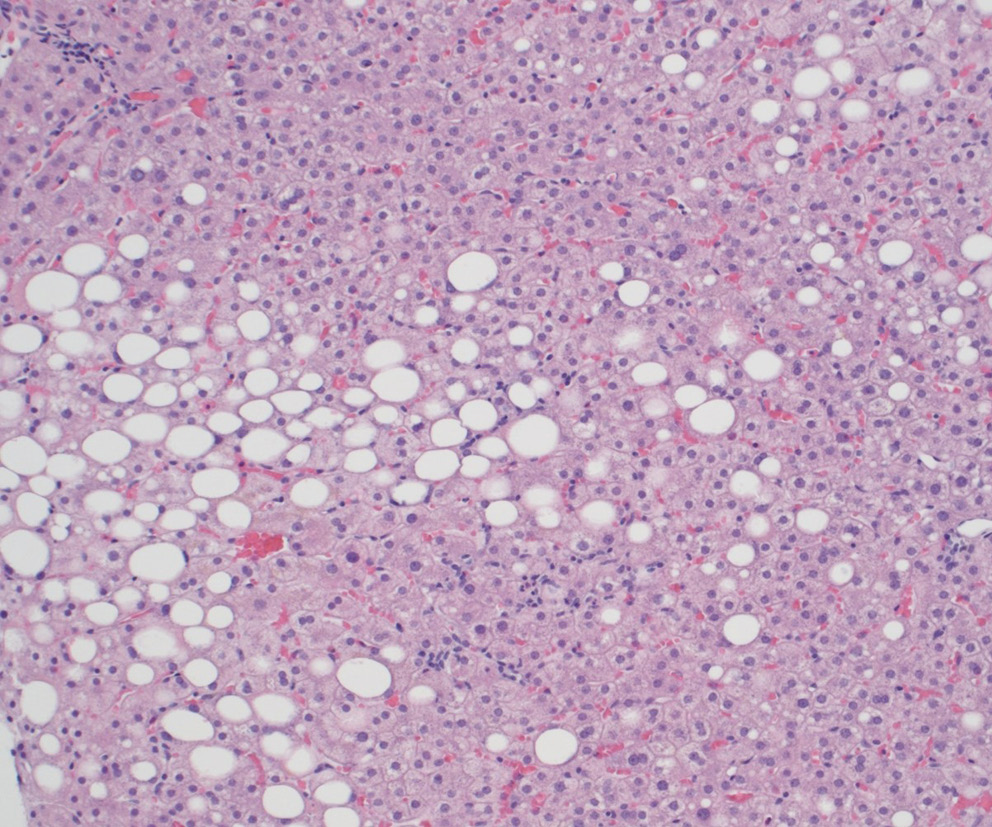
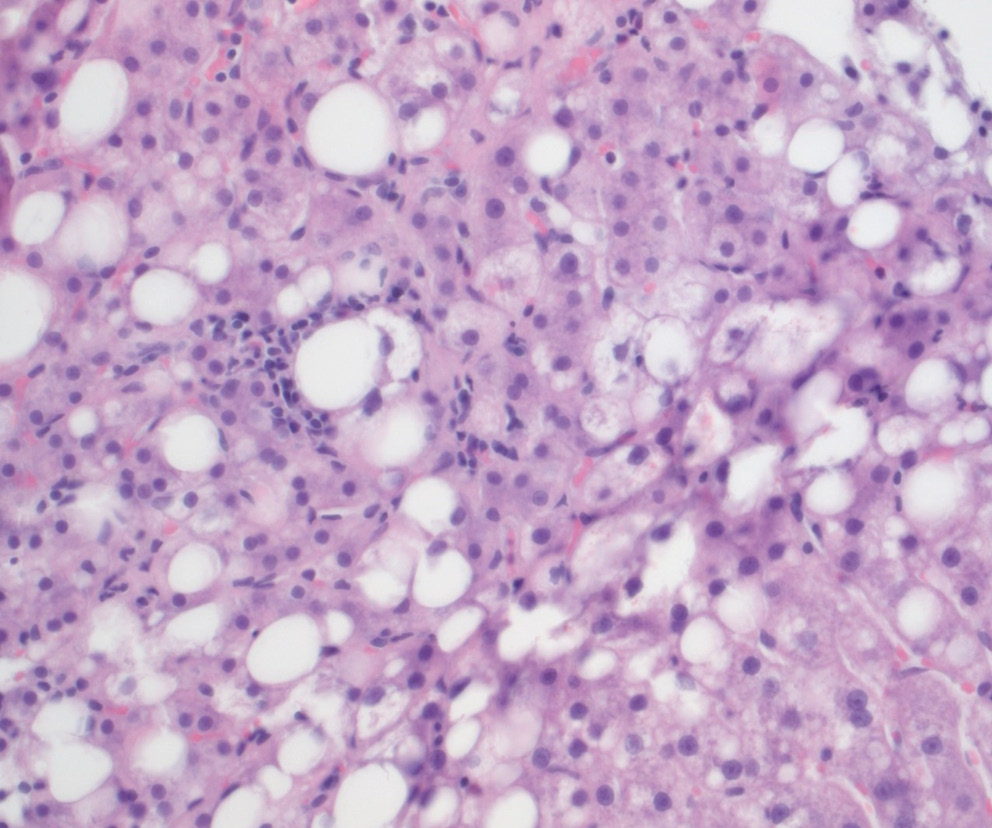
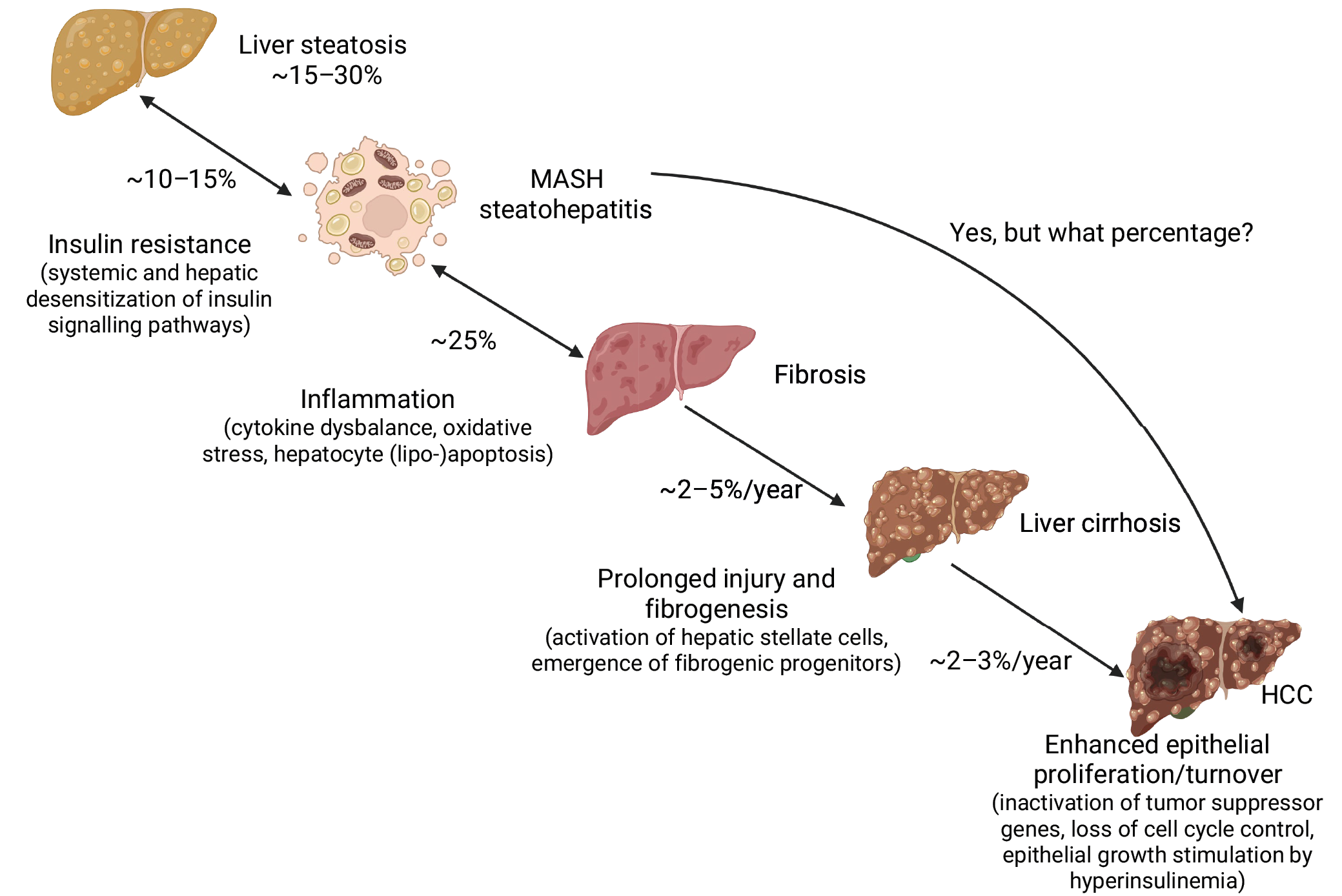
The development of hepatic inflammation distinguishes MASLD from MASH, as illustrated in Figure 1, which demonstrates simple steatosis on hematoxylin and eosin (H&E) staining, in contrast to MASH shown in Figure 2. These and other factors disrupt hepatic homeostasis and activate immune responses, leading to hepatocyte apoptosis and liver fibrosis.9 Liver cirrhosis is frequently complicated by the development of hepatocellular carcinoma (HCC; Figure 3).10 Hepatocellular carcinoma is the 6th most commonly diagnosed cancer and the 3rd leading cause of cancer-related death worldwide, with a higher incidence in men. It accounts for 75–85% of primary liver cancers. MASH is considered one of the major risk factors for HCC, alongside hepatitis B virus infection, hepatitis C virus infection, and excessive alcohol consumption (>30 g/day in men and >20 g/day in women).11
The progression of MASLD was evaluated in a study including 718 patients who underwent more than 2 non-targeted liver biopsies performed at least 6 months apart. At the initial biopsy, 497 patients (69.2%) had MASLD, 90 (12.5%) had non-fibrotic MASH, and 131 (18.2%) had non-cirrhotic fibrosis. Over a median follow-up period of 3.4 years between biopsies, 30.4% (218/718) of patients experienced disease progression, including 12.5% (62/497) with incident non-fibrotic MASH, 24.0% (141/587) with incident fibrosis, and 5.6% (40/718) with cirrhosis.12
Epidemiology and current therapy of MASLD
The worldwide prevalence of MASLD is reported to be approx. 30%, while the global prevalence of MASH is estimated at 5.27%.1 According to the Global Burden of Disease study, MASLD is the disease with the fastest-growing proportion among chronic liver diseases, including liver cirrhosis and HCC.13 Globally, approx. 20% of NAFLD cases were classified as NASH in 2015, and by 2030, this proportion is projected to increase to 27% according to the Makarov model, reflecting both disease progression and population aging. The incidence of decompensated cirrhosis is projected to increase by 168% to 105,430 cases by 2030, while the incidence of HCC is projected to increase by 137% to 12,240 cases. Deaths from liver disease are projected to increase by 178% to an estimated 78,300 deaths by 2030.14 Given the increasing morbidity and mortality associated with progressive forms of MASLD, there is growing urgency to identify effective therapies. In March 2024, the U.S. Food and Drug Administration (FDA) approved resmetirom for the treatment of MASH/MASLD, but this drug has not yet been approved in the EU. In routine practice, treatment still relies on management of individual components of metabolic syndrome, including the use of bariatric surgery techniques. However, the long-term effectiveness of these procedures remains unsatisfactory.
SGLT2 inhibitors (gliflozins)
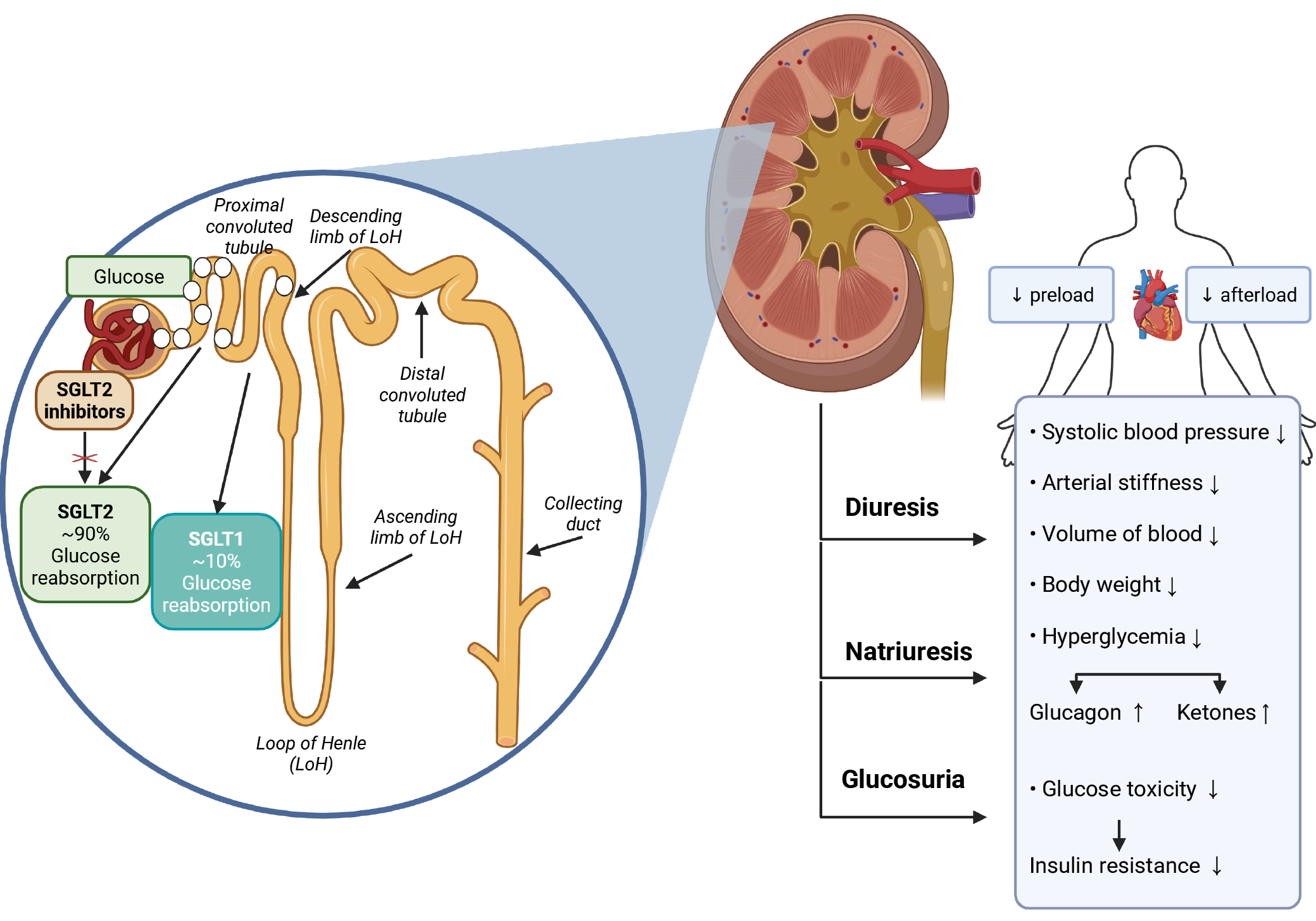
SGLT2 inhibitors (sodium-glucose co-transporter 2 inhibitors (SGLT2i)) are a modern group of drugs originally used as oral antidiabetic agents, either as monotherapy for T2DM or in combination with insulin or other oral antidiabetic agents in the treatment of this disease. Gliflozins block sodium-glucose co-transporter 2 (SGLT2) in the kidney. During blood filtration in the kidney, SGLT2 is responsible for the reabsorption of glucose from urine into the bloodstream. Thus, when SGLT2 activity is blocked, urinary glucose excretion increases and blood glucose concentration decreases. The mechanism of action of gliflozins is independent of insulin.15
SGLT2, which is mainly found in the proximal tubule, is responsible for up to 97% of renal glucose reabsorption and approx. 5% of total renal sodium reabsorption. The direct and indirect effects on sodium transport play an important role in cardioprotection and renoprotection; therefore, in addition to diabetes, gliflozins have also found applications in cardiology and nephrology, as shown in Figure 4.15, 16
According to the first large completed clinical trial, the EMPA-REG OUTCOME trial published in 2015, compared with placebo, the use of SGLT2i resulted in a significantly lower risk of cardiovascular death, reduced all-cause mortality, and fewer hospitalizations for heart failure.15 In large cardiovascular trials, beneficial effects on renal function were also observed, which led to studies focusing primarily on renoprotection. The first breakthrough study was the CREDENCE trial, which investigated the effect of canagliflozin on glomerular filtration rate in patients with T2DM. In this study, canagliflozin reduced the risk of renal and cardiovascular events independently of baseline glomerular filtration rate.17
The beneficial effects of SGLT2i are likely multifactorial and include alterations in arterial stiffness, cardiac function, and cardiac oxygen consumption. In addition to cardiorenal effects, SGLT2i reduce albuminuria and hyperuricemia and favorably affect hyperglycemia, body weight, visceral adiposity, and blood pressure.15 Other effects of SGLT2i include reduction of oxidative stress and reactive oxygen species (ROS) generated by TNF-α through inhibition of sodium-hydrogen exchange and reduction of intracellular sodium levels.18
SGLT2 inhibitors in the treatment of MASLD/MASH
Even in the case of MASLD, a growing number of studies have evaluated the effects of SGLT2i treatment on liver disease. A multicenter retrospective study by Huynh et al. compared 5-year mortality, the composite risk of hepatic decompensation, and the incidence of HCC in patients with diabetes and liver cirrhosis treated with either metformin monotherapy or dual therapy consisting of metformin and SGLT2i. Dual therapy was associated with reduced mortality compared with monotherapy (p = 0.002).8, 19, 20
In a recent meta-analysis evaluating the effects of SGLT2i on liver fibrosis and MASLD, 18 studies published up to December 2023 involving a total of 1,330 patients were included after meeting the eligibility criteria. The meta-analysis concluded that SGLT2i use may lead to modest improvement in hepatic steatosis and/or fibrosis compared with controls in patients with MASLD and T2DM, based on imaging and histopathological biomarkers, with low to moderate certainty of evidence, as shown in Table 2, Table 3.19, 21, 22, 23, 24, 25, 26
Case-control studies suggest that the use of glucagon-like peptide-1 receptor agonists (GLP-1 receptor agonists) or SGLT2i in patients with T2DM may be associated with a reduced risk of hepatic complications, although the only available pilot study of semaglutide in patients with cirrhosis did not demonstrate histological improvement. In the study by Newsome et al., 320 patients (230 of whom had stage F2 or F3 fibrosis) were randomly assigned to receive semaglutide at doses ranging from 0.1 mg to 0.4 mg or placebo. The highest percentage of patients achieving MASH resolution was observed in the 0.4-mg group (59%) compared with the placebo group (17%) (p < 0.001 for semaglutide 0.4 mg vs placebo). Improvement in fibrosis stage occurred in 43% of patients in the 0.4-mg group and in 33% of patients in the placebo group (p = 0.48). Although this trial demonstrated a significantly higher rate of MASH resolution with semaglutide compared with placebo, it did not show a significant improvement in fibrosis stage in patients with MASH.27, 28
There is currently an ongoing multicenter, randomized, double-blind, placebo-controlled phase 3 trial involving patients with MASH and moderate or advanced liver fibrosis who once weekly receive semaglutide at a dose of 2.4 mg or placebo. Interim trial results have demonstrated statistically significant improvement in liver histological findings. However, further research and additional data are required to confirm these results.29
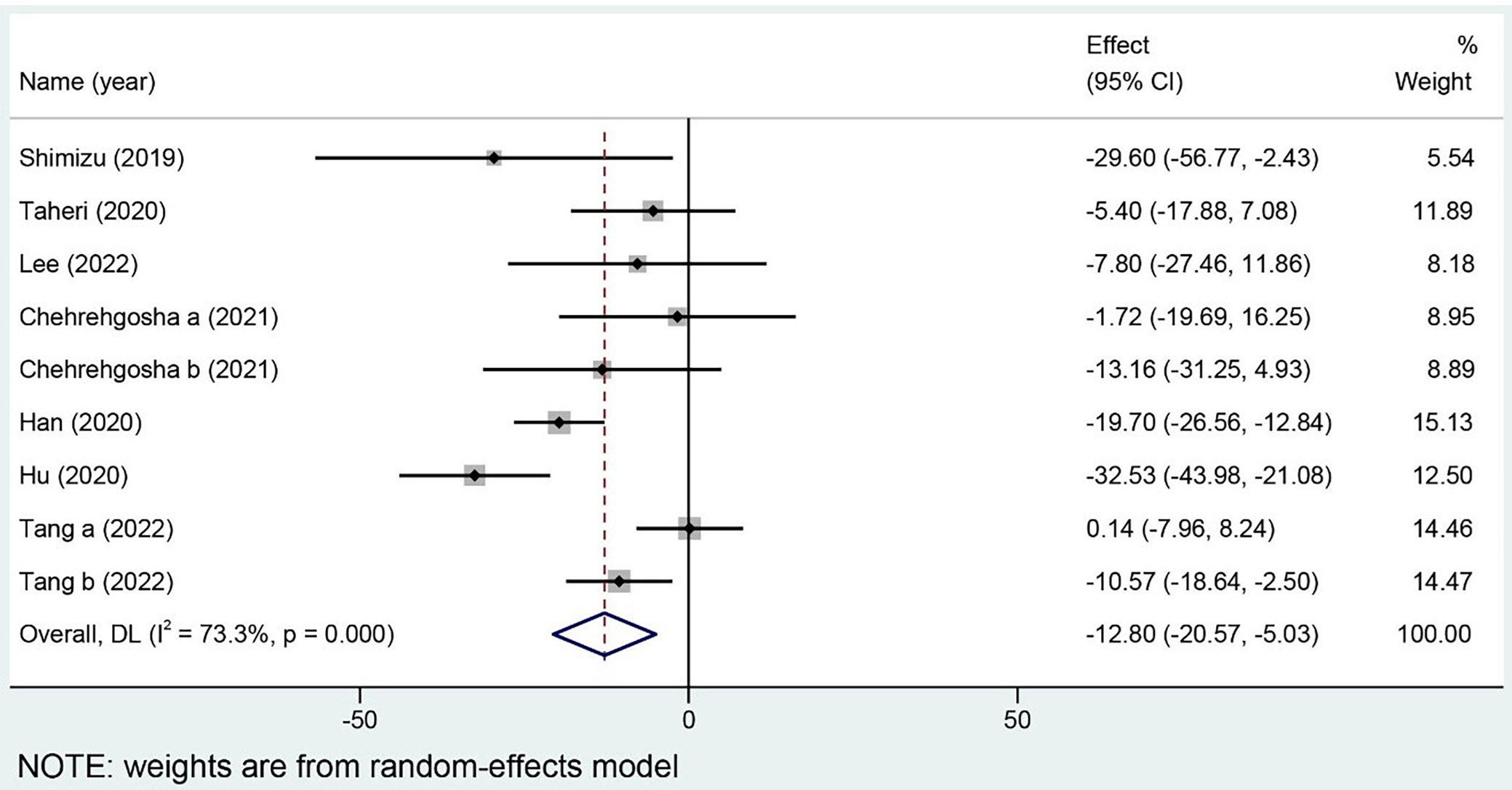
In a meta-analysis by Zhou et al., a total of 686 patients from 8 studies were included. Compared with the control group, SGLT2i significantly reduced controlled attenuation parameter (CAP) values (mean difference (MD) = −12.80, 95% confidence interval (95% CI): [−20.57, −5.03], p = 0.001; Figure 5) and liver stiffness measurement (LSM) values (MD = −0.82, 95% CI: [−1.38, −0.25], p = 0.005).30
According to the 2024 European guidelines for MASLD, there is currently insufficient evidence to recommend SGLT2i or metformin as specific treatments for MASH. However, their use in patients with MASLD is considered safe within currently approved indications. The guidelines indicate that SGLT2i are safe in patients with Child–Pugh class A and B cirrhosis and may be used according to their approved indications.21 Sufficient evidence supporting the effects of SGLT2i on reducing inflammatory activity and fibrosis in patients with histologically confirmed MASH is still lacking.
Limitations of the study
The main limitation of this review is that it falls within the category of narrative or scoping reviews and provides only a brief overview of the topic. It is not a protocol-driven, in-depth data analysis and may therefore be subject to limitations such as bias.
Conclusions
The importance of SGLT2i in diabetes, cardiology, and nephrology has already been demonstrated, and their use is becoming increasingly common across various clinical indications; however, their role in the treatment of MASLD/MASH has not yet been fully clarified. Nevertheless, SGLT2i are likely to be encountered in patients with MASLD/MASH during treatment of associated diseases related to metabolic syndrome and its complications. Some evidence suggests that SGLT2i may have beneficial effects on the course of MASLD/MASH, including potential effects on fibrosis, steatosis, and oxidative stress, at least through indirect mechanisms. However, sufficient evidence evaluating the effects of SGLT2i on reducing histologically confirmed inflammatory activity and liver fibrosis in MASH is still lacking. Further research focusing on histological assessment of the effects of SGLT2i is needed.
Use of AI and AI-assisted technologies
Not applicable.