Abstract
This review systematically analyzes the relationship between the immune microenvironment characteristics of microsatellite instability-high (MSI-H) or deficient mismatch repair (dMMR) colorectal cancer (CRC) and the efficacy of immune checkpoint inhibitors (ICIs). The article emphasizes that this tumor subtype has a high mutation burden, abundant neoantigens, and significant immune cell infiltration, explaining its high sensitivity to immunotherapy, while also pointing out that some patients exhibit primary non-response or subsequent resistance. Based on single-cell and spatial omics, as well as multi-omics integration analyses, the authors reveal the complexity and heterogeneity of key immune cell subpopulations, spatial distribution, and resistance mechanisms (such as abnormal Janus kinase/signal transducer and activator of transcription (JAK/STAT) pathways, human leukocyte antigen (HLA) loss, and metabolic reprogramming, and propose the necessity of multi-time-point dynamic monitoring and multimodal combination therapy. The study underscores that, in the future, standardized data integration and the establishment of artificial intelligence (AI) prediction models will be required to facilitate the implementation of precise, individualized immunotherapy strategies, thereby further improving clinical efficacy.
Key words: immune checkpoint inhibitors, tumor immune microenvironment, MSI-H/dMMR, single-cell and spatial transcriptomics
Introduction
Colorectal cancer (CRC) is one of the most common malignant tumors worldwide and a leading cause of cancer-related death. In 2020, it was estimated that there were approx. 1.9 million new CRC cases and 930,000 deaths globally.1 With population aging and the increasing prevalence of unhealthy lifestyles, the incidence of CRC in low- and middle-income countries has been rising rapidly. Although screening and treatment have made significant progress, the prognosis for advanced CRC remains poor; the 5-year survival rate for stage IV disease is only about 14%. Particularly in metastatic CRC, conventional treatments (surgery, chemotherapy, and biologically targeted therapies) often fail to achieve durable responses, highlighting the urgent need for new therapeutic strategies.2
Microsatellite instability-high (MSI-H) or deficient mismatch repair (dMMR) CRC accounts for about 15% of all CRC cases. Due to defects in the DNA mismatch repair pathway, these tumors accumulate a large number of mutations, thereby generating abundant neoantigens and resulting in a high tumor mutation burden (TMB).3 MSI-H/dMMR CRC is usually characterized by rich immune cell infiltration (a “hot” tumor) and displays strong immunogenicity. In contrast, microsatellite-stable (MSS) or mismatch repair-proficient (pMMR) CRC exhibits relatively low immune infiltration and is considered an immune-tolerant “cold” tumor.4 This difference in the immune microenvironment partly explains the marked sensitivity of MSI-H/dMMR CRC to immune checkpoint inhibitors (ICIs).
Since 2017, ICIs have been approved for the treatment of MSI-H/dMMR metastatic CRC. Phase III clinical trials, such as KEYNOTE-177, have shown that PD-1 inhibitors (e.g., pembrolizumab) can significantly prolong progression-free survival (PFS) in patients with MSI-H mCRC compared with chemotherapy.5 However, approx. 40–60% of MSI-H/dMMR CRC patients still exhibit primary non-response or subsequently develop acquired resistance to ICIs. In some cases, immune therapy-related hyperprogression (HPD), characterized by unexpectedly accelerated tumor growth, has been observed.6 Therefore, an in-depth analysis of the unique immune microenvironment characteristics of MSI-H/dMMR CRC and their relationship to therapeutic efficacy is of great significance for improving immunotherapy outcomes.
Objectives
This review aims to systematically summarize research progress on the tumor immune microenvironment (TME) of MSI-H/dMMR CRC since 2018, focusing on: 1) the roles of various TME components (such as TMB, neoantigens, immune cells, fibroblasts, and stroma); 2) the heterogeneity of key immune cell subpopulations and their responses to treatment; 3) potential mechanisms of immunotherapy resistance and HPD; 4) the application of new technologies, such as single-cell sequencing and spatial transcriptomics; 5) novel biomarkers identified through multi-omics integration; and 6) current challenges and future trends. By reviewing these cutting-edge advances, we aim to provide a reference for developing individualized immunotherapy strategies and to emphasize the importance of large-scale multi-omics research and multidisciplinary collaboration.
Materials and methods
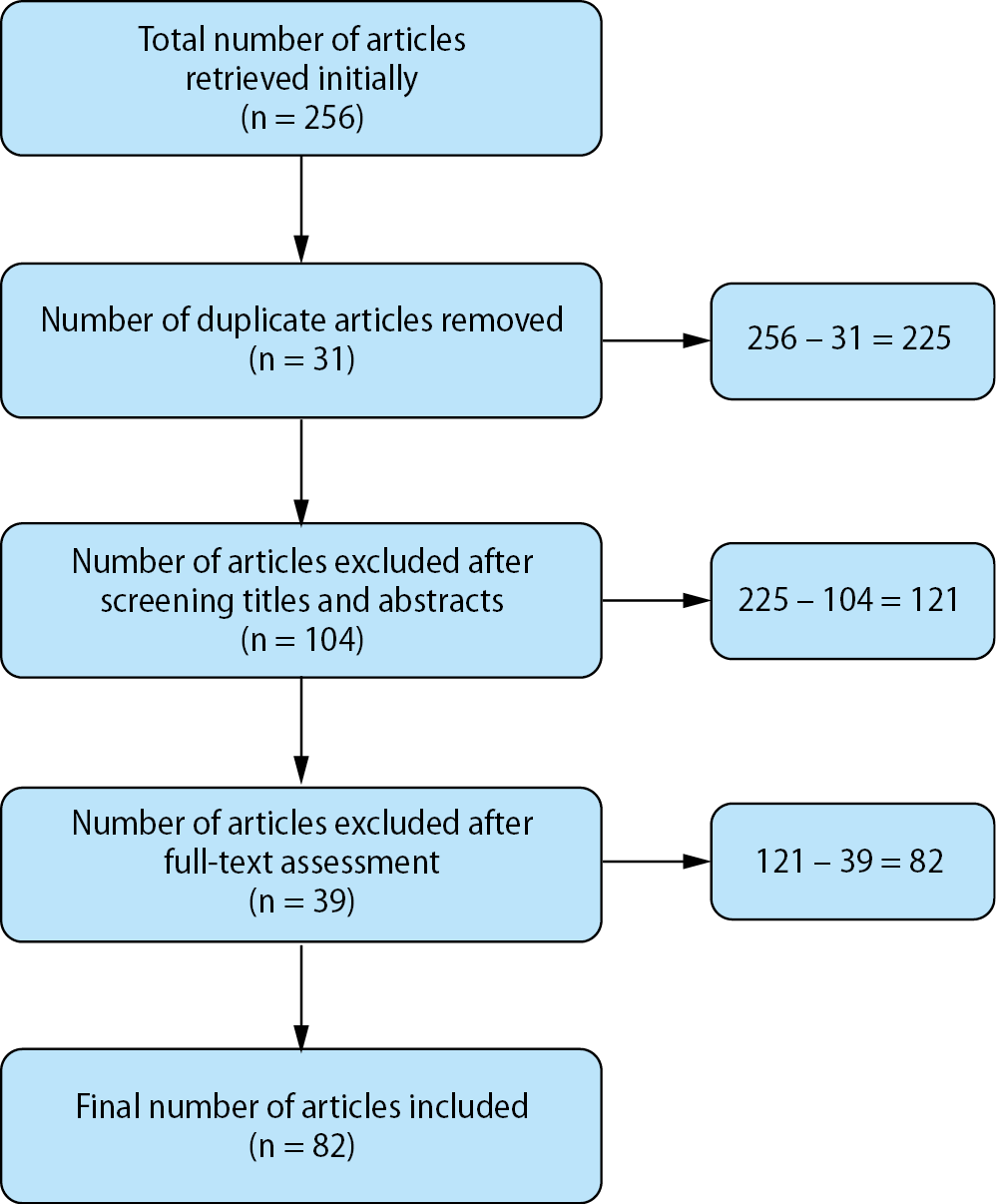
Databases including PubMed, Web of Science, Embase, and Scopus were searched up to March 2025, primarily using the following terms and their combinations: “MSI-H,” “dMMR,” “colorectal cancer,” “immune microenvironment,” “immune checkpoint inhibitors,” “immunotherapy,” “tumor mutational burden,” “single-cell sequencing,” and “spatial transcriptomics,” among others. To ensure comprehensiveness, we also performed a “snowball” tracing search of the reference lists of the included studies. After exporting the literature, duplicate records were first removed using EndNote 20 (Clarivate, London, UK). Subsequently, 2 researchers (Y.Z. and L.L.) independently conducted a preliminary screening of titles and abstracts. Any discrepancies were resolved through discussion with a 3rd researcher (B.Z.). inclusion criteria were as follows: 1) studies relevant to immune microenvironment characteristics or immunotherapy in MSI-H/dMMR colorectal cancer; 2) study types including original research (basic or clinical), retrospective or prospective cohort studies, or high-quality reviews; and 3) complete experimental or clinical data supporting the research objectives. The exclusion criteria were as follows: 1) irrelevance to the topic of this review; 2) non-peer-reviewed literature or conference abstracts with insufficient information; and 3) duplicate publications or redundant data. Uniform data extraction was performed for the final included literature, encompassing: 1) study population and sample size; 2) MSI-H/dMMR classification and detection methods; 3) methods for immune microenvironment analysis (such as immunohistochemistry (IHC), single-cell RNA sequencing (scRNA-seq), spatial transcriptomics, etc.); and 4) main findings and clinical significance. Considering the level of evidence of the included literature, we comprehensively evaluated the reliability and applicability of the findings. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart outlines the process from the initial retrieval to the final inclusion of the literature (Figure 1).
The core role of the tumor immune microenvironment in MSI-H/dMMR colorectal cancer
High tumor mutation burden and neoantigen generation
Due to defects in DNA mismatch repair, MSI-H/dMMR CRC produces frameshift and insertion/deletion mutations scattered throughout the genome, generating a large number of neoantigens and resulting in an extremely high TMB, often several times higher than that of MSS tumors.7 A high TMB increases the opportunities for antigen presentation by MHC class I molecules, thereby stimulating the clonal expansion of effector T cells. Studies have shown a positive correlation between the abundance of neoantigens and the level of tumor-infiltrating lymphocytes (TILs) in MSI-H/dMMR tumors, and this “antigen flood” phenomenon can activate the immune system. In addition, a high TMB is often accompanied by the upregulation of MHC class II molecules, which is conducive to CD4+ T cell-mediated antitumor immunity.8 Therefore, TMB and neoantigen burden are regarded as key markers for predicting the efficacy of ICIs in MSI-H/dMMR CRC.9 However, TMB is not absolutely reliable; a small number of MSS CRC cases can also exhibit TMB levels similar to those of MSI-H tumors,10 indicating the need for comprehensive evaluation in conjunction with other microenvironmental factors.
Microenvironment constituent elements and synergistic effects
The TME of MSI-H/dMMR CRC is composed of multiple cell types and factors that influence the intensity of the immune response and therapeutic outcomes. Immune cells are the core component: MSI-H/dMMR tumors are enriched with large numbers of CD8+ cytotoxic T cells and Th1-type CD4+ T cells, accompanied by high expression of cytokines such as interferon gamma (IFN-γ), thereby presenting an “inflammatory” state.11 The proportion of regulatory T cells (Tregs) is relatively decreased, promoting antitumor immunity.12 Natural killer (NK) cells and γδ T cells also play important roles; MSI-H CRC lacking human leukocyte antigen class I (HLA-I) can mediate ICI sensitivity through γδ T cells.13
Tumor-associated macrophages (TAMs) and myeloid-derived suppressor cells (MDSCs) have a double-edged effect: M1 macrophages secrete interleukin (IL)-12 and other factors to enhance anticancer immunity,14 whereas M2 macrophages enriched in some MSI-H CRCs express PD-L1, thereby inhibiting T cell function. Cancer-associated fibroblasts (CAFs) and endothelial cells constitute the tumor stroma and vascular network; CAFs can thicken the stroma and obstruct T cell infiltration via pathways such as transforming growth factor beta (TGF-β), while high endothelial microvasculature facilitates lymphocyte entry into the tumor bed.15 Immunosuppressive molecules (such as IL-10 and vascular endothelial growth factor (VEGF)) and metabolic factors (such as lactate) also continuously shape the immune landscape.
Clinical significance
The immune microenvironment features of MSI-H/dMMR CRC determine its high sensitivity to ICI treatment: A large number of CD8+ TILs and high PD-1/PD-L1 expression constitute the basis of immunotherapy.16 In a study involving more than 450 CRC cases, the TIL density in the MSI-H subgroup was significantly higher than that in the MSS subgroup, and high TIL density was associated with longer survival.17 For MSI-H/dMMR CRC patients not receiving immunotherapy, abundant immune infiltration is associated with a slightly better prognosis than in MSS CRC, with a lower recurrence risk in stages I–II.18
Multiple studies have also indicated better clinical outcomes in MSI-H/dMMR CRC patients in stages I–III, including significantly reduced recurrence risk and prolonged disease-free survival (DFS) and overall survival (OS),19 which are closely associated with high levels of CD8+ T cell infiltration, Th1-type immune responses, and strong neoantigen-induced immune effects within the TME. At the metastatic stage, only about 5% of mCRC cases remain MSI-H, and this advantage disappears; however, the enriched immune microenvironment still allows some patients to significantly benefit from immune checkpoint inhibitor treatment.20
Timely identification of MSI-H/dMMR status is crucial for clinical decision-making, and MSI testing has become routine in the molecular diagnosis of CRC, not only for Lynch syndrome screening but also as a companion diagnostic for immunotherapy.21 These studies further support the close association between the unique immune microenvironment of MSI-H/dMMR CRC and patient prognosis, providing a reference for the clinical identification of potential beneficiaries.
Key immune cell subpopulations and the heterogeneity of treatment response
CD8+ cytotoxic T cells are the main antitumor force in MSI-H/dMMR CRC, and the intratumoral density of CD8+ T cells is positively correlated with ICI efficacy and survival.22 PD-1 inhibitors can restore the killing function of exhausted CD8+ T cells. Postoperative analyses indicate that CD8A gene (a T cell cytotoxic molecule) expression is significantly higher in ICI responders than in non-responders. Th1-type CD4+ T helper cells promote the proliferation and activation of CD8+ T cells by secreting IL-2 and IFN-γ, which are also crucial in the MSI-H microenvironment.23
In contrast, Tregs (FoxP3+) infiltrate at relatively lower levels in MSI-H CRC, which benefits immune efficacy.24 It should be noted that there is heterogeneity in T cell subpopulation composition among different patients; some MSI-H tumors are “indifferent,” exhibiting few CD8+ T cells and a higher proportion of Tregs, resulting in no initial response to ICIs.25
Atypical T cells: The role of γδ T cells
The γδ T cells combine both innate and adaptive immune features and possess MHC-nonrestricted cytotoxic activity. In CRC, γδ T cells are mainly of the Vδ1+ phenotype, and their degree of infiltration is often associated with an improved prognosis.26 In MSI-H CRC with HLA-I deficiency, γδ T cells may replace CD8+ T cells in performing immune surveillance.
Yu et al. reported that the response of HLA-I-negative dMMR CRC to ICIs depends on the function of tumor-infiltrating γδ T cells, suggesting that they serve as a “replacement” cell type in the immune response of MSI-H CRC, especially in immune escape phenotypes.27
Myeloid cells: The heterogeneity driven by MDSCs and macrophages
MDSCs and TAMs often exert immunosuppressive effects. The number of MDSCs in the peripheral blood and tumor tissue of MSI-H CRC patients is positively correlated with resistance to ICI treatment.28 Tumor-associated macrophages have 2 polarized states: M1 and M2. M1 macrophages are pro-inflammatory and antitumor, whereas M2 macrophages secrete IL-10, TGF-β, and other factors that inhibit immune responses.29 Compared with MSS CRC, MSI-H CRC has more M1 macrophages and fewer M2 macrophages at the invasive margin,30 which may explain its greater sensitivity to immunotherapy. However, in MSI-H patients with ICI resistance, TAMs can repolarize toward the M2 phenotype and upregulate immunosuppressive molecules such as PD-L1 and indoleamine 2,3-dioxygenase (IDO).31 Therefore, combined strategies targeting MDSCs and M2 TAMs (e.g., CSF-1R or IDO inhibitors plus PD-1 antibodies) are being explored to improve efficacy in refractory MSI-H CRC patients.32
Spatial distribution characteristics: Differences in immune cell location within the tumor
In addition to quantity, the spatial distribution of immune cells in the TME also determines their function. In MSI-H/dMMR CRC, TILs often penetrate deep into the tumor center to form an “immune-hot” zone, whereas in MSS CRC, TILs are mostly confined to the invasive margin, presenting an “immune exclusion” state.33 High-resolution spatial omics comparing the tumor–stroma boundary in dMMR and pMMR CRC reveal that the boundary in dMMR CRC is enriched with LAMP3+ dendritic cells and CXCL13+ T cell clusters, facilitating the formation of effective immunological synapses, whereas in pMMR CRC, CAFs and collagen deposition at the boundary hinder T cell infiltration.34 Pelka et al. reported that MSI-H tumors contain a multicellular immune hub composed of densely packed antigen-presenting cells and effector T cells adjacent to surrounding tumor cells, which is conducive to immune attack, whereas MSS tumors often lack this structure.35
Mechanisms of resistance and hyperprogression
Regulation of immune checkpoints and signaling pathways
Although MSI-H/dMMR CRC is generally sensitive to ICIs, some patients exhibit primary or acquired resistance, with various underlying mechanisms. Abnormalities in the PD-1/PD-L1 axis are common factors; Chen et al. found that in MSI-H CRC, PD-L1 is primarily expressed by macrophages rather than by tumor cells, which may reduce the efficacy of ICIs.36 The classic JAK/STAT pathway is crucial for antitumor immunity, and loss-of-function mutations in JAK1 or JAK2 render tumors unresponsive to IFN-γ, allowing them to escape immune surveillance. Although their incidence is only about 4–7% in MSI-H CRC,37 once they occur, they are often directly related to ICI resistance.38
Hyperactivation of the Wnt/β-catenin pathway can also drive immune evasion; excessive Wnt signaling suppresses chemokine production and hinders the recruitment of dendritic cells and T cells.39 In MSS CRC, Wnt signaling promotes CAFs to secrete more TGF-β and exclude T cells. If MSI-H CRC also develops secondary Wnt abnormalities, it may transform into an immune-indifferent phenotype, leading to resistance.40 Therefore, combination therapies targeting key signaling nodes such as JAK or Wnt may overcome some forms of resistance.
Definition of hyperprogression and exploration of mechanisms
Hyperprogression refers to the rare but abnormally accelerated disease progression following ICI treatment. There is no unified standard, but it is generally defined by a significant increase in tumor growth rate on imaging or rapid clinical deterioration.41 Although HPD is rare in MSI-H/dMMR tumors, it is not nonexistent. Zhou et al. reported a case of dMMR small intestinal cancer exhibiting HPD after treatment with a PD-1 antibody, suggesting that high lactate dehydrogenase levels, extremely low TMB and TIL infiltration, and abnormally activated TGF-β signaling might be related.42 In other cancers, MDM2/MDM4 amplification and epidermal growth factor receptor (EGFR) mutations have been associated with an increased risk of HPD, presumably by promoting cell-cycle progression and inhibiting apoptosis, thereby accelerating tumor growth in an immunosuppressive environment. The mechanism of HPD in MSI-H CRC is not yet clear; however, given that some CRC cases harbor MDM2 amplification and EGFR mutations,43 clinicians should remain vigilant. For cases with rapid progression, it may be prudent to test for these genes and adjust treatment accordingly.
Antigen presentation defects and HLA loss
Although MSI-H CRC is rich in neoantigens, if the antigen presentation pathway is compromised, the immune system may still “turn a blind eye.” β2-microglobulin (B2M) is an essential component of MHC-I molecules, and its gene mutations account for approx. 24% of MSI-H CRC cases, resulting in almost no HLA-I antigen presentation in tumor cells, thus evading cytotoxic T lymphocyte (CTL) recognition. In addition, mutations in HLA-A/B/C and their transcriptional activator NLRC5 are also common. A study by Kloor et al. showed that 72% of MSI-H CRC harbor at least 1 genetic alteration in the HLA-I antigen presentation pathway, with more than half being loss-of-function mutations.44
This indicates that most MSI-H CRC tumors undergo immune selection pressure during evolution, tending to “shut down” antigen presentation to escape immune surveillance. For such tumors, PD-1 monotherapy is limited, necessitating combination therapy with CTLA-4 inhibitors or other immune strategies to activate NK or γδ T cells and other nonconventional immune pathways. Current studies such as COSMIC-312 are evaluating dual checkpoint blockade (PD-1 + CTLA-4) in MSI-H CRC, which is expected to partially overcome resistance caused by antigen presentation defects.45
Metabolic reprogramming-mediated immunosuppression
Tumor metabolism and the immune microenvironment influence each other, and metabolic reprogramming can promote immune evasion. Tryptophan (Trp) metabolism is a typical example: tumor cells and MDSCs overexpress IDO1, breaking down large amounts of Trp into kynurenine (Kyn), leading to Trp depletion and Kyn accumulation, which in turn block the T-cell cycle and induce Treg expansion.46 Research has shown that high IDO1 expression is associated with primary resistance of MSI-H CRC to PD-1 inhibitors.47 Clinical phase I/II trials have attempted to combine the IDO inhibitor BMS-986205 with PD-1 antibodies for the treatment of MSS CRC, and although they did not meet the primary endpoint, subgroup analyses showed some efficacy,48 indicating the value of further exploration of metabolic targets. Lactate is also an important metabolic factor: MSI-H/dMMR CRC undergoes high glycolysis, producing large amounts of lactate, which reduces the local pH, inhibits T- and NK-cell activity, and recruits M2-type macrophages. Sun et al. noted that lactate induces dendritic cell tolerance, reduces IL-12 secretion, and weakens CTL function. Higher lactate dehydrogenase A (LDHA) expression in pMMR CRC than in dMMR CRC is considered a marker of an immunosuppressive environment.49 Therefore, inhibitors targeting IDO1 or LDHA may improve the TME and enhance the efficacy of ICIs. Preclinical models have shown that inhibiting LDHA can restore T cell activity and enhance the effect of PD-1 antibodies.50
Advances in single-cell sequencing and spatial transcriptomics
Single-cell RNA sequencing for heterogeneity analysis
Traditional bulk tissue sequencing often masks differences among microenvironmental cells, whereas scRNA-seq can delineate gene expression profiles of different cell types at the single-cell level. In recent years, multiple studies have applied scRNA-seq to CRC, revealing subtle differences in immune microenvironment composition between MSI-H and MSS tumors. Wu et al. performed scRNA-seq on 6 cases of MSI-H mCRC (3 resistant to ICIs and 3 sensitive), analyzing over 56,000 cells.51 The results showed that the greatest differences between the responsive and resistant groups lay in the proportions of CD8+ T cells and monocytes: Patients in the responsive group had higher CD8+ T cell infiltration, whereas resistant patients exhibited increased proportions of immunosuppressive monocytes, implying that myeloid immunity interferes with ICI efficacy. The scRNA-seq can also uncover novel cell subpopulations that are not distinguishable using traditional markers. They have identified a cluster of CD8+ T cells highly expressing LAG3 and PDCD1 that were enriched in the resistant group, indicating the potential for combination therapy with LAG-3 inhibitors. Another study incorporating T cell receptor sequencing found that some MSS CRCs still possess numerous memory CD8+ T cell clones that, if activated, could potentially yield a response to immunotherapy.52
Spatial transcriptomics for visualizing spatial structure
Although scRNA-seq reveals cellular diversity, it loses spatial information. Spatial transcriptomics (10× Visium, Slide-seq, Stereo-seq, etc.) can measure location-specific gene expression in tissue sections. Feng et al. used Stereo-seq to analyze 5 untreated pMMR and 5 post-PD-1-treated dMMR CRC samples,53 constructing a digital tumor atlas and identifying an “immune-activated” spatial subtype enriched with LAMP3+ dendritic cells and CXCL13+ T cells at the tumor–stroma interface in dMMR CRC, which was positively correlated with ICI response. In contrast, pMMR tumors presented more tumor cell–fibroblast hybrid clusters that isolated immune cells. Another study employed Visium to compare mCRC tissues before and after neoadjuvant immunotherapy,54 showing that PD-1 antibodies facilitated deeper T-cell infiltration at the tumor boundary in dMMR CRC and reduced CAF activity, transforming it into an “immune-hot” central state.55 The “immune hub” reported by Pelka et al.35 was also identified through spatial analysis of immune aggregates within the tumor.
Advantages and challenges of new techniques
Single-cell and spatial omics provide unprecedented high resolution, detecting rare cell subpopulations without preset markers and enabling dynamic monitoring of multiple time point samples to track immune microenvironment remodeling. Challenges include high data complexity, requiring robust bioinformatics and rigorous statistical methods to avoid false positives or over-interpretation; elevated costs and a need for fresh tissue, posing a higher threshold for most hospitals; and limited sample sizes that may lack representativeness, leaving the question of broader applicability to further validation.
Multi-omics integration and novel biomarkers
Colorectal cancer involves multi-level changes in the genome, transcriptome, proteome, metabolome, and microbiome. A single-dimensional biomarker is often insufficient to comprehensively predict treatment outcomes, so multi-omics integration has garnered increasing attention.56 For MSI-H/dMMR CRC, combining genomic mutations (TMB, HLA mutations), transcriptomic data (immune gene expression), proteomic data (immune infiltration scores), and microbiome data can provide a more complete picture of the tumor immune landscape.57 Cheng et al. conducted a multi-omics study on MSI-H/dMMR advanced gastrointestinal tumors, collecting 16S microbiome sequencing data, blood metabolomics, and cytokine profiles, together with tumor molecular analyses. They found that responders were enriched in short-chain fatty acid-producing bacteria (e.g., Akkermansia muciniphila) and had higher levels of Trp and other metabolites in the blood, suggesting that integrating microbiome–metabolism–immune signals can form a comprehensive predictive model.58 An immune gene expression profile (GEP) score, which weights and sums the expression of multiple immune-related genes, can effectively predict PD-1 antibody efficacy59; in MSI-H CRC patients, a high GEP score is often associated with a durable response. The Immunoscore, which quantitatively assesses CD3+ and CD8+ T cell density in both the tumor center and the invasive margin via immunohistochemistry, outperforms TNM staging in predicting the prognosis of localized CRC.60 In the context of immunotherapy, MSI-H mCRC with a high Immunoscore is more likely to benefit from ICIs. The serum kynurenine/tryptophan ratio (Kyn/Trp) reflects IDO activity; Cheng et al. found that a high Kyn/Trp ratio was significantly associated with early progression on immunotherapy and may be used to identify patients with primary resistance. The composition of the gut microbiome affects ICI efficacy61; for instance, increased abundance of A. muciniphila and Bifidobacterium is linked to ICI response in multiple tumor types.62 In CRC, some researchers have constructed a “probiotic index” to assess the abundance of beneficial bacteria, finding that MSI-H CRC patients with a higher index respond better to PD-1 antibodies. The NICHE-2 trial applied neoadjuvant nivolumab plus ipilimumab in locally advanced (stage III) dMMR CRC and collected tumor samples before and after treatment for multi-omics analysis, showing that most patients achieved a pathological complete response. Subsequent transcriptome and T-cell receptor omics analyses will further elucidate molecular features related to efficacy.63 The DURVA-TREM trial is evaluating the efficacy of durvalumab (anti–PD-L1) combined with tremelimumab (anti-CTLA-4) in MSI-H mCRC, using ctDNA and peripheral immune profiling to identify predictive factors.64
Gut microbiome interventions are also under exploration, where probiotics or fecal microbiota transplantation combinfed with ICIs are being used in MSS CRC to potentially convert it into a “hot” tumor.65 In a study of 20 MSS CRC patients, anti-PD-1 therapy plus fecal microbiota transplantation was accompanied by pre- and post-treatment transcriptomic and microbiome analysis. Some previously “cold” tumors showed upregulated IFN-γ signaling and increased TILs.66 Proteomics can capture post-translational modifications and protein interaction networks, thereby identifying key regulatory proteins associated with immune escape or therapeutic resistance. Metabolomics helps to elucidate the roles of lactate, Kyn, and other metabolites in immune suppression or immune activation processes. Existing studies have utilized proteomics to identify differentially expressed or modified signaling molecules, such as phosphorylated JAK/STAT proteins and critical immune checkpoint proteins, providing more precise evidence for multi-pathway combination therapies and the discovery of new therapeutic targets67; researchers have also used metabolomics approaches to reveal the close association between the Kyn–Trp pathway, T-cell exhaustion, and immunosuppressive TME.68 In combination with genomic, transcriptomic, and microbiomic data, proteomics and metabolomics analyses can further refine the comprehensive landscape of the TME, facilitating the identification of biomarkers with greater clinical utility and guiding personalized immunotherapy strategies.
Unresolved key issues and future perspectives
Dynamic monitoring and multi-time point sampling
The TME continually evolves during disease progression and treatment. Most studies based on single-time point analyses have difficulty capturing its dynamic changes. Larger-scale prospective studies need to collect tissues from the same patient at multiple time points before, during, and after treatment through longitudinal cohorts, combined with dynamic indicators such as peripheral T cell subsets and ctDNA to monitor shifts in the immune landscape throughout the course of ICIs.69 Neoadjuvant immunotherapy can perform multi-omics analyses before, during, and after treatment to track changes in immune infiltration from baseline to pathological remission; minimally invasive liquid biopsies can capture the real-time status of peripheral blood immune cells.70 Although multi-time point sampling has ethical and feasibility concerns, patient-derived xenograft (PDX) mouse models with humanized immune systems can only partially simulate tumor evolution.71
Exploration of combination therapy strategies
Although single checkpoint blockade in MSI-H/dMMR CRC shows significant effectiveness, improvements are still needed for resistant and MSS populations. Multimodal combination strategies remain under continuous exploration. For instance, PD-1 + CTLA-4 can increase response rates in metastatic MSI-H CRC,72 and other studies incorporate LAG-3 or TIGIT antibodies to further activate exhausted T cells. Radio-chemotherapy (e.g., oxaliplatin) can induce immunogenic cell death and enhance immune stimulation in the TME73; small-molecule targeting (JAK/STAT agonists or Wnt inhibitors) can also alleviate immunosuppression.74 Personalized neoantigen vaccines have shown promise in melanoma,75 though their clinical application in MSI-H CRC still lacks sufficient evidence; TIL or TCR-T cell therapies for MSI-H CRC are under clinical investigation (NCT03412877), and their actual clinical benefits require further evidence support.
Data standardization and multidisciplinary integration
Multi-omics and high-throughput technologies generate massive multidimensional data, urgently requiring unified data processing standards and multidisciplinary collaboration.76 Employing uniform formats and metadata descriptions (e.g., clinical information, sequencing parameters) facilitates subsequent meta-analyses. Artificial intelligence (AI) can extract patterns from multi-level data to predict individual treatment responses,77 but close cooperation with tumor biologists and clinical experts is needed to ensure practicality. Some studies have attempted to integrate radiomics, pathological images, and gene expression with deep learning models to predict MSI status,78 with feasibility and accuracy still needing further validation.
Controversial issues and future research directions
The value of anti-EGFR therapy in the MSI-H setting remains controversial. Conventional wisdom holds that RAS/BRAF wild-type CRC is limited to left-sided MSS cases for use, but recent reports show significant tumor shrinkage with cetuximab in patients who are MSI-H and RAS/BRAF wild-type,79, 80 though the applicable population still requires more sufficient multicenter validation. Other studies suggest that MSI-H/dMMR tumors under high mutation and strong immune pressure may more easily develop immune evasion, with some patients experiencing relapse after immunotherapy and loss of dMMR features,81 potentially related to immune clonal selection or inadequate treatment. Additionally, the impact of the tumor microbiome (e.g., Fusobacterium spp.) on the TEM and mechanisms maintaining immune memory exhibit variations, and specific intervention strategies and clinical benefits currently lack large-sample evidence.82 Further in-depth prospective studies and multi-dimensional validations may advance the refinement of personalized therapeutic strategies.
Limitations of the study
This review still has limitations in both data collection and scope. It relies primarily on published literature without conducting a meta-analysis, and may be influenced by study biases (such as differences in study populations and technical platforms). Some mechanisms (e.g., the potential mechanisms of HPD and the value of new biomarkers) are based on limited evidence and require further experimental validation. Since MSI-H/dMMR CRC accounts for a relatively small proportion of cases and single-cell and spatial omics studies have limited sample sizes, caution is needed when applying these conclusions to larger populations. Due to space constraints, an in-depth discussion of neoadjuvant immunotherapy and insights from other MSI-H solid tumors was not possible. Readers should critically integrate the latest developments with each patient’s specific circumstances.
Conclusions
MSI-H/dMMR CRC is characterized by a high mutation burden and abundant immune infiltration, conferring a relatively favorable prognosis and providing ideal conditions for immune checkpoint inhibitor therapy. In recent years, PD-1 monoclonal antibodies have shown advantages in first-line treatment, and dual blockade of PD-1/CTLA-4 has further enhanced clinical benefits. However, some patients still exhibit no response or develop resistance. This paper has outlined the immune microenvironment characteristics of MSI-H/dMMR CRC, including the strong immune response driven by a high TMB and neoantigen burden, as well as the mechanisms of immune escape caused by HLA mutations, JAK pathway abnormalities, immunosuppressive cell infiltration, and metabolic reprogramming. Single-cell and spatial multi-omics technologies are helping us more accurately characterize immune cell types and distributions, clarifying individual differences in treatment outcomes.
Use of AI and AI-assisted technologies
Not applicable.