Abstract
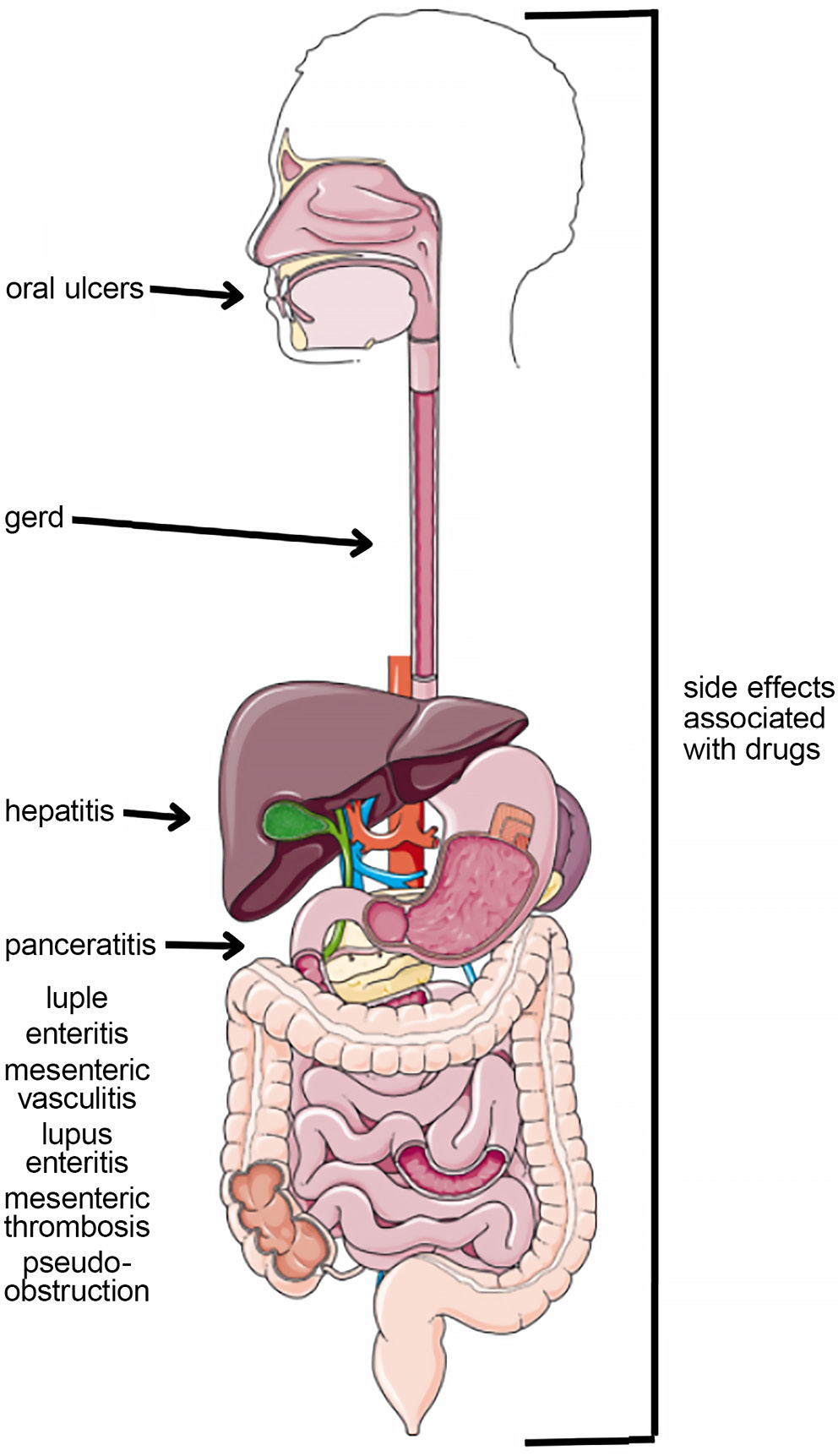
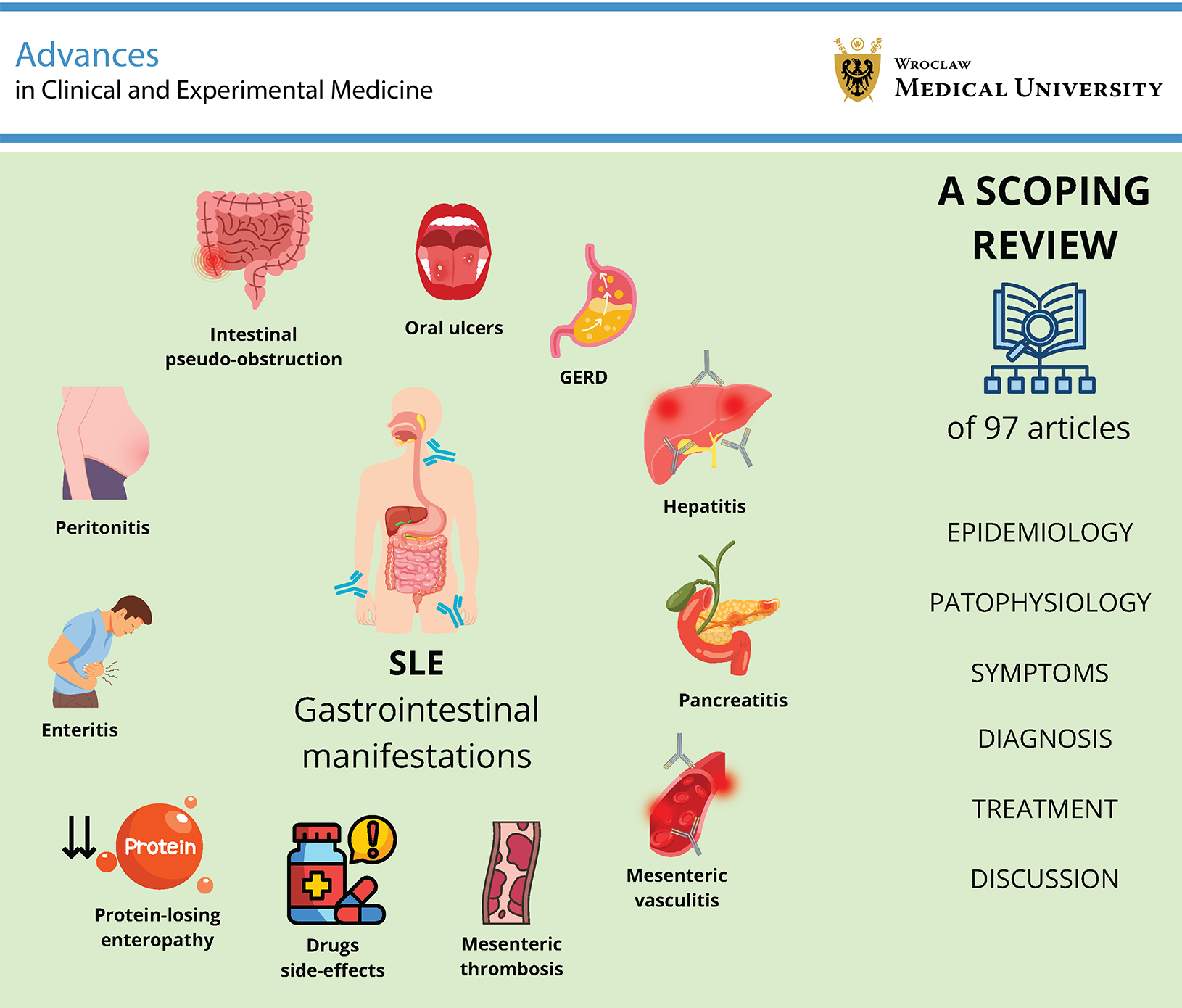
Systemic lupus erythematosus (SLE) is a complex autoimmune disease characterized by a broad spectrum of clinical manifestations, including gastrointestinal (GI) involvement. Although the joints, skin, and kidneys are most commonly affected, GI manifestations are frequently underrecognized despite their potential to significantly influence patient outcomes. Eleven major GI manifestations have been identified and described: oral ulcers, lupus enteritis (LE), lupus peritonitis (LP), mesenteric vasculitis, mesenteric thrombosis, protein-losing enteropathy (PLE), intestinal pseudo-obstruction (IPO), lupus pancreatitis, lupus hepatitis (LH), gastroesophageal reflux disease (GERD), and medication-related adverse effects.
These manifestations may present with nonspecific symptoms, such as abdominal pain, diarrhea, vomiting, and weight loss, which often complicate timely diagnosis. Imaging modalities, particularly contrast-enhanced computed tomography, together with serological markers, including antinuclear antibodies (ANA) and complement levels, play a central role in diagnosis. Corticosteroids remain the cornerstone of treatment, whereas immunosuppressive agents and biologic therapies are reserved for refractory cases. Medication-induced GI adverse effects, particularly those associated with glucocorticoids, nonsteroidal anti-inflammatory drugs (NSAIDs), and immunosuppressive agents such as azathioprine (AZA) and cyclophosphamide (CPA), also represent important contributors to GI pathology in patients with SLE. Gastrointestinal involvement in SLE is heterogeneous and may be severe. Increased awareness, early recognition, and individualized treatment strategies are essential for improving patient outcomes. Further research is required to establish standardized diagnostic criteria and therapeutic guidelines for GI manifestations in SLE.
Key words: lupus erythematosus, rheumatology, gastroenterology
Introduction
Systemic lupus erythematosus (SLE) is one of the most prevalent multisystem autoimmune disorders. It is characterized by the production of a broad spectrum of antinuclear antibodies (ANA) and the deposition of immune complexes in various organs, leading to inflammation and tissue damage. Although SLE most commonly affects the joints, skin, and kidneys, it may also manifest with respiratory, neurological, or gastrointestinal (GI) symptoms, reflecting the systemic nature of the disease (Figure 1).1, 2
The global incidence of SLE is estimated at 5.14 cases per 100,000 person-years, including 8.82 cases among women and 1.53 cases among men. The estimated worldwide prevalence is 43.7 cases per 100,000 individuals, with approx. 78.73/100,000 women and 9.26/100,000 men affected. Most documented cases have been reported in more developed regions, particularly in Europe and North America. However, these data should be interpreted with caution due to the lack of reliable epidemiological data from certain countries.3 It is also important to note that SLE is most commonly diagnosed in young adults. Moreover, earlier disease onset is associated with a more aggressive clinical course. This observation highlights the importance of early and accurate diagnosis of the disease.4
As mentioned previously, SLE may also involve the GI tract among the many organ systems affected by the disease. Abdominal pain and other GI symptoms are associated with a broad differential diagnosis.5 Because nonspecific GI manifestations may represent the initial clinical presentation of SLE, and delayed diagnosis may lead to a more severe disease course, accurate classification and comprehensive understanding of the epidemiology, clinical manifestations, diagnostic approaches, and treatment of GI involvement in SLE are essential.6 This paper presents a scoping review of the gastroenterological manifestations of SLE. We systematically mapped the epidemiology, pathophysiology, clinical features, diagnostic approaches, and management strategies related to eleven distinct GI manifestations: oral ulcers; gastroesophageal reflux disease (GERD); enteritis; peritonitis; vasculitis; thrombosis; protein-losing enteropathy (PLE); intestinal pseudo-obstruction (IPO); pancreatitis; hepatitis; and drug-related adverse effects (Table 1).
Objectives
This scoping review aims to systematically map current evidence on the epidemiology, pathophysiology, clinical presentation, diagnosis, and management of gastrointestinal manifestations in SLE. By comprehensively describing eleven distinct GI manifestations, we seek to raise clinical awareness, highlight gaps in standardized diagnostic and therapeutic guidelines, and identify priorities for future research.
Materials and methods
The literature search was conducted using the PubMed, Embase, and Google Scholar databases, as well as references from relevant articles and online sources. The following medical keywords were used, the majority of which were Medical Subject Headings (MeSH) terms: “lupus” OR “SLE” combined with “GI system”, “colitis”, “mesenteric vasculitis”, “intestinal pseudo-obstruction (IPO)”, “GERD”, “gastroesophageal reflux”, “oral cavity”, “peritonitis”, “hepatitis”, “pancreatitis”, “enteritis”, “mesenteric vascular thrombosis”, “lupus-associated protein-losing enteropathy (LUPLE)”, “glucocorticosteroids”, “hydroxychloroquine”, “azathioprine (AZA)”, “nonsteroidal anti-inflammatory drugs (NSAIDs)”, “cyclophosphamide”, and “belimumab”. The authors screened article titles and abstracts to identify relevant publications. Original articles and review papers published in 2020 or later were included. Older articles and case reports were considered only when more recent literature was unavailable. The final literature search was performed on May 25, 2025. The exclusion criteria were as follows: articles published before 2020, publications in languages other than English, studies with very small sample sizes, and case reports when review articles or meta-analyses were available.
Oral cavity
Oral cavity involvement is a common manifestation of SLE. Du et al. reported that the prevalence of oral manifestations may reach 30%.7 Oral ulcers, the most frequently observed oral pathology, are included in the European Alliance of Associations for Rheumatology (EULAR) recommendations for the management of SLE. These lesions may be painful or remain asymptomatic and unnoticed by the patient. Clinically, they typically present as pale yellow or grayish-white superficial ulcers.8
Other reported oral manifestations include hyperkeratosis, erosions, oral pigmentation, fissured tongue, and xerostomia resulting from oral dryness.9 The hard palate and buccal mucosa are the most common sites of involvement. Therefore, proper oral and dental hygiene represents an important aspect of prophylaxis and supportive care. Management of oral lesions includes a variety of therapeutic approaches, with antimalarial agents considered first-line treatment. In addition, standard SLE therapies, including glucocorticosteroids, immunosuppressive agents, and other systemic treatments, may also be used.10
GERD
One study reported that nearly half of patients with SLE experienced esophageal involvement, most commonly regurgitation (27.3%) and heartburn (24.6%).11 The pathophysiology of esophageal motility disorders in SLE remains unclear. Earlier studies suggested that these abnormalities may result from ischemic vasculitis, muscle atrophy, or inflammatory involvement of the esophageal musculature. Symptomatic treatment is primarily based on proton pump inhibitors, prokinetic agents, and high-dose H2-receptor blockers.6
Intestinal pseudo-obstruction
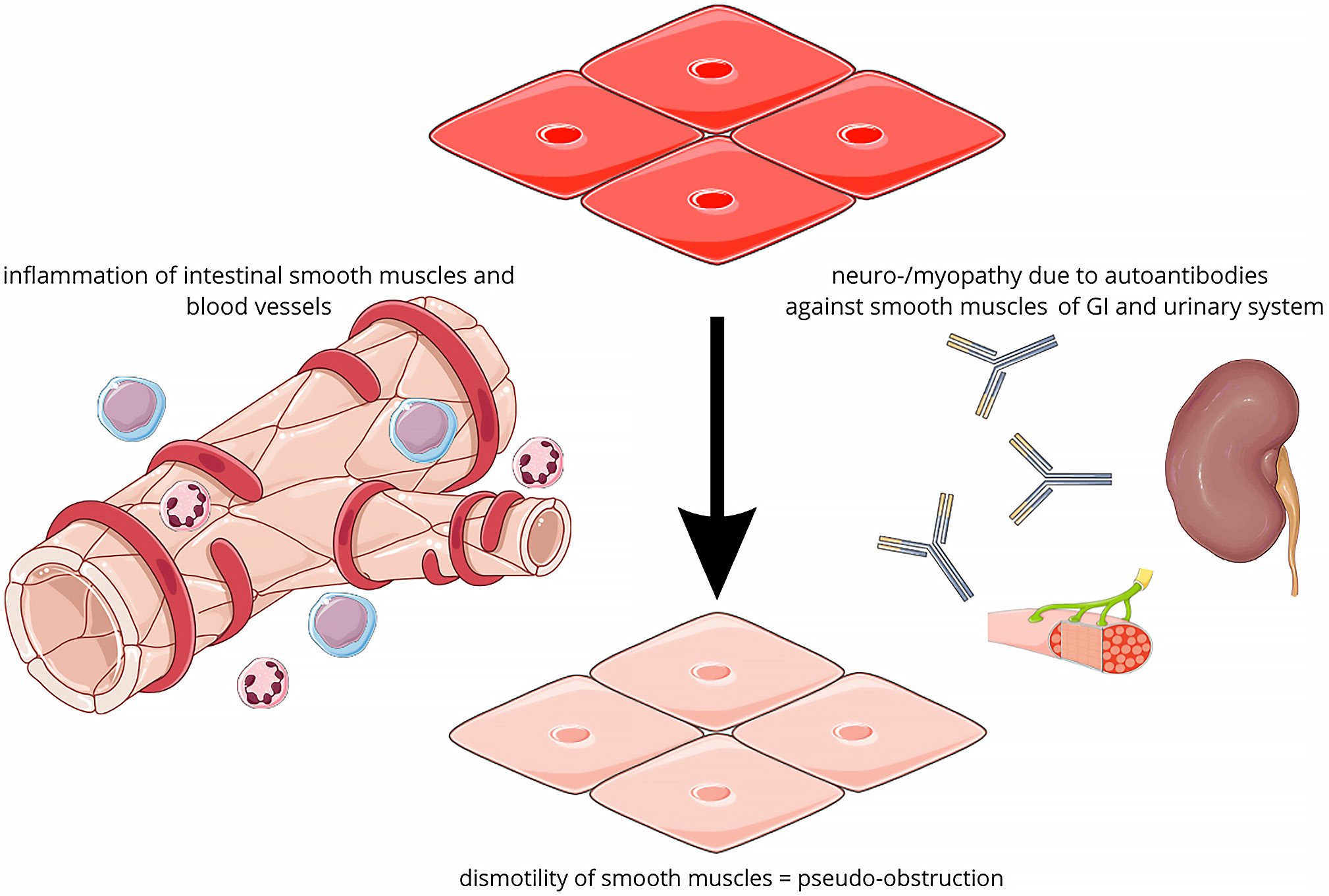
Intestinal pseudo-obstruction is a rare gastrointestinal manifestation of SLE, characterized by symptoms resembling mechanical or functional bowel obstruction despite the absence of an identifiable obstructive cause.12 It may occur either as the initial manifestation of the systemic disease or as one of multiple clinical manifestations of SLE.13 The prevalence of IPO is estimated to affect approx. 1–2% of patients with SLE.14 Several theories have been proposed regarding the pathophysiology of this manifestation of lupus; however, none has been conclusively confirmed due to the limited number of reported cases. Based on current evidence, 2 principal mechanisms have been suggested. One hypothesis involves vasculitis affecting the smooth muscles of the GI tract, leading to ischemia and dysfunction of the affected tissue, which subsequently impairs normal smooth muscle contraction. The 2nd hypothesis, frequently associated with ureterohydronephrosis and other genitourinary complications, suggests generalized smooth muscle dysmotility caused by myopathic or neurogenic abnormalities. These alterations are thought to develop as a result of autoantibodies and immune complexes directed against smooth muscle tissue and its vasculature (Figure 2).12
Patients typically present with symptoms suggestive of bowel obstruction, including nausea, vomiting, and constipation; however, episodes of diarrhea may precede the acute phase of the disease. In addition, substantial weight loss is often observed before the onset of acute symptoms.15 In more severe cases, patients may also present with fever.16 Physical examination may reveal absent bowel sounds on auscultation, as well as diffuse abdominal tenderness and muscular guarding.17 Laboratory findings are similar to those observed in lupus enteritis (LE), including elevated C-reactive protein (CRP) levels and the presence of SLE-associated autoantibodies.18 Diagnostic imaging typically demonstrates features of bowel obstruction, such as air–fluid levels on abdominal radiography and dilated intestinal loops. A characteristic finding in this manifestation is the coexistence of bilateral hydronephrosis, which is frequently identified on computed tomography (CT).19 This phenomenon is considered highly prevalent, and its absence is often regarded as atypical and highlighted in case reports. Management of this manifestation of lupus includes not only corticosteroids and immunosuppressive agents, but also supportive measures such as nasogastric decompression, electrolyte correction, and, in selected cases, surgical intervention. Standard pharmacological treatment most commonly involves pulse methylprednisolone therapy, cyclophosphamide (CPA), and hydroxychloroquine (HCQ).17
Lupus peritonitis
Lupus peritonitis (LP) is one of the least frequent GI manifestations of SLE, and it is not described in the literature as often as other lupus features, such as lupus nephritis or enteritis. Serositis, defined as inflammation of serous membranes, is a well-established criterion of SLE. It typically involves the pleura or pericardium, with peritonitis being a far less common presentation. The reported prevalence of serositis in SLE ranges from 10% to 20%, depending on the cohort studied.20 Isolated LP is particularly rare, but cases in which it was the first manifestation of SLE have been documented.21 The pathophysiology of LP is believed to involve the formation of pathological immune complexes in the peritoneum and inflammation of local vessels and serosal surfaces. Clinically, LP can present in an acute or chronic form. The former is associated with nonspecific acute abdominal symptoms, such as abdominal pain, nausea, vomiting, and tenderness.22 Chronic manifestation is characterized by exudative ascites, which should be differentiated from appendicitis and neoplastic or infectious causes.
Diagnostic evaluation should include autoantibody testing (e.g., ANA, anti-dsDNA), complement levels, and peritoneal fluid analysis to differentiate LP from other causes.23 Currently, no specific guidelines for the treatment of LP have been developed due to its rarity and the limited amount of available literature. Despite this, available case reports demonstrate high effectiveness of intravenous or oral pulse methylprednisolone therapy.22 Immunosuppressants, such as mycophenolate mofetil, are sometimes administered together with glucocorticosteroids with satisfactory results.
Lupus hepatitis
Lupus hepatitis (LH) is a liver dysfunction associated with SLE. Since the liver is rarely a primary target organ in SLE, liver function abnormalities are not included in the diagnostic or classification criteria for the disease.24 However, up to 50% of patients with SLE are reported to experience abnormal liver function at some point in their lives, possibly related to SLE. This may result from LH, coexisting autoimmune liver diseases, or liver damage caused by non-autoimmune conditions.25 Lupus hepatitis occurs in approx. 3–8% of affected individuals and is characterized by mildly elevated transaminase levels, often without clinical symptoms.26 Elevations may be observed in liver enzymes, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT), as well as bilirubin, inflammatory markers such as erythrocyte sedimentation rate (ESR) and CRP, and SLE-specific serological markers. Laboratory findings may also reveal reduced complement levels, including C3, C4, and C1q.27
Strongly positive complement C1q deposits observed in liver immunohistochemistry are highly indicative of LH, whereas such deposits are absent in patients with other hepatic disorders.28 Patients with LH characteristically exhibit elevated anti-ribosomal P antibody levels, and liver biopsy usually reveals lobular inflammation. These features may be valuable in differentiating LH from other chronic hepatic pathologies observed in patients with SLE.29 Several studies have reported that elevated liver enzyme levels in patients with SLE usually normalize following corticosteroid treatment. In contrast, a diminished initial therapeutic response to corticosteroid treatment has been observed in patients with autoimmune hepatitis (AIH).30
Autoimmune hepatitis is a chronic, immune-mediated inflammatory liver disease characterized by elevated levels of circulating autoantibodies, hypergammaglobulinemia, and increased serum transaminase activity.31 The overlap syndrome involving AIH and SLE represents a rare complication.32 Differential diagnosis between AIH and SLE-associated LH can be demanding. Certain parameters, such as elevated antinuclear antibody (ANA) and immunoglobulin (IgG) levels, are commonly observed in both conditions. However, markers more specific for AIH and typically absent in SLE include antibodies against soluble liver antigen (SLA), liver–pancreas antigen, smooth muscle antibodies (SMA) with specificity for F-actin, and microsomal autoantibodies such as anti-liver kidney microsomal antibodies (anti-LKM antibodies).33, 34 A key distinguishing factor between AIH and SLE is liver histopathology. Patients with AIH typically present with characteristic biopsy findings, including interface hepatitis, hepatocyte rosetting, emperipolesis, and fibrosis. In comparison, liver histology in SLE usually reveals fatty degeneration or hydropic changes in hepatocytes, which are typically associated with drug-induced toxicity or nonspecific hepatic involvement.35
A recent systematic review summarized findings from 4 studies investigating the treatment of lupus-associated hepatitis, including SLE–autoimmune hepatitis (SLE-AIH) overlap, SLE-AIH–primary biliary cholangitis (PBC) overlap, and LH, encompassing a total of 59 patients. Overall, approx. 2/3 of patients (39/59) experienced favorable outcomes, while 11 patients relapsed and 3 died. Intravenous methylprednisolone (IVMP) and oral prednisolone (0.5–1 mg/kg/day), often in combination with AZA, formed the basis of both induction and maintenance therapy. Although higher doses of prednisolone (>0.25 mg/kg/day) may correlate with improved response rates, the available evidence remains limited and of low certainty. Conservative management may be appropriate for patients with mild disease presentations.
Differentiating SLE-associated hepatitis from AIH remains clinically challenging due to overlapping features; however, specific serological and histological markers may assist in establishing the diagnosis. Current limited evidence suggests that immunosuppressive therapy with corticosteroids and AZA is generally effective, although high-quality controlled studies are needed to establish standardized treatment approaches.10
Acute pancreatitis
Acute pancreatitis (AP) is an acute inflammatory condition of the pancreas that constitutes a gastroenterological emergency.36 Pancreatitis is primarily caused by alcohol consumption and gallstones. Pancreatic involvement in SLE remains a rare occurrence.37 Pancreatitis associated with SLE has a reported prevalence ranging from 0.2% to 8.2% and an annual incidence of 0.4–1.1 cases per 1,000 patients.38 If not treated promptly, more than half of patients with SLE-related AP are at risk of developing complications. The onset of pancreatitis in SLE is multifactorial and involves a complex pathophysiology, including immune-mediated pancreatic damage and vasculitis.39 Yuan et al. identified 132 cases of abdominal pain considered to be SLE-related. Among these, lupus-associated pancreatitis accounted for 17.4% of patients (23 out of 132).40 One study reported that in 97% of cases, the diagnosis of pancreatitis was confirmed by laboratory evidence of elevated serum amylase or lipase levels.41 Pancreatic involvement represents a severe and potentially life-threatening clinical condition, often occurring as part of widespread multiorgan involvement, such as macrophage activation syndrome (MAS).42 Recent studies suggest that favorable outcomes in the management of acute pancreatitis associated with SLE (SLEAP) may be achieved with higher doses of glucocorticoids and intensified immunosuppressive therapy. In cases of chronic pancreatitis occurring in the context of SLE, limited evidence supports the use of induction therapy with prednisolone (20–60 mg/day), often in combination with other immunomodulatory agents such as CPA. However, the lack of high-quality randomized controlled trials (RCTs) underscores the need for further clinical research to inform evidence-based therapeutic guidelines. Further clinical studies are essential to establish clear and effective treatment strategies for both acute and chronic SLE-associated pancreatitis.10
Pancreatitis may present as the first manifestation of previously undiagnosed SLE or occur during the course of the disease. It is commonly associated with high disease activity, which increases the risk of severe outcomes. Patients experiencing severe disease flares are particularly vulnerable to developing fatal complications due to pancreatitis; therefore, appropriate therapeutic interventions are required. However, standardized guidelines regarding the type, dosage, and duration of corticosteroid therapy for SLE-associated pancreatitis are currently lacking, highlighting the need for further research in this area.
Lupus enteritis
Lupus enteritis is one of the most common specific GI manifestations of SLE. It may be either the first manifestation of the systemic disease or may develop concurrently with other symptoms.43 It may also arise because of suboptimal or inappropriate management of lupus.44 The pathophysiology of LE is not fully understood. It is suggested that deposition of immune complexes, as well as abnormal complement activation, leads to inflammation and microvascular damage, causing edema and thrombosis of intestinal blood vessels. Consequently, ischemia may lead to ulceration or even perforation.45 The symptoms accompanying LE are usually nonspecific. They include severe abdominal pain – most commonly diffuse, although some reports indicate that it may be localized – abdominal distention, diarrhea without blood or mucus, nausea, dry heaving, and vomiting.46 They present with varying degrees of severity, ranging from moderate to severe, and may be accompanied by symptoms involving other affected systems, such as joint pain, dysuria or anuria, and uterine bleeding.47 Physical examination may reveal sluggish or completely absent bowel sounds, as well as abdominal tenderness or muscle guarding. However, physical examination findings may also be completely normal.
Most often, LE affects the jejunum and ileum. It can also involve different parts of the colon and, very rarely, the rectum.48 Laboratory findings can be divided into nonspecific and lupus-associated abnormalities. The former include elevated CRP levels (ranging from low elevations to approx. 100 mg/L), erythrocyte sedimentation rate (ESR), and lactate dehydrogenase (LDH).49 The latter include positive ANA, anti-Ro, anti-Sm, anti-dsDNA, anti-La, and anti-U1 RNP antibodies. Decreased complement protein levels (C3 and C4) are also frequently observed.50 Blood morphology findings are nonspecific; however, low hemoglobin (Hb) levels are common, often due to blood loss, whereas white blood cell (WBC) counts may be either elevated or decreased.51
The gold standard imaging modality for diagnosis is abdominal CT. Possible findings include edema, thickening of the intestinal wall, and dilated intestinal loops.47 There are no pathognomonic signs of LE; however, 3 specific findings strongly raise suspicion of this disease when present together: the target sign (bowel wall thickening above 3 mm), the comb sign (engorgement of mesenteric vessels), and increased attenuation of mesenteric fat.47 Mild ascites is also frequently observed on CT. Pathological changes in the thorax, such as pleural effusion, may also be present.52 Other diagnostic methods include ultrasonography.53 Although it is easier to perform, its diagnostic accuracy is limited. In contrast, endoscopic procedures with biopsy, despite being more invasive, frequently demonstrate nonspecific inflammatory findings.54 First-line treatment of LE includes glucocorticosteroids, mainly high-dose intravenous methylprednisolone administered in pulses (200 mg, 300 mg, or 500 mg daily) for several days, followed by oral prednisone therapy. Most patients improve rapidly; however, treatment is often supplemented with 1 or 2 pulses of CPA and daily HCQ therapy. Mycophenolate mofetil is sometimes used and has demonstrated efficacy in certain cases.47, 55 Supportive treatment with intravenous fluids, antibiotics, or vitamin supplementation also plays a vital role due to impaired GI tract function.56 In more severe cases, this treatment may be insufficient. Biologic agents such as rituximab or belimumab are used in these situations, generally with favorable therapeutic outcomes.10, 52
Lupus-associated protein-losing enteropathy
Protein-losing enteropathy is a rare manifestation of SLE characterized by excessive protein loss through the GI tract.57 It leads to hypoproteinemia, hypoalbuminemia, and lymphopenia. Hypoalbuminemia may result in ascites, pleural effusion, pericardial effusion, and generalized edema.58, 59 In the pathogenesis of PLE, a key role is played by increased vascular permeability due to vessel damage caused by cytokine activity and complement deposition, as well as by vasculitis and intestinal lymphangiectasia.58
The early stage of PLE is frequently asymptomatic and difficult to detect. The most common symptom, with a prevalence of up to 89.7%, is peripheral edema. Among GI manifestations, the most frequent are abdominal distension, diarrhea, abdominal pain, and vomiting.60 Protein-losing enteropathy should be considered in patients with hypoalbuminemia in the absence of significant proteinuria or malnutrition and with positive ANA results. Relevant diagnostic tests include magnetic resonance (MR) lymphangiography, alpha-1-antitrypsin clearance, and technetium-99m human serum albumin scintigraphy (99mTc-HSA); however, in low- and middle-income countries, PLE is often diagnosed by exclusion.61 Technetium-99m human serum albumin scintigraphy is important because it can localize the site of protein leakage.62 Differential diagnoses include right-sided heart failure, inflammatory bowel disease (IBD), chronic liver diseases, renal conditions associated with significant proteinuria, malnutrition, malabsorption syndrome, amyloidosis, malignancies, nonsteroidal anti-inflammatory drug-induced enteropathy, and post-chemotherapy protein loss.58 The condition is treated with glucocorticoids and immunosuppressants such as CPA, mycophenolate mofetil, and cyclosporine A.60
Lupus mesenteric vasculitis
Mesenteric vasculitis is an uncommon GI complication of SLE that should be considered in patients presenting with abdominal pain. Lupus mesenteric vasculitis (LMV) is reported to affect between 0.2% and 9.7% of individuals with SLE, with a higher prevalence in Asia. It can be the initial manifestation of SLE and occurs more frequently in pediatric patients.63 The superior mesenteric artery is affected in 80–85% of cases, with the ileum and jejunum being more commonly involved than the large intestine and rectum. Patients with high disease activity are at a greater risk of developing LMV compared to those with inactive SLE.64 The pathogenesis of this condition is associated with the deposition of immune complexes in vessel walls, as well as thrombosis resulting from the presence of antiphospholipid antibodies.65 Case reports suggest that LMV may develop following GI infections; however, a definitive association has not been fully confirmed.63 The symptoms of LMV result from ischemia, which may progress to organ infarction. The most common clinical manifestations include abdominal pain, tenderness, and rectal bleeding, while nausea, vomiting, and diarrhea are also frequently reported.66, 67 Thrombotic occlusion typically leads to acute, sudden-onset abdominal pain, whereas chronic ischemia presents with postprandial pain and progressive weight loss. Urinary symptoms, such as lupus cystitis and dysuria, are associated with LMV in approx. 22.7% of cases.68
A prompt diagnosis is essential to prevent complications, but it remains highly challenging. The imaging modality of choice is contrast-enhanced CT of the abdomen, which is considered the gold standard.68 Typical radiological findings include bowel wall thickening, bowel loop dilation, intestinal wall enhancement known as the “target sign”, vascular occlusions, and ascites. Characteristic signs such as the “fence-like” pattern and the double halo sign may also be observed.69 The differential diagnosis should include infections, malignancies, adverse drug reactions, and atherosclerotic mesenteric ischemia. Management of the underlying disease is a key aspect of treatment.65 Anti-inflammatory and immunosuppressive therapy includes glucocorticoids, CPA, AZA, and mycophenolate mofetil.10 In SLE-related LMV, high-dose intravenous glucocorticosteroids are the first-line treatment,68 while CPA is reserved for refractory cases. Biologic agents, such as rituximab and tumor necrosis factor alpha (TNF-α) inhibitors, have also shown efficacy. Given the risk of perforation, surgical intervention, including segmental bowel resection, should be considered at an early stage.70
Mesenteric vascular thrombosis in SLE
Mesenteric vascular thrombosis is rare in SLE, and its frequency is difficult to determine due to the limited number of studies. The risk of thrombosis increases in the presence of concurrent vasculitis and antiphospholipid syndrome (APS).71 Antiphospholipid antibodies are present in approx. 20–40% of patients with SLE, and within 20 years, 50–70% of these individuals are likely to develop APS.72 Patients with SLE can develop both arterial and venous mesenteric thrombosis.73 This condition can lead to acute intestinal ischemia, necrosis, perforation, and hemorrhage. Clinically, it may present with acute abdominal pain and vomiting. Laboratory tests often reveal elevated WBC count, D-dimer, CRP, and lactic acid levels.74 Computed tomography findings may include bowel dilatation, bowel wall thickening, mesenteric edema, or vascular engorgement. Thrombi are often clearly visualized within mesenteric vessels on imaging.75 However, definitive diagnosis often requires exploratory laparotomy. Bowel segments affected by transmural infarction must be resected, and in some cases, a second-look laparotomy may be necessary.76 Current evidence suggests that anticoagulation should be the primary conservative treatment for mesenteric vein thrombosis, as it is associated with lower mortality, fewer complications, and improved outcomes compared to other therapies.77 Mesenteric thrombosis is a rare but potentially life-threatening cause of abdominal pain, with a mortality rate of up to 50% if left untreated.78
Drugs side effects
Gastrointestinal manifestations are common in patients with SLE, but most are related to adverse drug reactions and infections (Table 2).13 Glucocorticosteroids possess anti-inflammatory and immunosuppressive properties, which is why they are widely used in the treatment of autoimmune diseases such as SLE. Dexamethasone belongs to this group and has been associated with the occurrence of AP. Clinical cases have been reported in which AP developed after re-administration of dexamethasone.79 There is an increased risk of AP in patients receiving at least 1 of the following glucocorticosteroids: cortisol, dexamethasone, or prednisolone.80 Increasing the steroid dose may further elevate the risk of AP. Acute pancreatitis usually develops within 4–14 days after the initial exposure.
The mechanism by which AP occurs during glucocorticosteroid therapy remains unclear. However, it may be related to changes in lipid and calcium metabolism resulting from the systemic effects of corticosteroids. Another mechanism identified in animal studies suggests that corticosteroids may obstruct small pancreatic ducts, leading to increased viscosity of pancreatic secretions, which in turn causes pancreatic changes such as vacuolization of acinar cells, necrosis of peripancreatic fat, and hyperplasia of the islets of Langerhans.81
Hydroxychloroquine and, to a lesser extent, chloroquine (CQ) are commonly used in rheumatic autoimmune disorders (RADs), such as SLE. The most common side effects observed in RAD patients receiving HCQ or CQ are GI disturbances.82 These include decreased appetite, nausea, vomiting, diarrhea, bloating, and a burning retrosternal sensation. The most common adverse effect is GI upset, which may be severe enough to cause loss of appetite. It occurs more frequently with CQ (20%) than with HCQ (10%).83 These manifestations are usually transient and resolve over time or after dose reduction.83
Tacrolimus is a calcineurin inhibitor mainly metabolized by CYP3A. Ritonavir is a CYP3A and P-gp inhibitor, which may increase the plasma concentration of medications that are substrates of the CYP3A and P-gp enzymatic systems. Ritonavir is used in the treatment of HIV infection. For this reason, significant interactions between tacrolimus and nirmatrelvir/ritonavir have been reported. Blood tacrolimus concentrations increased above the therapeutic threshold in all patients. These patients presented with various symptoms, including nausea, vomiting, fatigue, weakness, loss of appetite, abdominal pain, slowed speech, and peripheral neuropathy, after taking nirmatrelvir/ritonavir without discontinuing tacrolimus.84
Leflunomide is an oral disease-modifying antirheumatic drug with anti-inflammatory and immunomodulatory properties.85 Many experimental models and clinical studies have shown that leflunomide has a beneficial effect in SLE.86 Common side effects of leflunomide include GI symptoms such as nausea, abdominal pain, and diarrhea, occurring in 10–20% of treated patients. More serious adverse effects, such as colitis, have also been reported. Leflunomide-induced colitis is a very rare adverse effect, with only a few cases described in the literature. The mechanism of this condition is not well understood. Diagnosis is challenging because symptoms may appear at different times, even several years after initiation of treatment. The median time to symptom relief following discontinuation of leflunomide was approx. 3 weeks, but ranged from 3 days to 7 weeks.87
Nonsteroidal anti-inflammatory drugs (NSAIDs) rank among the most frequently used medications worldwide. Evidence from certain studies indicates that the use of NSAIDs and aspirin among the elderly population reaches a prevalence of 24.7%.88 NSAIDs are commonly administered for the management of pain and discomfort associated with chronic rheumatologic conditions.89 According to data from 2 large cohort studies – ESTHER (n = 7,737) and the UK Biobank (n = 213,598) – low-dose aspirin administration independently contributes to an increased risk of developing gastric and duodenal ulcers during the early phase of treatment initiation.90 The risk ratios (RRs) for the development of gastric and duodenal ulcers were 1.82 [95% CI: 1.58–2.11] and 1.66 [1.36–2.04], respectively, in the UK Biobank study, and 2.83 [1.40–5.71] and 3.89 [1.46–10.42], respectively, in the ESTHER study. According to data from studies conducted in Spain, the mortality rate associated with NSAID use is 5.6%, corresponding to 15.3 deaths per 100,000 users.91 In the endoscopic picture, erosive and ulcerative lesions commonly occur in the gastric antrum; however, the pathological process may affect the entire gastroduodenal tract. These lesions may manifest in both acute and chronic forms, often presenting with bleeding and subepithelial hemorrhages on endoscopic examination. Ulcers typically heal without the formation of fibrotic scarring or structural deformities.88 Recent studies comparing the safety profile of celecoxib at a daily dose of 200 mg with other NSAIDs in the context of GI adverse effects have demonstrated that celecoxib exhibits a superior GI safety profile relative to other NSAIDs.92 Similarly, a previously conducted meta-analysis found that patients treated with meloxicam (a partially cyclooxygenase-2 (COX-2) selective agent) demonstrated a decreased occurrence of GI adverse effects, including dyspepsia, gastric and duodenal ulcers, and perforations. These findings suggest that COX-2 selective inhibitors are associated with a reduced risk of GI toxicity compared to nonselective NSAIDs. However, certain studies have demonstrated that GI symptoms during treatment with the nonselective NSAID naproxen were not indicative of mucosal injury. Although the risk of ulcer development correlates with the number of risk factors present, approx. 25% of patients without any classical risk factors still developed ulcers during high-dose NSAID therapy. These findings suggest that reliance solely on risk factor assessment is inadequate for determining the need for gastroprotection. A proactive preventive strategy is therefore recommended to ensure that all patients prescribed NSAIDs receive appropriate gastroprotective measures. Studies confirm that gastric and duodenal ulcers are common adverse effects associated with NSAID use, particularly among patients with rheumatologic conditions. Although NSAIDs are effective in the management of pain and inflammation, their use must be approached with caution because of GI risks, and appropriate preventive measures are required to reduce serious complications.
Azathioprine is a member of the immunosuppressive thiopurine group and is used to treat autoimmune diseases such as SLE. Retrospective data suggest that approx. 3.25% of patients treated with thiopurines experience AP, although clinical experience suggests that the incidence may be at least twice as high.93 The exact pathogenesis of AZA-induced AP is not yet known, but its idiosyncratic nature suggests an allergic mechanism. The association between AZA and AP appears to be dose-independent and does not correlate with myelosuppression, suggesting an etiology independent of thiopurine methyltransferase activity. A delayed type II or IV allergic reaction or an immunological genetic predisposition has been proposed, with the former hypothesis supported by the fact that rechallenge with AZA causes recurrence of symptoms.94 Azathioprine was one of 3 drugs in the study for which evidence of causing AP was demonstrated in RCTs.95 If a patient is admitted with a high clinical suspicion of drug-induced pancreatitis (DIP), AZA should be discontinued immediately while awaiting tests to exclude other common causes of pancreatitis.
Cyclophosphamide is widely prescribed for the treatment of autoimmune diseases such as SLE. Treatment regimens for patients with SLE often cause short-term toxicity manifested by GI symptoms (e.g., vomiting and diarrhea).96 Reported GI side effects include dose-related nausea, stomatitis, and a single case of hemorrhagic colitis. One report described a patient with colitis accompanied by fatal small bowel enteritis and pancolitis associated with 4 weeks of CPA therapy.97
Belimumab is a fully human recombinant IgG monoclonal antibody that targets and inhibits soluble B-lymphocyte stimulator (BLyS). Consequently, it induces apoptosis and downregulation of circulating B-cell clones. Studies have shown that patients with SLE have significantly higher BLyS levels than healthy controls. There have been some reports of AP associated with belimumab use. These cases were reported in women aged 40–49 years who had been receiving the drug for 1–2 years.87
Discussion
Systemic lupus erythematosus encompasses a wide array of GI manifestations that present significant diagnostic and therapeutic challenges. Our scoping review identified 11 distinct GI presentations, ranging from common, low-severity conditions such as GERD and oral ulcers to high-risk acute complications including LE, mesenteric vasculitis, and IPO. Although GERD and oral ulcers affect up to 1/3 of patients with SLE and are generally managed with proton pump inhibitors and antimalarials, delayed recognition of these symptoms as part of the lupus spectrum may prolong the time to definitive diagnosis and initiation of immunosuppressive therapy. Conversely, LE, mesenteric vasculitis, and IPO, while rarer, with prevalence ranging from 0.2% to 9.7%, carry risks of ischemia, perforation, and acute abdomen that require prompt contrast-enhanced CT imaging and aggressive treatment with high-dose intravenous corticosteroids, often supplemented with CPA pulses.
Between these extremes lie intermediate manifestations such as LH and pancreatitis, occurring in approx. 3–8% and 0.2–8.2% of patients, respectively. These conditions require careful differentiation from autoimmune overlap syndromes. Serological markers such as anti-ribosomal P antibodies, anti-LKM antibodies, and complement C1q deposits, alongside targeted histological evaluation, may help clinicians choose between intensified immunosuppression and conservative management.
A unifying pathophysiological mechanism underlies several of these GI manifestations: immune complex-mediated vascular injury. Deposition of antinuclear antibody complexes activates complement pathways, damages the endothelium, and promotes thrombosis, thereby contributing to mesenteric vasculitis, LE, IPO, and PLE. Recognition of this shared process emphasizes the importance of early and aggressive immunosuppressive intervention.
Despite advances in imaging techniques and treatment strategies, significant diagnostic and therapeutic gaps persist. Reliance on advanced CT imaging and histological confirmation limits rapid diagnosis in resource-constrained settings, and the absence of consensus diagnostic criteria for rare manifestations such as PLE or IPO contributes to underreporting and inconsistent management. Moreover, therapeutic protocols for many GI manifestations are mainly derived from case series and small cohort studies, with no standardized guidelines regarding the dosing, duration, or selection of immunosuppressive agents.
Adding further complexity, the immunosuppressants and supportive medications used to manage SLE carry their own GI risks. NSAIDs predispose even low-risk patients to peptic ulcers, corticosteroids may precipitate AP, and AZA poses an idiosyncratic risk of DIP These iatrogenic complications require vigilant pharmacovigilance, patient education, and proactive gastroprotective measures as integral components of SLE management.
Looking forward, future research must prioritize prospective, multicenter cohort studies to establish the true incidence, risk factors, and outcomes of GI manifestations of SLE. The development of noninvasive biomarkers, such as serum complement fragments or anti-endothelial antibodies, could improve early detection and monitoring, while AI-assisted imaging algorithms may enhance the identification of subtle vasculitic changes on CT and ultrasound. Finally, RCTs comparing specific immunosuppressive regimens for GI involvement are urgently needed to support the development of evidence-based standardized treatment protocols.
Limitations of the study
The heterogeneous nature of SLE makes it difficult to establish universal conclusions, since individual patient presentations can vary widely. Many of the referenced studies include small patient cohorts, which limits the generalizability of the findings and highlights the need for larger multicenter investigations. Additionally, the absence of standardized diagnostic criteria for certain GI manifestations complicates comparisons across studies, while the predominance of cross-sectional data leaves long-term disease progression and treatment efficacy insufficiently explored. Moreover, some treatment recommendations are based on case reports or small-scale studies rather than robust RCTs.
Conclusions
Gastrointestinal manifestations in SLE span a spectrum from mild, common symptoms to life-threatening acute complications. Early recognition of the shared mechanisms of immune complex-mediated vascular injury may facilitate timely and aggressive therapy. Standardized diagnostic criteria, accessible imaging, and consensus treatment protocols remain critical gaps. Addressing these issues through multicenter studies, biomarker development, and RCTs may improve outcomes and optimize care for patients with SLE and GI involvement.
Use of AI and AI-assisted technologies
Not applicable.