Abstract
Background. Closed locked intramedullary nailing (IMN) of femoral diaphyseal fractures (FDF) is the gold standard treatment. Postoperative frontal plane deformities can still occur following locked IMN.
Objectives. The primary aim of this study was to evaluate the effect of coronal plane deformities on knee joint function and overall functional outcomes in adults with FDF treated using static locked IMN.
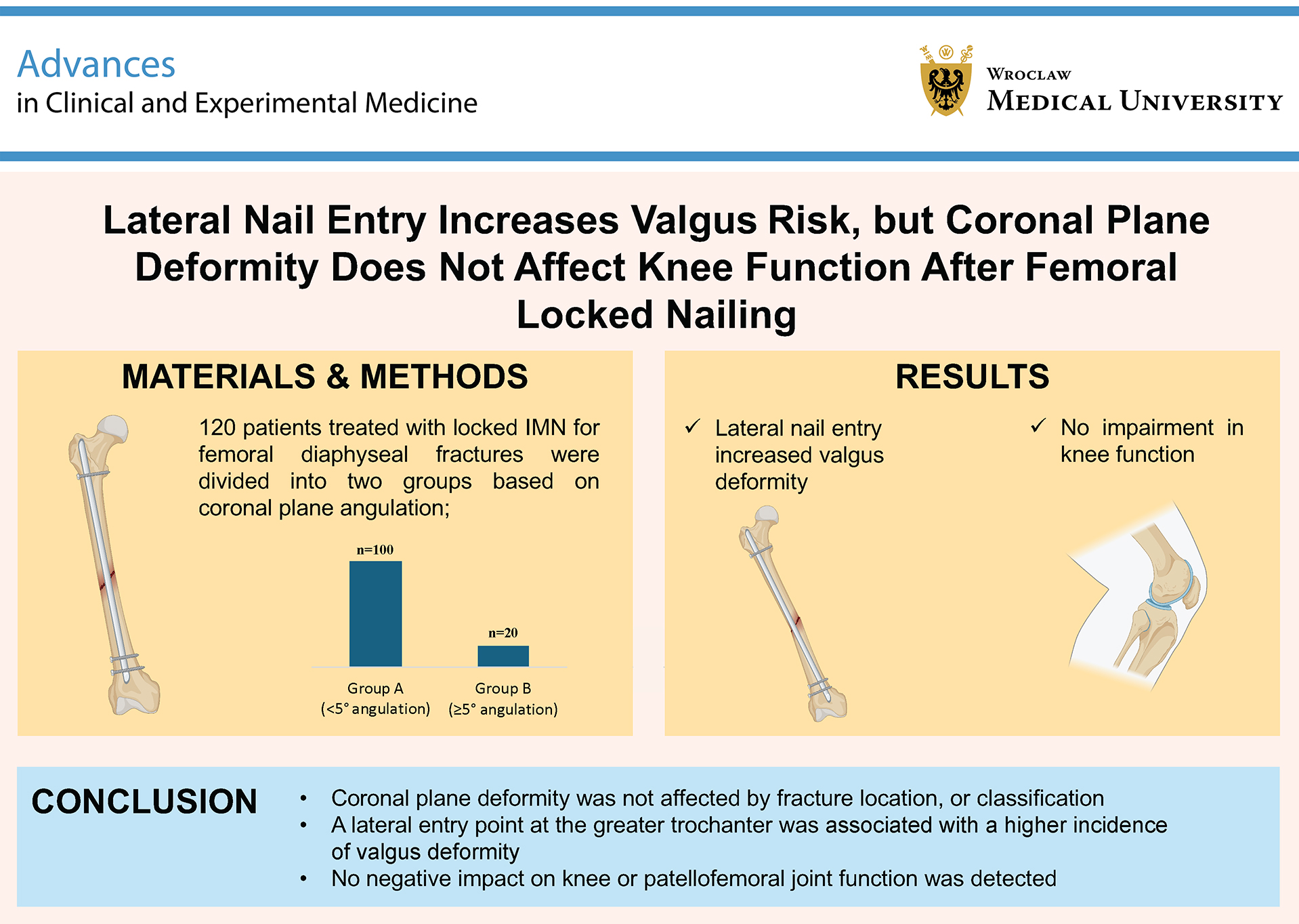
Materials and methods. One hundred and twenty patients treated with locked IMN for FDF were divided into 2 groups based on coronal plane angulation measured on long-leg radiographs: group A (<5° deformity, n = 100) and group B (≥5° deformity, n = 20). Factors potentially influencing coronal plane deformity were compared between the groups. Radiographic parameters, including the mechanical lateral distal femoral angle (mLDFA), mechanical medial proximal tibial angle (mMPTA), and postoperative lower extremity mechanical axis angle (MA), as well as intraoperative factors and complications, were analyzed. Functional outcomes were assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee score, the Lower Extremity Functional Scale, and the Kujala patellofemoral scoring system.
Results. There were no significant differences between the groups in terms of age, gender, AO classification, or mechanism of injury. Coronal plane deformity was found to be independent of fracture localization, fracture type, and use of a traction table. However, nails implanted laterally to the greater trochanter were associated with significantly more valgus deformity (p < 0.001). No significant differences were observed in postoperative mLDFA, mMPTA, or MA between the groups at the final follow-up. Functional scores also showed no significant differences.
Conclusions. After a minimum follow-up of 5 years, no adverse effects on knee or patellofemoral joint function were observed in patients with coronal plane deformities. Coronal plane deformity following locked IMN for FDF was independent of fracture location, classification, and traction table use. However, lateral entry to the greater trochanter was associated with increased valgus deformity.
Key words: femur diaphyseal fractures, intramedullary nailing, coronal plane malalignment
Background
The femur serves as the main weight-bearing bone of the lower extremity, and its fracture can lead to substantial morbidity and mortality. Femoral diaphyseal fractures (FDF) are common fractures in orthopedic practice, frequently seen in young male patients as a result of high-energy trauma, such as traffic accidents, falls from significant heights, or gunshot wounds.1, 2, 3 In this group of patients, transverse or oblique fractures are typically located in the middle third of the femoral shaft.1, 2, 3 These fractures display a bimodal distribution: They occur primarily in younger individuals due to high-energy trauma, while in elderly patients, they are more often the result of low-energy trauma.4 According to epidemiological studies, the annual incidence of diaphyseal femur fractures is estimated to be around 13 per 100,000 individuals.5
Currently, the preferred treatment for FDF is locked intramedullary nailing (IMN) with closed reduction, which is considered the gold standard due to its high union rates, facilitation of early mobilization and weight-bearing, and low complication rates.6, 7 From both biomechanical and clinical perspectives, this method is regarded as superior to extramedullary fixation with plates and external fixators. 6, 7 However, malalignment is a well-recognized complication in the literature that may lead to non-union and may require additional surgical intervention after locked IMN.8, 9
Malalignment can present as angular deformities (such as varus/valgus or flexion/extension) or rotational discrepancies. Postoperative coronal plane deformities following locked IMN are typically defined as frontal plane angulations exceeding 5°, which are generally classified as deformities. A literature review indicates that coronal malalignment is most commonly defined as an angular deformity of either “more than 5 degrees” or “5 degrees or more.”9, 10, 11, 12 Studies report that the incidence of such deformities above 5° ranges from 2% to 18%.9, 11, 13 While some studies in the literature have explored the impact of rotational deformities on patient functional outcomes following femoral IMN, there is a lack of research examining the effect of coronal deformities on functional status.
Objectives
To our knowledge, this study is the first to directly evaluate the impact of coronal plane malalignment on long-term functional outcomes, including knee and patellofemoral joint function, following locked intramedullary nailing of femoral diaphyseal fractures. The primary aim of this study was to evaluate the effect of coronal plane deformities on knee joint function and overall functional outcomes in adults with FDF treated using static locked IMN. A secondary aim was to identify the factors that contribute to the development of these coronal plane deformities. We hypothesized that coronal plane deformity negatively impacts knee function following femoral locked IMN.
Materials and methods
Study design and patient selection
This retrospective study included patients who underwent locked intramedullary nailing (IMN) for FDF in the Orthopedics and Traumatology Departments of 2 trauma centers. The study received approval from the Medical Research Ethics Committee of İzmir Bozyaka Training and Research Hospital (approval No. 2023/55), and general informed consent was obtained from each participant before the study procedures.
One hundred and twenty patients treated with locked IMN for FDF between February 2012 and February 2019 were included in the study. We excluded patients with open fractures, pathological fractures, additional lower extremity fractures, a history of knee surgery, those over 60 years of age, and those with a follow-up period of less than 5 years. Patients were divided into 2 groups based on coronal plane angulation measurements at the femoral fracture line obtained from orthoroentgenograms: group A, with an angulation of less than 5° (n = 100, 83.4%), and group B, with an angulation of 5° or greater (n = 20, 16.6%). Patient demographics, trauma mechanisms, follow-up duration, type of femoral nail used, and use of a traction table during surgery were obtained from medical records (Table 1).
Assessment of parameters between groups
Fracture localization and the Müller AO classification of fractures were assessed on preoperative femur radiographs. Three orthopedic surgeons independently reviewed and measured the preoperative and postoperative radiographic parameters. Fracture union was evaluated on anteroposterior and lateral femur radiographs obtained during follow-up. Sagittal plane angulations of the femur were assessed using lateral femur radiographs.
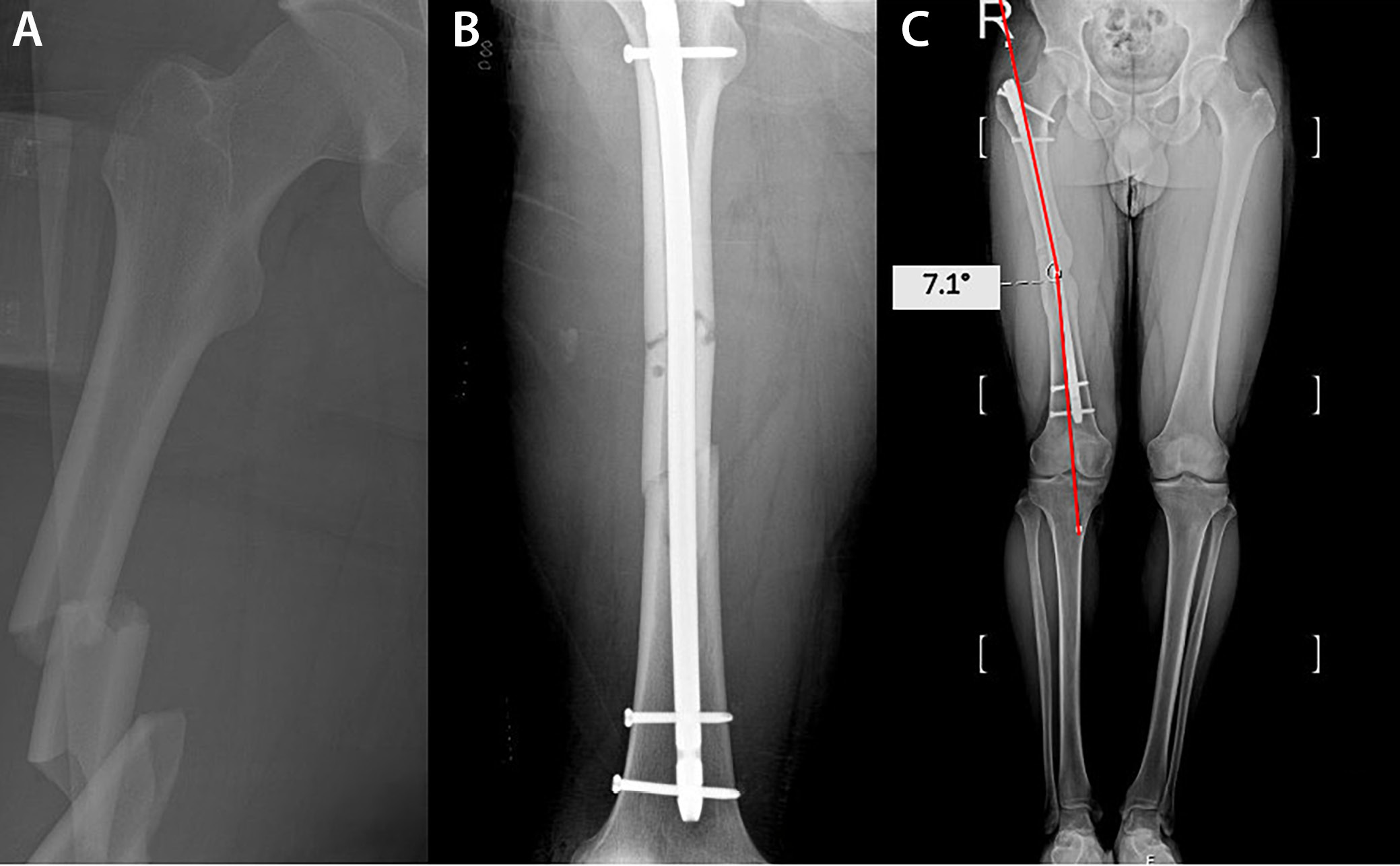
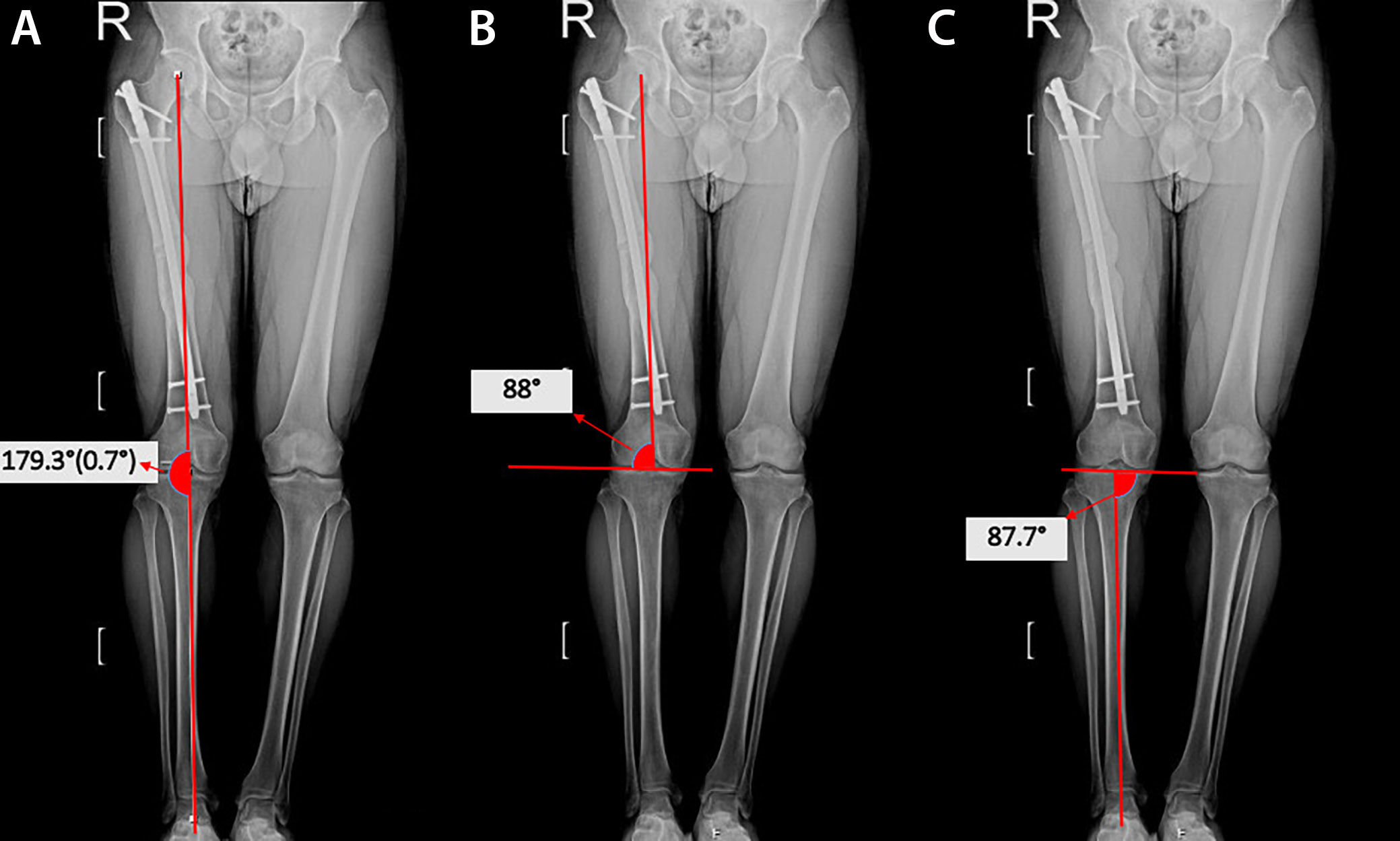
Orthoroentgenograms were used to assess femoral length discrepancies, coronal plane angulations (varus/valgus) at the fracture line, mechanical lateral distal femoral angle (mLDFA), mechanical medial proximal tibial angle (mMPTA), and postoperative lower extremity mechanical axis angle (MA), and to compare the sizes of the lesser trochanters on both sides to detect rotational deformity (Figure 1, Figure 2, Figure 3). Coronal plane deformity of the femur was evaluated by drawing one line from the fracture site to the proximal center of the medullary canal and another line from the fracture site to the midpoint of the distal femoral articular surface. The angle between these 2 lines was then measured (Figure 1C, Figure 2C).
Functional outcomes were evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) knee scores, the Lower Extremity Functional Scale, and the Kujala patellofemoral scoring system, and these outcomes were compared between the 2 groups.
Surgical technique
All surgical procedures were performed after patients were medically stabilized and appropriate radiological examinations and consultations were completed. Antegrade locked intramedullary nails were used for all patients. Procedures were conducted either on a traction table in the supine position or on a standard operating table in the lateral position. The insertion point for nail entry was selected based on individual anatomy, with entry sites including the greater trochanter, piriformis fossa, or the lateral aspect of the greater trochanter.
Statistical analyses
Continuous variables with a non-normal distribution are presented as medians and interquartile ranges (IQR; 1st quartile (Q1) and 3rd quartile (Q3) values reported), while categorical variables are presented as percentages. Normally distributed continuous variables are shown as means with standard deviations (SD). Categorical variables were compared between groups using Pearson’s χ2 test. The normality of continuous variables was assessed using the Shapiro–Wilk test, and the homogeneity of variances was evaluated using Levene’s test.
Comparisons of continuous variables between groups were performed using independent-samples t-tests for normally distributed data, and the Mann–Whitney U test was applied for non-normally distributed data. Interrater reliability was assessed using the intraclass correlation coefficient (ICC; 2-way mixed effects, absolute agreement, 3 raters) at each measurement point.
All statistical analyses were performed using IBM SPSS v. 23.0 (IBM Corp., Armonk, USA), with statistical significance set at p < 0.05.
Results
Patients were divided into 2 groups based on the coronal plane angle measurements of the femoral fracture line obtained from orthoroentgenograms: group A, with angulation less than 5° (n = 100, 83.4%), and group B, with angulation of 5° or more (n = 20, 16.6%). In group B, 6 patients (30%) exhibited varus deformity, while 14 patients (70%) displayed valgus deformity. The median coronal plane angle was 1.14° (Q1 = 0.5, Q3 = 2) in group A and 5.74° (Q1 = 5, Q3 = 6.2) in group B.
The median age was 28 years (Q1 = 21, Q3 = 39.25) in group A and 27 years (Q1 = 20, Q3 = 36.75) in group B, with no statistically significant difference (U = 1092, p = 0.519). The median body weight was 77 kg (Q1 = 73, Q3 = 79) in group A and 75.5 kg (Q1 = 73.5, Q3 = 78.25) in group B (U = 1138, p = 0.331). Similarly, the median body mass index (BMI) was 24.64 kg/m2 (Q1 = 23.71, Q3 = 25.58) in group A and 24.46 kg/m2 (Q1 = 23.23, Q3 = 25.89) in group B, showing no significant difference (U = 1007, p = 0.963). In terms of gender distribution, group A consisted of 19 women (19%) and 81 men (81%), whereas group B included 4 women (20%) and 16 men (80%), with no significant difference between groups (χ2 = 0.013, p = 0.918).
Regarding the mechanism of injury, motor vehicle accidents accounted for 73% of cases in group A and 85% in group B, while falls constituted 27% and 15%, respectively. Again, this difference was not statistically significant (χ2 = 1.263, p = 0.262). The median follow-up time was 78 months (Q1 = 69, Q3 = 90) in group A and 72 months (Q1 = 66, Q3 = 80.5) in group B (U = 1168, p = 0.238) (Table 1).
There was a satisfactory level of agreement among the 3 physicians who independently conducted radiological evaluations for all patients. The ICC values were 0.96, 0.95, and 0.92 for the CP angle; 0.94, 0.92, and 0.93 for mLDFA; 0.91, 0.94, and 0.95 for mMPTA; and 0.90, 0.95, and 0.91 for the MA angle, according to the measurement time points.
None of the 120 patients included in our study showed any signs of clinical rotational deformity. Radiologically, rotational deformity was assessed using orthoroentgenograms by comparing the sizes of the lesser trochanters on both sides. No discrepancies were observed in any patient. Postoperative sagittal plane deformities of the femur were assessed using lateral femur radiographs, and no deformities were identified in any patient.
The femoral diaphysis was divided into 3 equal segments, and fractures were categorized based on their location as proximal third (n = 19; 15.8%), middle third (n = 78; 65%), and distal third (n = 23; 19.2%) fractures. Coronal plane deformities ≥5° were found in 5.3% of proximal third, 17.9% of middle third, and 21.7% of distal third diaphyseal fractures. There were no significant differences between coronal plane deformities and fracture localization (χ2 = 2.297, p = 0.169) (Table 2).
Seventy-nine patients (65.8%) had AO 32-A, 31 patients (25.8%) had AO 32-B, and 10 patients (8.5%) had AO 32-C type fractures. Coronal plane deformities ≥5° were found in 17.7% of AO 32-A type fractures, 12.9% of AO 32-B type fractures, and 20% of AO 32-C type fractures. There were no significant differences between coronal plane deformities and fracture types (χ2 = 0.332, p = 0.758) (Table 2).
Intramedullary nails were placed through the greater trochanter in 37 patients (30.8%), through the piriformis fossa in 59 patients (49.2%), and laterally to the greater trochanter in 24 patients (20%). A coronal plane deformity ≥5° was observed in 2.7% of patients with intramedullary nails inserted through the greater trochanter, 50% of patients with nails inserted via lateral access to the greater trochanter, and 11.9% of patients with nails inserted through the piriformis fossa. It was determined that coronal plane deformity was more frequent in nails inserted from the lateral side of the greater trochanter. This difference was found to be significant (χ2 = 28.092, p < 0.001) (Table 2).
Ninety-one patients (75.8%) underwent surgery on a traction table, while the remaining 29 patients (24.2%) were operated on a standard operating table. Coronal plane deformities ≥5° were detected in 16 patients (17.6%) who were operated on a traction table and in 4 patients (13.8%) who were operated on a standard operating table. There were no significant differences between surgeries performed on a traction table and those performed on a standard operating table (χ2 = 0.369, p = 0.637) (Table 2).
The results of the radiological evaluations are shown in Table 3. There was no difference between the 2 groups in terms of mLDFA, mMPTA, and lower extremity MA angle measured at the last follow-up (t = 0.778, p = 0.415; t = 0.952, p = 0.350; and U = 1069, p = 0.627, respectively).
There was no significant difference between the groups in terms of the WOMAC knee score, the Lower Extremity Functional Scale, and the Kujala patellofemoral score (U = 737, p = 0.127; U = 1256, p = 0.061; and U = 1214, p = 0.067, respectively) (Table 4).
Discussion
The primary aim of this study was to evaluate the effect of coronal plane deformities on knee joint function and overall functional outcomes in adults with FDF treated using static locked IMN. A secondary aim was to identify the factors that contribute to the development of these coronal plane deformities. The results demonstrated that, although coronal plane deformities ≥5° were present in 16.6% of patients, they did not significantly affect functional outcomes, as measured using the WOMAC knee scores, the Lower Extremity Functional Scale, and the Kujala patellofemoral score.
The incidence of coronal plane deformities ≥5° in this study aligns with previous findings, in which deformities above 5° are reported in 2–18% of cases after locked IMN.9, 11, 13 Notably, we observed a significantly higher rate of coronal deformities when the nail was inserted laterally to the greater trochanter compared to other insertion points. This result suggests that the choice of nail insertion point may influence postoperative alignment, which could have implications for surgical planning.
Lateral entry points likely alter the trajectory of the nail, making precise alignment more challenging, especially in cases of complex fracture patterns resulting from high-energy trauma. Our findings are consistent with earlier reports suggesting a strong correlation between lateral insertion points and increased varus or valgus angulations.14 Sadagatullah et al. concluded that there was a higher rate of malalignment in proximal femoral shaft fractures treated with interlocking nails utilizing the greater trochanter entry point.15 Similarly, Ostrum et al. reported that a lateral starting point led to malalignment and gapping of the femoral cortex with all nails.16
Malalignment is a well-recognized complication in the literature that may lead to non-union and may require additional surgical intervention after locked IMN.8, 9 Malalignment can present as angular deformities (such as varus/valgus or flexion/extension) or rotational discrepancies. These deformities may negatively impact knee function following femoral locked IMN. To our knowledge, no previous study has examined the impact of coronal plane deformity on knee functional outcomes following femoral locked intramedullary nailing.
A review of the literature revealed a focus on rotational deformities following femoral locked intramedullary nailing, with studies examining their impact on knee and hip function.17, 18 Karaman et al. showed that femoral rotational malalignment ≥10° is symptomatic for patients and that the hip, knee, and patellofemoral joints are affected.17 Sharma et al. found worse WOMAC knee and lower extremity functional scores in patients with rotational deformity than in patients without.18 We found that despite the higher rate of coronal deformities with lateral insertion, functional outcomes were not significantly different between patients with and without deformity. We believe that minor angular deformities may not substantially impact functional performance, particularly in young, active individuals with greater compensatory abilities. However, it is worth noting that our study included a relatively young cohort with an average age of 31.7 years. Older patients or those with pre-existing knee pathology may experience greater functional limitations due to malalignment.
We hypothesized that coronal deformities are more commonly observed in fractures of the proximal and distal thirds of the femoral diaphysis. Khan et al. reported a significant association between proximal femur fractures and malalignment in their study involving 65 patients.10 Ricci et al. found that fractures in proximal and distal locations are correlated with increased fracture angulation.11 In our study, coronal deformities were detected in 5.3% of proximal, 17.9% of middle, and 21.7% of distal diaphyseal fractures. In contrast to our initial hypothesis, our study found no statistically significant association between coronal deformities and fracture localization (p = 0.169).
We anticipated that progression from AO type A to type C would involve more complex and fragmented fractures, making coronal alignment more challenging to control. Ricci et al. showed that an unstable fracture pattern is associated with increased fracture angulation.11 In our study, coronal deformities were identified in 17.7%, 12.9%, and 20% of patients with AO type A, B, and C fractures, respectively. Contrary to our initial hypothesis, our study revealed no statistically significant association between coronal deformities and fracture type (p = 0.758).
Regarding the operative setup, the use of a traction table versus a standard operating table did not significantly impact the incidence of coronal plane deformity. He et al. concluded that, compared with manual traction, the traction table in femoral intramedullary nailing surgery lengthens operative time and preoperative setup time. At the same time, it does not show significant advantages in reducing blood loss volume, fluoroscopy time, or improving prognosis.19
Similarly, Sholla et al. found that the lateral decubitus method without a traction table was a safe and effective alternative to the supine method with a traction table in terms of radiological and clinical results.20 While a traction table is often preferred for better control of fracture reduction, our results suggest that it may not necessarily result in superior coronal alignment. This finding may inform surgical teams that, under certain conditions, a standard operating table may be a viable alternative, especially in facilities without access to traction tables.
Radiographically, there were no significant differences between the groups in terms of mLDFA, mMPTA, or lower extremity mechanical alignment. This outcome highlights that minor deviations in coronal alignment at the fracture site may not translate into large-scale mechanical axis alterations, at least in the short to medium term. This finding may explain why coronal plane deformity does not negatively impact knee function, at least within a 5-year follow-up period. Long-term studies are warranted to evaluate whether these deformities contribute to early degenerative changes, especially in high-functioning individuals.
Limitations of the study
The retrospective nature of this study limits the generalizability of our findings. Future research with a prospective design, larger sample sizes, and longer follow-up periods could provide more insight into the long-term effects of coronal deformities on joint function. An additional limitation of our study is the large difference in the number of patients between the groups. Another limitation was that we could not determine a cut-off point for coronal varus deformity. A key limitation in establishing a definitive “cut-off” for acceptable coronal plane deformity lies in the ethical and clinical need to correct severe malalignments. For instance, high degrees of coronal plane deformity would not be ethically feasible to include in a study or to leave unaddressed in clinical practice. Severe deformities are typically corrected intraoperatively, as leaving a patient with such a misalignment would constitute a deviation from standard care and could lead to legal and medical implications. Consequently, the absence of patients with extreme deformities in our study reflects routine corrective practices rather than a defined clinical threshold for acceptable alignment. This limitation underscores the importance of standardized guidelines and surgical expertise in preventing significant malalignment. Future biomechanical studies could further explore the impact of major coronal plane deformities. Another limitation of our study is that, because the patients were trauma cases with femoral fractures, preoperative evaluation of limb alignment parameters could not be performed. Therefore, it was not possible to compare preoperative measurements with postoperative measurements.
Conclusions
No negative outcomes were detected in the knee or patellofemoral joints of patients with coronal plane deformities after at least a 5-year follow-up. Coronal plane deformity was found to be independent of fracture localization, fracture classification, and whether the fracture was operated on using a traction table. Increased valgus deformity was observed in nails inserted from the lateral aspect of the greater trochanter.
Data Availability Statement
Data sharing does not apply to this article, as all data are already included in the manuscript.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.
.jpg)