
















Abstract
Three-dimensional bioprinting technology appears to be a promising solution for the treatment and reconstruction of a wide range of maxillofacial bone defects. In this review, the authors discuss different bioprinting solutions and options in the context of the 4 factors of bone healing: structures or scaffolds, osteogenic cells, growth factors, and stabilization (diamond concept of healing), as well as the influence of a 5th factor – vascularization. Bone is a complex tissue; hence, bone bioprinting may require different technical approaches and mixed methods. Ultraviolet (UV) crosslinkable hydrogels, such as gelatin methacryloyl (GelMA), are among the most promising bioinks; they are enhanced by hydroxyapatite or 1–2.5 mm beta-tricalcium phosphate (β-TCP) granules and porous scaffolds with recommended pore sizes greater than 300 µm. The advantages of mesenchymal stem cells (MSCs) are their significant availability, low tumorigenicity, and great potential for differentiation into osteoblasts or endothelial cells (ECs). Although growth factors require advanced delivery systems, they provide excellent improvement in the functionality of printed tissues. A proper vasculature system supplies cells with oxygen and nutrients, removes waste products, promotes osteogenesis, prevents ischemic necrosis, and improves the mechanical properties of bone. With all of these aspects perfectly balanced and working in synergy, the clinical use of bioprinting is only a matter of time.
Key words: bioprinting, augmentation, tissue engineering, regenerative dentistry, regenerative medicine
Introduction
Three-dimensional (3D) printing has long been used in efforts to not only achieve bone regeneration but also restore lost dentition. Computer-aided design and computer-aided manufacturing (CAD/CAM)-produced titanium mesh can be used for guided bone regeneration procedures, allowing for more predictable outcomes.1, 2 Furthermore, 3D technology can be used to manufacture custom-made, precisely fitting scaffolds out of porous hydroxyapatite blocks.3 Titanium dental implants created through the process of direct laser metal forming, a particular method of additive manufacturing, have already proven to be predictable. Moreover, although their properties still need to be confirmed, they could potentially surpass conventional, machined dental implants in many ways.4, 5, 6, 7, 8, 9, 10
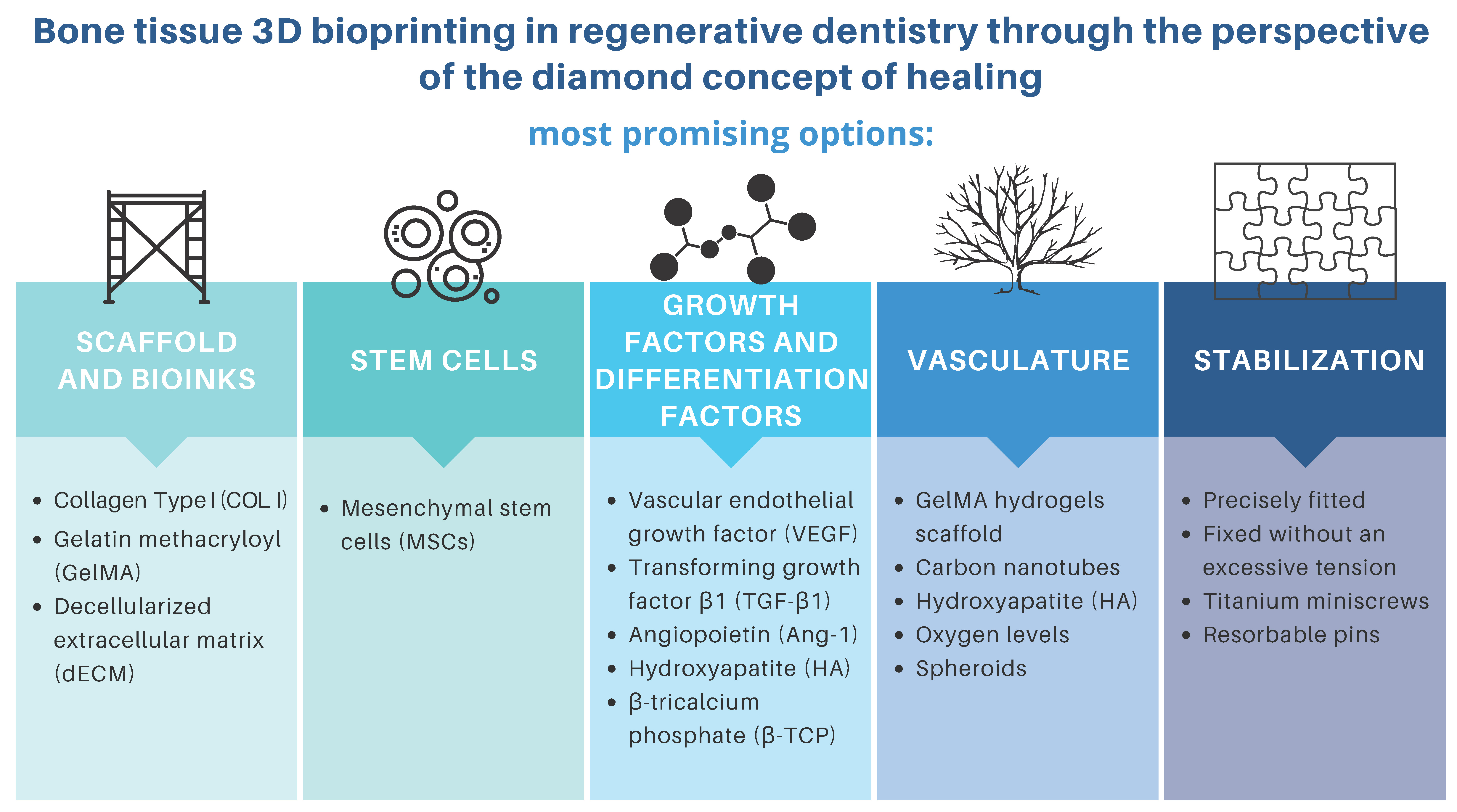
Since its inception over a decade ago, the “diamond concept”, a conceptual framework of what is necessary to achieve successful bone healing, has been acknowledged. This framework includes the following: 1) sufficient mechanical stabilization and biological competence of the organism; 2) osteogenic cells; 3) osteoconductive structures or scaffolds; and 4) growth factors.11, 12 Additionally, sufficient vascularization of newly formed tissue should be considered a 5th element required for successful bone regeneration (Figure 1).
Autogenous grafts are considered the “gold standard” in bone tissue regeneration due to their osteogenic, osteoconductive and osteoinductive properties.13 Unfortunately, harvesting autogenous bone grafts usually causes pain at the donor site. It may also result in other, less frequently encountered complications, including nerve injury, hematoma, infection, and damage to neighboring tissues.14 An emerging solution to this problem is 3D bioprinting technology, which has the ability to create living autogenous grafts that are designed and manufactured in adequate form and dimensions to perfectly fit the shape of the defect. The creation of 3D tissue constructs is achievable using bioink deposition (specifically, jetting, extrusion or laser-assisted evaporation) and then crosslinking with a 3D bioprinter. This technology facilitates the design of complex constructs – individualized forms and shapes of the target tissue structure that simultaneously contain multiple cell types.15
Objectives
The available scientific literature is relatively lacking in original studies and review articles on the use of bioprinting in dental procedures. Nevertheless, knowledge of this topic is important to refine the practice and development of this technology. This review aims to summarize the current state of knowledge on contemporary bioprinting treatment in dentistry. Current regenerative practices and studies in the field of regenerative dentistry are also discussed.
Methods
An electronic database search was conducted using MEDLINE via PubMed and Google Scholar. The database was searched for in vitro and in vivo studies involving different approaches to certain topics (i.e., types of cells, bioinks, growth factors, and answers to vascularization needs). The especially valued studies were those that contradicted or proved the limitations of factors and methods used in previous studies.
The search terms included all combinations of the following keywords: bioprinting OR 3D bioprinting OR stem cells OR mesenchymal stem cells OR growth factors OR GelMA AND bone regeneration OR bone OR clinical use OR regenerative medicine OR regenerative dentistry. Since 3D bioprinting refers to a variety of scientific fields, the following exclusion criteria were applied: 1) 3D printing not related to medicine; 2) 3D printing of medical materials; 3) studies related to hard tissues other than bone; 4) studies on bone regenerated with different techniques; and 5) other 3D applications in medicine.
Two researchers (KO and MC) independently reviewed the titles and abstracts to determine whether they met the inclusion and exclusion criteria. Disagreements were resolved via consensus. Collected titles and corresponding abstracts without duplicates were imported into Sciwheel citation manager program (Sciwheel Ltd., London, UK). The reference lists of the imported articles were screened for other relevant studies (Figure 2). In turn, the collected studies were screened to search for bias in article selection. They were then grouped into the following 5 categories depending on the type of experiment conducted: 1) scaffold and bioinks; 2) stem cells; 3) growth factors and differentiation factors; 4) vasculature; and 5) stabilization. Although some studies addressed 2 or more categories, the authors tried to cite the results in such a way that the main points and significance of the results could be easily understood. Sometimes, one study was mentioned multiple times, as it pointed to various findings.
Scaffolds and bioinks
Bioprinting offers the possibility of printing cell suspensions into a tissue construct, regardless of the presence of a scaffold support. The most common bioinks are cell-laden hydrogels, decellularized extracellular matrix (dECM)-based solutions and cell suspensions.16 When choosing a suitable bioink, certain technical aspects must be considered, as it should: 1) provide chemical conditions mimicking those of the targeted tissue; 2) be biocompatible; 3) have controlled biodegradability to allow for cellular remodeling; 4) present shear-thinning behavior that allows extrusion with minimal stress to the encapsulated cells; 5) enable sol–gel transition; 6) be able to be extruded without clogging the nozzle; 7) provide suitable durability and stiffness; 8) provide adequate shape fidelity with proper stacking ability; and 9) feature proper density and porosity for the diffusion of gasses and nutrients.17 No perfect, flawless bioink exists; the compromise between suitability for fabrication and ability to accommodate encapsulated cells should be established. This compromise is known as the “biofabrication window”.18 Bioprinting of bone requires the use of bioinks with the ability to transform from a liquid state to a more dense structure while simultaneously preserving cell viability and bioactivity.19 Moreover, the density of the newly formed construct has an impact not only on the durability of the scaffold itself but also directly influences the activity of the cells.20 Precalcified bone with a maximum stiffness of approx. 50 kPa is the most rigid matrix that can host stem cells,21 which is still over 10,000 times less rigid than mature calcified bone.22 Bone marrow mesenchymal stem cells (MSCs) are the softest stem cell niche,23 with a nearly liquid extracellular space and elasticity of 0.3 kPa.20 Such a difference may be overcome in vitro, but it presents a challenge for in vivo experiments. A promising solution seems to be integrating different technical approaches for different bone compartments (i.e., scaffold-based and non-scaffolding methods).15
The biomaterials currently used in 3D bioprinting can be assigned to one of 3 main categories: 1) non-hygroscopic polymers; 2) hydrogels; and 3) dECM.19
Curable polymers comprise the 1st category; they display good durability and mechanical properties suitable for adequate structure and scaffolding. Processing of this kind of material, however, requires extraordinary conditions, including high temperature or the presence of toxic solvents, which mostly excludes them from being printed collectively with cells. Therefore, these materials are usually used for scaffold production, with cells seeded upon the surface.24
The 2nd category consists of hydrogels, i.e., soft biomaterials that can absorb and maintain large loads of water.25 These can be made of synthetic or natural polymers and do not present the same levels of mechanical features as curable support polymers, although cells are capable of residing within them.24 Synthetic hydrogels include polyethylene glycol (PEG)-based materials, such as PEG diacrylate, and polyacrylamide-based gels. Naturally derived hydrogels, which employ polymers, are often polysaccharides obtained and purified from natural sources. Additionally, they can be composed of peptides or proteins. Hydrogels commonly used in laboratories include collagen, hyaluronic acid, alginate, agarose, chitosan, fibrin, and Matrigel.19, 24
As the majority of bone tissue’s extracellular matrix (ECM) (approx. 95%) consists of collagen (COL) type I,26 and since collagen is one of the most widely available bioinks, it might seem to be a logical initial choice from the viewpoint of bone bioprinting.27 Although not ideal, COL has the qualities to be a potential bioprinting material. It has a variety of different characteristics, including being liquid at low temperatures; when faced with an increase in temperature or neutral pH, it creates a fibrous structure.25 As a consequence of losing its typical, organized structure, COL becomes gelatin (denatured COL).28
Gelatin, being the degraded form of collagen, contains many arginine–glycine–aspartic acid sequences, which display cell-responsive properties,29 as well as the target sequences of matrix metalloproteinases (MMPs) responsible for tissue and cell remodeling.30 Pore sizes greater than 300 µm are recommended, as they enhance the formation of bone tissue and capillaries. Larger pores are better vascularized and cause immediate osteogenesis, without the preceding formation of cartilage. Smaller pores, on the other hand, tend to cause hypoxic conditions and favor osteochondral formation. In addition, gelatin is easily soluble and less antigenous than collagen.31
Gelatin methacryloyl (GelMA) is a synthetically modified gelatin-based material containing methacrylamide groups and methacrylate groups.32 Most importantly, GelMA is an inexpensive, cell-responsive hydrogel utilized to create cell-laden microtissues and microfluidic devices. Synthetically derived hydrogels have the advantage of allowing easy modification of their mechanical features and having cell-adhesive properties.33 Gelatin methacryloyl hydrogels could be useful for creating complex, cell-responsive microtissues with endothelialized microvasculature. They have been patterned down to 100 μm resolution and proven to have accuracy and functionality similar to other commonly used hydrogels. However, unlike other synthetic ultraviolet (UV) crosslinkable hydrogels, they have been shown to have cell-adhesive properties; cells adhere to them, migrate within them, proliferate, and organize in both 2D and 3D in GelMA micropatterns. These data suggest possible applications in creating endothelial-lined vasculature within engineered tissues.33
Conveniently, methacryloyl substituent groups provide gelatin with the ability to photo-cross-link when exposed to light and a photoinitiator.34 This process of polymerization does not require extraordinary conditions and allows a certain level of control over the reaction. For this reason, the photo-curing properties of hydrogels are considered a significant upgrade compared to other common materials. Gao et al. created a particular bioink composed of GelMA hydrogel cross-linked with PEG-gelatin and MSCs incorporated within its structure as a way to obtain mechanical properties ideal for creating bone and cartilage.35 After 21 days, different types of constructs were compared: human MSC-PEG-GelMA and cell-laden PEG or GelMA. The first type demonstrated an elastic modulus improvement of 100% compared to the others. The authors proved that multimaterial hydrogels with photo-cross-linking features may introduce new solutions and promising advances in the composition of bioinks, in particular in the context of producing cartilage and bone substitutes.19 Additionally, GelMA has already been used in several studies on printing functioning vascular networks and bone-tissue substitutes, which will be discussed later in this article.36, 37, 38
The 3rd category of biomaterials is dECM, which has the native ECM components retained. Its premanufacturing requires all cells to be removed from a tissue while preserving only the ECM. This is achieved through a series of chemical and enzymatic processes.39 The dECM is then solubilized to a desired concentration until a gel-like substance appropriate for 3D bioprinting is obtained.19 Once isolated, bone dECM can be co-printed with biocompatible hydrogels or molecules.40, 41, 42 Moreover, in order to promote osteogenesis, small particles of hydroxyapatite or beta-tricalcium phosphate (β-TCP) can be dispersed in the hydrogel-based bioink.43
Factors such as the macrostructural and geometrical properties of a material have a major impact on more than just the resilience of a scaffold. Studies have shown that materials characterized by numerous pores of variable sizes and connectivities facilitate the passage of oxygen, nutrients and cellular wastes.19 As porosity promotes the oxygenation of MSCs in printed hydrogel scaffolds, it also supports their viability and osteogenic differentiation.44 Lower porosity has been shown to suppress cell proliferation and force cell aggregation in vitro, thus stimulating osteogenesis. On the contrary, significantly greater ingrowth of bone tissue can be achieved in vivo, thanks to larger pore size and higher porosity. However, the increased size and number of pores results in worsened mechanical properties. This fact sets an upper limit to pore size and porosity.45 Pore sizes greater than 300 µm are recommended, as they enhance the formation of bone tissue and capillaries. Larger pores are better vascularized and cause immediate osteogenesis, without the preceding cartilage formation. Smaller pores, on the other hand, tend to cause hypoxic conditions and favor osteochondral formation.45 A study by Lee et al. compared porosity of and cell cultures on 3 different scaffolds: COL, COL/dECM (CE) and COL/dECM/silk fibroin (CES). After 7 days, scanning electron microscope (SEM) images showed the highest concentration of cells on CES, followed by a medium concentration on CE and comparatively the lowest concentration on pure COL. Furthermore, the researchers analyzed the pore aspect ratio (length/width), and almost 100% of CES pores had a ratio of less than 3. In the case of CE, approx. 70% of pores had a ratio lower than 3, 20% had a ratio of 3–6 and 10% had a ratio greater than 6. The majority of pure COL pores had a ratio of 3–6. In light of these data, it seems that longer and narrower pores provide inferior conditions for cell cultures compared to more proportional ones.42
Stem cells
Stem cells have major advantages over adult cells (i.e., self-renewing potential and ability to differentiate when exposed to specific stimuli).46 Tissue engineering and regenerative medicine need to embrace these abilities to fulfill the following tasks: such as: 1) providing architectural and hierarchical arrangement of the cell–biomaterial complex; 2) patterning living cells in 3D; and 3) mimicking the complex patterns of tissue organization.47 Before selecting stem cells for a bioprinted model, their experimental and therapeutic boundaries, origin, immunocompetence, and long-term engraftment potential dictated by the potency of the cell must be taken into consideration.48
Three major classes of stem cells can be distinguished: 1) induced pluripotent stem cells (iPSCs), which can be reprogrammed from somatic cells isolated from the patient’s tissue with ease of access; 2) embryonic stem cells (ESCs), which originate from the inner cell mass of blastocysts and have the potential to differentiate into any cell type; and 3) adult stem cells, which are located in specific tissues and take an active role in repair processes.47
The initial creation of iPSCs was accomplished through the ectopic expression of 4 specific genes (OCT4, KLF4, SOX2, and c-Myc; all 4 are abbreviated as OSKM). Thus far, iPSCs have been successfully acquired from a variety of different cell types and species, suggesting a universal molecular mechanism. The abundance of sources of iPSCs in contrast to other pluripotent stem cell sources may suggest their forthcoming usefulness in the development of tissues and organs.49 Moreover, autologous iPSCs provide cells considered the least dangerous in terms of the risk of immune rejection. However, in research into age-related macular degeneration therapy, 2 major drawbacks were encountered: financial limitations and the duration of treatment. The process of generating iPSCs, confirming their safety and differentiating them into retinal cells used for transplantation took approx. 1 year and cost almost 1 million USD.49
In the 2nd group are ESCs, which provide extraordinary proliferative potential and are directly responsible for the formation and growth of the embryo and the 3 different germ layers – ectoderm, endoderm and mesoderm – which are essentially employed in the formation and generation of any type of tissue.47 There has been extensive research on utilizing ESCs to achieve regeneration of bone tissue. However, due to the risk of immune rejection and existing ethical issues, the application of ESCs under nonlethal orthopedic conditions is considerably limited.50 Furthermore, ESCs isolated from mice and then later from humans featured not only pluripotency but also tumorigenicity.51 In the context of regenerative medicine, the extent of their application for printing tissue constructs is largely limited by their low approachability, questionable safety and ethical issues.52
Unlike ESCs, MSCs have the advantage of being available throughout the entire life of an individual and at all stages of development, including adulthood. Moreover, they may also be obtained as a result of differentiation of other types of stem cells (iPSCs and ESCs).53 A meta-analysis by Wang et al. showed that tumorigenesis, which might potentially occur in MSC therapy, has rarely been reported.54 The MSCs constitute a class of cells displaying significant heterogeneity and the possibility to be isolated from many different sites, including adipose tissue, the umbilical cord and the placenta,54 as well as from bone marrow in the form of an aspirate.45 One of the natural pathways for the development of MSCs is differentiation into osteoblasts, although this requires key differentiation factors, such as ascorbic acid, β-glycerophosphate, dexamethasone/vitamin D3, and galectins. This process results in the expression of certain markers, including an increase in alkaline phosphatase, calcium accumulation and RUNX2.53 However, research on the potential of MSCs in scaffold models should concentrate not only on osteogenic capabilities, as they can actually play 2 different roles. The first and most obvious role is as a source of a specific type of cell, which in this case means subsequent differentiation into osteoblasts. An alternative role of MSCs is as a supplemental population of cells, either as a native population or as an additional population that can be recruited to the tissue in order to perform a different function. In osteochondral constructs within the same model, MSCs are meant to differentiate into bone lineages and cartilage.53 Cidonio et al. highlighted that the patterning of endothelial cells (ECs) and using MSCs for printing are crucial for the proper functioning of engineered bone tissue, while new clinical solutions targeting bone defects may fail due to poor interconnection between the graft and host tissues and possible necrosis of the graft caused by insufficient nutrient supplies.55 An in vitro study by Wang et al. demonstrated successful MSC differentiation into ECs. Factors such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, insulin-like growth factor (IGF), epidermal growth factor, ascorbic acid, and heparin were used to impact MSCs. In addition, real-time quantitative polymerase chain reaction (qPCR) showed elevated expression of certain indicators, such as vascular endothelial cadherin, von Willebrand factor and VEGF receptor-2, in an induced MSC group compared with an uninduced MSC group.56 The ability of MSCs to create vasculature was examined in a recent in vivo study of canines by producing small artificial vessels. The researchers employed autologous MSCs of bone marrow origin and biodegradable polycaprolactone (PCL). After MSC culturing and confirmation of differentiation into endothelial-like cells, 3-layered artificial vessels were created and subsequently implanted into the arteries of the canines. In comparison to the control vessels, the cell-derived vessels showed that their inner surfaces were covered with more ECs, whereas fibrinous clots exhibited little to even no inflammation. The authors of that study suggested that the immune system only minimally rejected these artificial vessels due to the autologous origin of the MSCs.57
Although the presented studies depict MSCs as currently the best candidate for tissue engineering and regenerative medicine, there are always drawbacks. In this case, more research needs to be conducted on the exact mechanism of differentiation into other cell types, as this process remains unknown.53
Growth and differentiation factors
Growth factors are endogenous signaling molecules that regulate the cellular responses required for wound healing processes, including migration, proliferation and differentiation.58, 59
These signaling molecules can be divided into 3 groups: 1) pro-inflammatory cytokines; 2) transforming growth factor beta (TGF-β) superfamily and other growth factors; and 3) metalloproteinases and angiogenic factors.60
All of these molecules, including the interleukins (IL-1 and IL-6), tumor necrosis factor alpha (TNF-α), fibroblast growth factor, IGF, platelet-derived growth factor, and VEGF, are naturally found in abundant quantities in a fracture hematoma. These biologically active molecules are secreted not only by a variety of cell types, including ECs, platelets, macrophages, and monocytes, but also MSCs. Bone morphogenetic proteins (BMPs) are well-known signaling molecules that possess osteoinductive properties.12 Bone morphogenetic protein 2 and BMP-7 are already approved for clinical use in orthopedic and trauma surgery.61 Additionally, the activity of BMPs and other proteins that triggers cell differentiation into osteoblasts, which in turn results in bone formation, is also affected by the micro- and nanostructural properties of the scaffold used.62
Vascular endothelial growth factor is known to be a key regulator of physiological angiogenesis during embryogenesis.63 This makes it one of the best examined growth factors in regard to this topic. In fact, a different approach to promoting vascularization is to enrich 3D constructs with growth factors, thus causing the fabrication of a vascular network in tissue-engineered bone.64 Unfortunately, growth factors display very low in vivo stability, which significantly reduces their effectiveness in clinical settings.58 The effective use of growth factors is highly dependent on available delivery systems. Some researchers have targeted this aspect of therapy with novel delivery platforms, such as polymer gels, coated dressings, chamber devices, and nanoparticles.65, 66
Gelatin microparticles have been tested as a way of controlling the release of VEGF so that it is active for a longer period of time at a specific part of the 3D-bioprinted scaffold. Gelatin microparticles enabled the prolonged release of VEGF during 3 weeks of in vitro studies. Perhaps more importantly, with the help of human endothelial progenitor cells, the bioactivity of VEGF was successfully confirmed. Moreover, in vivo experiments on mice compared Matrigel scaffolds containing endothelial progenitor cells and VEGF that were released in one of 2 ways – fast or sustained – through the application of gelatin microparticles. The results after 7 days showed significantly higher levels of vessel formation in the sustained-release VEGF group compared to the fast-release VEGF group.67 A study by Kim et al. tested the chitosan gel/gelatin microsphere dual delivery system as a method of enhancing osteoblast differentiation through the sequential release of 2 osteogenetically important molecules – BMP-2 and IGF-1. In their research, BMP-2 was released at the beginning, with a succeeding sustained slow release of IGF-1. Significantly higher alkaline phosphatase activity, which is usually associated with ongoing osteoblast activity, was observed among cells that received the sequential delivery system when compared with cells that underwent other treatment methods (p < 0.05).68
A study by Jeon et al. examined the effect of transforming growth factor beta 1 (TGF-β1) and angiopoietin (Ang-1) on human bone marrow-derived MSCs, both in monoculture and in direct contact with ECs. They demonstrated that the effect of these molecules is dependent on direct heterotypic cell–cell contact. Furthermore, they found a significant increase in the amount of α-smooth muscle actin in microvascular networks with added VEGF and TGF-β1 or VEGF and Ang-1 compared to networks with added VEGF alone. The addition of Ang-1 resulted in the creation of fully functional networks, while the microvasculature initiated by TGF-β1 lacked interconnections and thus was not satisfactory. The addition of Ang-1 to human bone marrow-derived MSCs caused an increase in the number of network branches and a reduction in mean vessel diameter compared to EC-only vasculature.69 In conclusion, more actin-rich networks originated with VEGF + TGF-β1 or VEGF + Ang-1 compared to VEGF alone; in particular, Ang-1 developed more complex networks than TGF-β1.
Platelet-rich fibrin, with its advantage of being of autologous origin, does not face the legal problems of its predecessors and has been applied for a variety of different surgical indications.70
A recent study by Lafiti et al. showed that platelet rich plasma/heparin sulfate (PRP/HS) improved adipose MSC differentiation and accelerated osteoblast differentiation, regardless of the presence of an osteogenic medium. Moreover, HS has a positive effect on the induction of osteoblast differentiation. Hydroxyapatite, PRP and HS showed synergistic effects on the formation of a 3D scaffold, especially in the presence of chemical induction. The ZrO2 increased mechanical strength without any detrimental effects on bone formation. All things considered, it seems that hydroxyapatite/ZrO2/PRP/HS scaffolds provide a better osteoconductive microenvironment for stem cells to differentiate into osteoblasts.71
Bone morphogenetic proteins provide proper stimulation for osteoblasts or progenitor cells toward osteogenic differentiation. However, some biomaterials can induce intrinsic osteoinduction, in which MSCs differentiate into osteoblasts, even without the contribution of BMPs, thereby avoiding the potential adverse effects of BMP treatment.19
The process of osteogenic differentiation may be directly triggered by surface topography and inorganic ion release (in the case of calcium phosphate-based ceramics).62 When implanted within a coralline hydroxyapatite scaffold, adipose tissue-derived MSCs promoted the formation of new bone and enhanced bone healing of critical-size defects in rat mandibles. Descriptive histology and histomorphometry revealed a significant (p < 0.05) increase in bone regeneration values in the cell-treated defects at 3 and 6 weeks.72
An in vitro study by Gao et al. demonstrated that β-TCP granules affected bone mesenchymal stem cells (BMSCs) by improving their proliferation and osteogenic genes through promoting their expression and the formation of related proteins. Additionally, the 1–2.5-millimeter granule scaffolds exhibited superior function compared to the 1-millimeter β-TCP granules. Furthermore, an in vivo study demonstrated that the 1–2.5-millimeter β-TCP granules facilitated new bone formation without the application of any exogenous cells or growth factors.43
Another cell line that plays an important role in bone tissue regeneration is macrophages. Studies on animal models have proven that macrophage–MSC communication is essential for bone regeneration, and that macrophages probably play the most important role during the early stages of fracture healing.73 However, many studies have shown seemingly contradictory results, which is suggested to be the result of technical differences among the studies (i.e., different sources of cells, maturity of the monocytes/macrophages, and specific co-culture conditions). In point of fact, all subpopulations of monocytes and macrophages have the ability to promote MSC-mediated osteogenesis, although their relevance fluctuates depending on the ambient physiological conditions: while M0 macrophages are the most important in physiological bone homeostasis, M1 and M2 macrophages show greater significance in particular stages of fracture healing. Presumably, the timing and duration of the M1 macrophage-mediated inflammatory reaction is a critical determinant in the outcome of subsequent bone regeneration.73
Vasculature
Since free grafts do not have a proper vascular connection with the rest of the host, and oxygen diffusion reaches only cells located 100–200 µm from blood vessels, fabricated constructs may face oxygenation problems if the layer between vessels is thicker than 400 µm. Observations following in vivo implantations have shown relatively slow and insufficient capillary ingrowth into thick constructs.74 Therefore, tissue engineers must first create functional vasculatures into the engineered tissue to provide nutrient and oxygen supply, as well as to effectively remove waste products.75 Highly developed vascularization in engineered bone tissue was shown to positively impact osteogenesis, lower the risk of ischemic necrosis and enhance mechanical properties.76 Additionally, adequate vascularization promoted successive recruitment, differentiation and proliferation of osteoprogenitor cells as well as efficient gas exchange with subsequent bone homeostasis.77
The creation of new blood vessels is possible through 2 processes. First, angiogenesis is the formation of new capillaries from existing blood vessels.64 Vasculogenesis, on the other hand, is the formation of a primitive vascular network by differentiation of endothelial progenitor cells or angioblastic progenitor cells into ECs.78
The maturation of newly formed vasculature through angiogenesis or vasculogenesis requires meeting certain conditions: 1) recruitment of mural cells; 2) generation of an ECM; and 3) specialization of the vessel wall for structural support and regulation of vessel function. In addition, parenchymal cells require an adequate nutrient supply, which can only be achieved when there is proper organization of the vascular network. All of these processes are finely regulated by a variety of receptors and ligands and their expression or concentration, as well as the influence of physical forces. Physical or biochemical disturbances of these factors result in abnormal vasculature, which may underlie future pathologies.79
As mentioned earlier in this review, there are many different ways to ameliorate vasculature nascence and growth. Angiogenesis can be promoted through the influence of MSCs, as they cause an increase in the number of vascular branches.53
An in vitro and in vivo study by Temple et al. tested varying internal porosities in anatomically shaped PCL scaffolds. The properties of these scaffolds were compared in terms of influencing human adipose-derived stem cells into producing vasculature and bone, which are 2 essential elements of bone tissue. The researchers demonstrated large scaffolds of maxillary and mandibular bone printed with precise details gathered from patients’ computed tomography (CT) scans.80 As another construct example, a functioning model of a fabricated vascular network was created with GelMA hydrogels. The authors of that study confirmed that the channels they produced were lined with endothelial monolayers. This suggests that GelMA is potentially an adequate substance for printing vascular networks.36 Byambaa et al. gave another example of GelMA application in constructing whole vasculature within large-scale 3D-printed constructs. The co-culture of human bone marrow-derived MSCs and human umbilical vein endothelial cells (HUVECs) was integrated into bone-like tissue matrices with a perfusable vascular lumen. In order to print perfusable vessels within the construct, the authors formed a cylinder with 5% GelMA hydrogel at low methacryloyl substitution (GelMALOW). They also loaded GelMA hydrogel with silicate nanoplatelets to induce osteogenesis, and synthesized hydrogel formulations with chemically conjugated VEGF to promote vascular spreading. The whole construct successfully supported proliferation and cell survival and remained structurally stable for 21 days of in vitro tests.37 Anada et al. bioprinted 2 GelMA rings, creating a vascularized bone-mimetic construct with a central ring and peripheral ring to mimic bone marrow and cortical bone, respectively. The central ring contained HUVEC spheroids, and the peripheral ring contained octacalcium phosphate. As a result, octacalcium phosphate induced osteoblastic differentiation of the MSCs, while in the center, the HUVEC spheroids stimulated capillary network formation. In conclusion, both osteoblastic and angiogenic differentiation can be successfully achieved in the hydrogel environment.38
As for directly printing vasculature, Dolati et al. printed conduits with carbon nanotubes as an additional mechanical reinforcement and a way to improve bioprintability. Their study became the foundation for more advanced constructs where, instead of carbon nanotubes, natural protein nanofibers could be used in large-scale tissue fabrication.81
Jusoh et al. prepared a vascularized bone tissue model made of ECM with incorporated hydroxyapatite. Not only did various hydroxyapatite concentrations in the ECM result in varying mechanical properties, but mechanically modulated hydroxyapatite–ECM interactions affected sprouting angiogenesis. Furthermore, hydroxyapatite improved not only sprouting speed but also lumen diameter, length and number of newly formed vessels.82
Not only chemical particles but also physical factors affect vascularization. A study by Kuss et al. regarding the influence of oxygen levels showed that long-term hypoxia resulted in less vascularization and lower cell viability, while short-term hypoxia promoted vascularization-related gene expression. Experiments were conducted on stromal vascular fraction-derived cell (SVFC)-laden hydrogels and 3D- bioprinted composite scaffolds with polycaprolactone/hydroxyapatite (PCL/HAp). The results proved that short-term hypoxia accelerated microvessel development both in vitro and in vivo and helped merge with the host vasculature, although no osteogenic effect on SVFCs was proven. This effect could be embraced to promote in vitro prevascularization in order to rapidly achieve in vivo anastomosis.83
Another aspect worth considering is the application of spheroids. Spheroids can contain high concentrations of cells from the outset, while encapsulated cells require time to proliferate.84 This could be incredibly useful in regard to printing complex vascular networks. Norotte et al. successfully 3D-printed tubular vascular scaffold-free grafts with multicellular spheroids. Closely placed spheroids, used as building blocks, were assembled, fused and used to create a branched vascular tree. Moreover, when comparing tissue spheroids and multicellular cylinders, the latter showed improved precision of the construct over a shorter period of time.85
Stabilization
Bone grafts should be designed to adapt precisely to the recipient site. Importantly, in order to increase blood supply for the graft, it is recommended to perforate the recipient site with a round bur of 1.0 mm in diameter.86 Afterwards, the bone block can be placed in a passive manner and fixed without any excessive tension to the alveolar bone, usually with titanium miniscrews. The length and number of screws depended greatly on the clinical situation, such as recipient bone conditions and the thickness of the block.87 Improper fixation of the graft may cause tension within forming tissues and eventually constrain bone healing. A thorough surgical procedure strategy and fine management of soft tissues, including adequate flap design, are essential for osseointegration and more predictable wound healing.86
Currently, titanium osteosynthesis and screws are the default choice in orthognathic surgery and maxillofacial traumatology.88, 89, 90
Alternatively, resorbable pins can be used.91 Biodegradable systems reduce the number of necessary surgical interventions, as there is no need to remove them after the initial procedure. However, it has been reported that the degradation products of these systems may cause adverse tissue reactions.90 Additionally, prolonged resorption time and greater screw diameter should be taken into consideration.87
As bioprinting technology offers new regeneration possibilities, it may also introduce new solutions for fixation that are different from screws.
Discussion
The clinical use of 3D bioprinting is another step forward toward personalized medicine. This blend of different areas of sciences, such as engineering, biotechnology, medicine, and material sciences, is persistently being developed, as each of them presents new discoveries every day that can escalate the progress of the others. With innovative solutions, tissue engineering may be able to lower its costs, which is a necessary condition for achieving broad public access to this technology. Hopefully, patients with maxillofacial bone defects, tumor diseases, bone fractures, or alveolar atrophy will soon be easily able to benefit from the potential of 3D bioprinting.
Limitations
A possible limitation of this study is selection bias. The process of choosing the articles to be included in the paper was conducted independently by 2 researchers. Despite the steps taken to prevent it, it is possible that some studies that deserved to be included in this review may have been omitted.
Conclusions
All crucial elements of the diamond concept of healing are achievable through the use of 3D bioprinting, which has been both discussed theoretically and applied clinically with promising outcomes. Among the most promising scaffolds and bioinks are COL I, GelMA and dECM. The most accessible and suitable stem cells are MSCs. As for growth factors and differentiation factors, various substances and particles may empower the final results, such as VEGF, TGF-β1, Ang-1, hydroxyapatite, and β-TCP. In order to build functioning vasculature, researchers have used GelMA hydrogel scaffolds, carbon nanotubes, hydroxyapatite properties, different oxygen levels, and spheroids as building blocks. The stabilization issue is still to be resolved, and the newly created tissue should be precisely fitted and fixed without excessive tension (i.e., using titanium miniscrews or resorbable pins). Despite these advances, as this study shows, there is still room for improvement in all aspects of clinical bioprinting.

