
















Abstract
Background. Motion analysis systems have been widely used in orthopedics and rehabilitation for diagnostics, patient monitoring and outcome evaluation purposes. Since Microsoft Azure Kinect Developer Kit (DK) had been released, only a few studies were published concerning its usage. However, it has not been used for wrist motion assessments, even though the use of standardized examinations with known reliability, validity and responsiveness remains a constant challenge.
Objectives. This study aimed to examine the reliability of hand and forearm range of motion (ROM) measurements recorded using new software utilizing the Microsoft Azure Kinect DK.
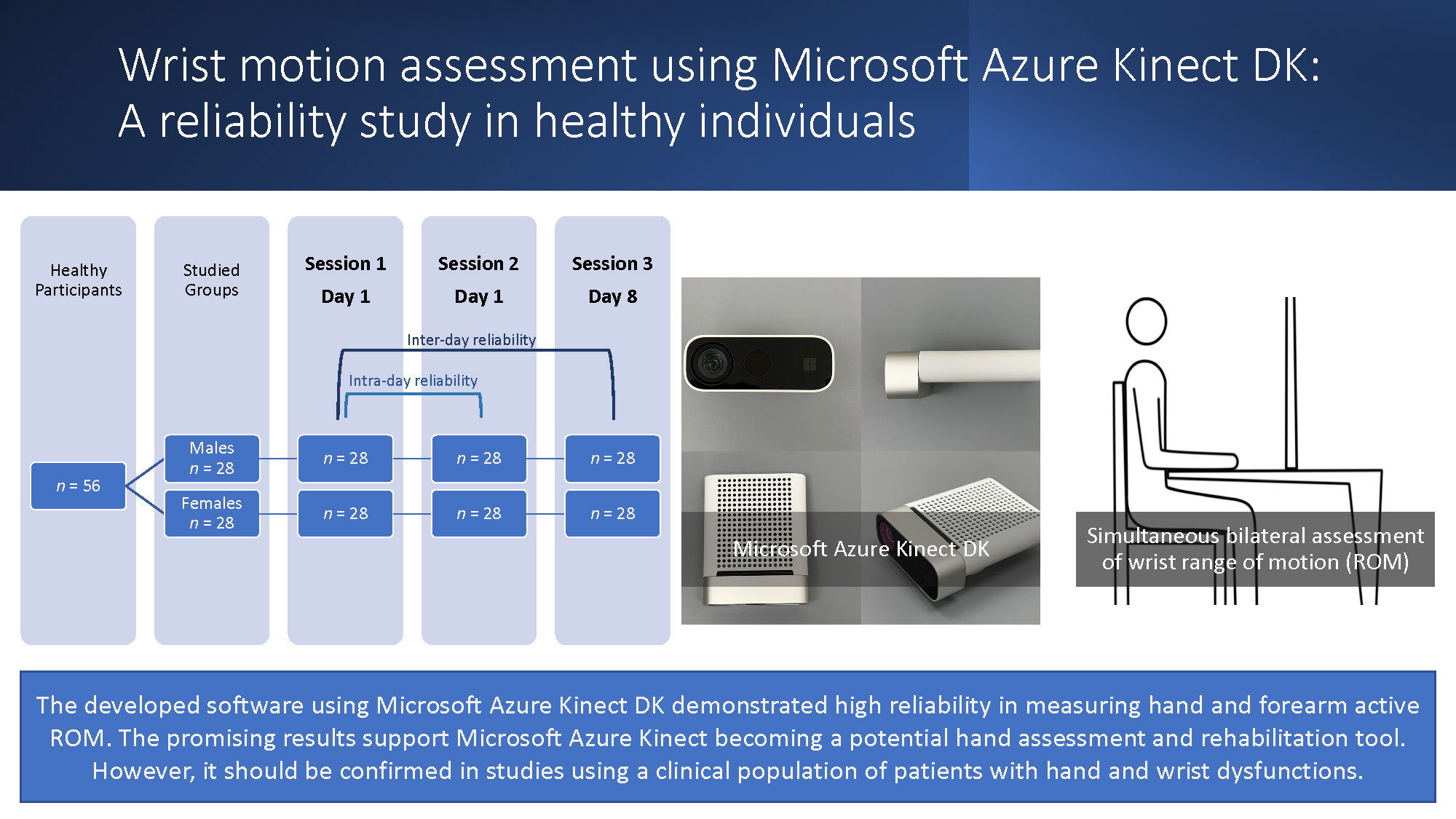
Materials and methods. Twenty-eight healthy males and 28 healthy females participated in measurements of active ROM for wrist extension, wrist flexion, radial deviation, ulnar deviation, and forearm supination and pronation on 3 separate occasions. Sessions 1 and 2 were carried out on the same day with a 90-minute rest period between each session, while the 3rd session was conducted a week later. Data were recorded simultaneously in both limbs using a custom-made software developed by a software development company (Oleksy Medical & Sports Sciences, Łańcut, Poland) for the purposes of the present study using Microsoft Azure Kinect DK. The assessment of intra-day and inter-day reliability was based on intraclass correlation coefficient (ICC) calculations and interpreted based on commonly used guidelines.
Results. In the group of males, the lowest ICC was 0.846 for intra-day comparisons and 0.816 for inter-day analyses. In the female group, the lowest ICC for intra-day comparisons was 0.826 and exceeded 0.833 for inter-day comparisons.
Conclusions. The developed software using Microsoft Azure Kinect DK demonstrated high reliability in measuring wrist and forearm active ROM. These promising results support the use of Microsoft Azure Kinect DK in a clinical capacity as a potential hand assessment and rehabilitation tool.
Key words: rehabilitation, orthopedics, hand, patient monitoring, motion
Background
Motion analysis systems have been widely used in orthopedics and rehabilitation for diagnostics, monitoring progress and evaluating outcomes. Optoelectronic motion capture systems based on markers have generally been considered the gold standard for motion analysis research.1, 2, 3 One proposed alternative to optoelectronic systems is human motion analysis using wearable inertial sensors.4, 5 Also, markerless motion capture systems have been validated and applied to functional diagnostics and rehabilitation.6, 7, 8
The common commercially available sensors used for markerless motion analysis are Leap Motion Controller (LMC; Leap Motion Inc., San Francisco, USA) and consecutive versions of Microsoft Kinect sensors (Kinect for Windows v. 1 (V1) and Kinect for Windows v. 2 (V2); Microsoft Corp., Redmond, USA).9, 10 For center-based and home rehabilitation purposes, Nintendo Wii Mote, Wii Balance Board (Nintendo Inc., Redmond, USA) and Microsoft Kinect motion-sensing game controllers have gained popularity over the past years.11, 12, 13, 14
Since Microsoft had released Azure Kinect Developer Kit (DK) in 2019, only a few studies were published concerning its usage. The literature describes its use in rehabilitation-related purposes and hand gesture recognition.15, 16, 17, 18 However, it has not been used for hand motion assessments, even though standardized examinations with known reliability, validity and responsiveness remain a constant challenge in physiotherapy.19 When evaluating the reliability of a new testing method, it is primarily performed on healthy individuals to make sure that repeated trials on the same participants are reproducible.20
Objectives
This study aimed to evaluate the reliability of wrist and forearm range of motion (ROM) measurements recorded using new software developed for Microsoft Azure Kinect DK.
Materials and methods
Study design
The test–retest reliability was employed to determine the variation in the ROM measurements assessed using custom-developed software and Microsoft Azure Kinect DK in the same participant under the same conditions. The development of the software for the purposes of the present study was outsourced to a software development company (Oleksy Medical & Sports Sciences, Łańcut, Poland) that designed it according to the predefined specification. The test–retest design was chosen as it assumes that in a software reliability assessment the effect of an examiner is rather negligible. Therefore, levels of consistency were precisely noted between 2 measurements taken on the same day (intra-day reliability) and 2 measurements taken on different days (inter-day reliability).
Setting
The present study was performed in 2020–2021 in an academic setting. Each participant took part in 3 measurement sessions. Sessions 1 and 2 were performed on the same day, separated by a 90-minute rest period. Session 3 was carried out exactly a week later. A flowchart of the study is presented in Figure 1.
Participants
The first 28 male and 28 female students from the university who volunteered to participate and met all the inclusion criteria comprised the study group. In all studied participants, an interview and physical examination were carried out to assess their general health and musculoskeletal system condition. The inclusion criteria encompassed a dominant right upper limb, lack of musculoskeletal disorders and injuries to the upper limbs, cervical spine and thoracic spine, and no diagnosed general diseases. Upper limb dominancy was determined by asking the participants which hand they use to write. During the 1st session, all participants underwent body height and mass measurements and their body mass index (BMI) was calculated.
Variables
The measured variable was a maximal value of wrist extension, wrist flexion, radial deviation, ulnar deviation, forearm supination, and forearm pronation. The results were expressed in degrees [°], and recorded separately for dominant and non-dominant upper limbs during 3 separate measurement sessions.
Measurement
The variables mentioned above were obtained during the measurements of active wrist ROM. The measurements were carried out on the wrists simultaneously and bilaterally. The 3 measurement sessions were performed by the same examiner who was trained and experienced in the use of the developed software. The examiner asked participants not to change their regular training regimens during the 8-day-long experiment. The sessions were conducted at precisely the same time in the morning.
Data recorded by the developed software for the present study using Microsoft Azure Kinect DK is presented in Figure 2. Microsoft Azure Kinect DK is a device that uses infrared light to generate in-depth images that give a 3D representation after a process called reconstruction. The custom application was written using a Unity-based engine. A custom plugin was created to include the Microsoft Software Development Kit (SDK) for the Kinetic Azure device.
One Microsoft Azure Kinect DK was set up on the desk using a frame that faced down to the desk, as shown in Figure 3. Metcalf et al. previously suggested a similar method.6 The participants sat by the desk with both arms close to their bodies. The elbows were flexed 90°. Their forearms were placed on the desk, parallel to one another.
For measuring wrist extension and flexion, the participants placed their forearms in a midline position, also called neutral or zero position. At first, the participants extended their wrists maximally, and their fingers were allowed to flex passively. Next, the participants returned to the starting position and consecutively flexed their hands maximally.
The starting position for measuring radial and ulnar deviation was with the forearm in pronation and the hand in neutral. First, the participants performed maximal radial deviation. Then, from the starting position, they performed maximal ulnar deviation.
The forearm was then placed in the midline position for measuring rotational movements. First, the participants rotated their forearms to maximum supination. Then, after placing the forearm in a midline position, the participants rotated the forearm into maximum pronation.
Verbal commands were used during the assessment. The participant performed 3 repetitions of each movement within the full ROM; however, the parameter taken for analysis was the maximal value obtained during the 3 repetitions.
Bias
To address a potential source of bias, the reliability of wrist and forearm ROM measurements were recorded separately for males and females. Additionally, the statistician was blinded regarding the gender of the participants, as well to the type of the analysis (intra-day and inter-day reliability).
Study size
The minimal sample size was determined using the method described by Bujang and Baharum.21 Two measurements were performed for intra-day and 2 for inter-day reliability assessment purposes, with a statistical power of 80%, and a minimum intraclass correlation coefficient (ICC) of 0.50 required a minimal number of participants of 22. An additional 20% of participants were added in case of dropouts between the sessions, also according to the Bujang and Baharum’s guidelines.21
Quantitative variables
The maximal values of wrist and forearm motion between sessions 1 and 2 were taken for comparative analysis for the intra-day comparison. The results from the 1st and 3rd session were considered to determine inter-day reliability.
Statistical analyses
The statistical analysis was carried out using IBM SPSS Statistics Premium v. 28 (IBM Corp., Armonk, USA) and Microsoft Office Excel 365 Personal (Microsoft Corp.).
Calculation of the arithmetic mean (x) and standard deviation (SD) was performed for the participant’s age, body height, body mass, and BMI. Using the Shapiro–Wilk test, the data of the maximal values of assessed movements, expressed in degrees [°], were found to be normally distributed. Two-way mixed effects, absolute agreement and single examiner/measurement form of the ICC, determined by McGraw and Wong, were used.22 According to guidelines by Koo and Li, the ICC interpretation was based on an estimated ICC 95% confidence interval (95% CI).23 The ICC values were also interpreted with reference to the criteria proposed by Cicchetti and Sparrow as follows: ICC < 0.40 – poor; ICC = 0.40–0.59 – fair; ICC = 0.60–0.74 – good, and ICC ≥ 0.75 – excellent.24 One-way analysis of variance (ANOVA) and F tests were used for rating the significance of the ICC. A p-value <0.05 was considered statistically significant.
Results
As presented in Figure 1, 28 males (age x = 22.32 ±0.99 years, body height x = 178.77 ±4.10 cm, body mass x = 76.36 ±3.86 kg, and BMI x = 23.88 ±0.60 kg/m2) and 28 females (age x = 21.73 ±1.24 years, body height x = 169.36 ±5.06 cm, body mass x = 60.82 ±5.06 kg, and BMI x = 21.18 ±1.08 kg/m2) took part in 3 consecutive sessions. There were no dropouts from the study and no missing data to be addressed.
As presented in Table 1, in the group of males, the intra-day reliability in the dominant and non-dominant limbs was rated good to excellent. The lower bound of ICC values was noted in wrist flexion of the non-dominant limb and exceeded 0.607. The highest upper bound of ICC values were observed in non-dominant limb forearm supination and exceeded 0.995. In the female group, the intra-day reliability was good to excellent, with a lower bound of ICC of 0.631 for wrist flexion in the non-dominant limb and the upper bound of ICC of 0.990 for radial deviation in the non-dominant limb.
As presented in Table 2, the inter-day reliability was good to excellent in both males and females. For the male group, the lower bound was noted for ulnar deviation in the dominant limb and exceeded 0.616. The upper bound exceeded 0.988 and was reported in forearm supination of the dominant limb. In females, the lower bound of ICC was 0.642 for wrist flexion in the non-dominant limb. The upper bond of ICC was 0.993 for ulnar deviation in the non-dominant limb.
Discussion
Our study determined that the new software utilizing Microsoft Azure Kinect DK demonstrates high reliability in measuring wrist movements in the sagittal and frontal planes and forearm rotational movements.
In motion analysis, the quality and quantitative parameters of movement can be distinguished. The most common quantitative parameters used in clinical rehabilitation include biomechanical variables like postural angles, pressure distribution, moments, and forces produced by examined patients.5 Motion capture has been utilized in numerous fields, including biomechanical analysis of clinical populations with hand and wrist dysfunctions. The so-called gold standard optoelectronic motion capture systems are based on camera tracking and data collection on the position of retroreflective markers placed on the body of the examined patient. The positional data has been used to perform biomechanical analysis in static and dynamic conditions.1, 2, 3, 25 However, marked motion capture systems have some limitations. They are expensive and few clinical centers can afford them. The placement of the markers on the hand is also challenging. Apart from the fact that such measurements are time-consuming, there are patients with diseases in which the placement of markers can cause difficulties, such as in patients with complex regional pain syndrome (CRPS).26
Of course, there are some non-marker-based possibilities available to track wrist motion, like instrumented gloves. They are less expensive than marker-based systems and their usage is not limited to the laboratory setting.27, 28 Although the gloves come in different sizes, they cannot be perfectly adjusted to every patient, especially considering various deformities from hand diseases and injuries. Moreover, the gloves are in complete contact with the patient’s skin, which can influence the performed movement. There are also conditions where the contact of the glove with the patient’s skin is contraindicated.9
Another option for hand motion analysis is computer vision-based systems. An example of this system is Monochrome Egocentric Articulated Hand-Tracking for Virtual Reality (MEgATrack), which was introduced by Han et al.29 It should be noted that studies using this system are promising; however, there is still a need for its validation in clinical settings.
The LMC, released in 2013, was supposed to allow the analysis of hand motion at a low cost.9 However, its utility was initially criticized because the area of motion tracking was relatively limited. Moreover, the examination capacity itself was also limited because a lot depended on the placement of the device.30 However, promising results appeared in studies by Houston et al., assessing an updated LMC released in 2018, that allowed for data capturing using multiple cameras in one setup.9
In 2010, Microsoft released Kinect V1 with an integrated RGB and infrared (IR) camera, primarily designed as a gaming controller for Xbox. The Kinect V1 allowed users to interact with games without a controller device.31 Four years later, an improved version of the Kinect V1 was launched; however, Microsoft halted the production of this device.32
Because the Microsoft Azure Kinect DK is a relatively new sensor option, the literature supporting its use for rehabilitation-related purposes is limited.15, 16, 17, 18 In a study by Albert et al., a comparative analysis between the Microsoft Azure Kinect DK and Microsoft Kinect V2 was carried out by performing gait analysis on a treadmill. Additionally, a gold standard optoelectronic Vicon motion capturing system was used. The study supported the usage of Microsoft Azure Kinect DK and Microsoft Kinect V2 for the analysis of temporal gait parameters. However, the Microsoft Azure Kinect DK superiority in spatial gait parameters was highlighted.17 Also, Yeung et al. supported the use of Microsoft Azure Kinect DK for tracking gait patterns while walking on a treadmill, and compared the results to the Microsoft Kinect V2 and Orbbec Astra Pro v. 2.16 Antico et al. examined the accuracy of Microsoft Azure Kinect DK in examining postural control and concluded it is a promising technique in the future of home rehabilitation.15 Apart from direct rehabilitation-based purposes, Lee et al. developed a real-time system using Microsoft Azure Kinect DK for gesture recognition.18
As presented above, some studies support the usage of Microsoft Azure Kinect DK for rehabilitation-related purposes; however, none of the authors reported reliability measurements performed neither in different sessions on the same day nor in sessions performed on different days.15, 16, 17 Therefore, it is impossible to compare the results obtained in the present study to other studies. Also, all the mentioned studies had very small study groups compared to this paper. Antico et al. conducted their study on 26 participants (18 males and 8 females), Yeung et al. on 10 healthy participants (2 females and 8 males), and Albert et al. on 5 participants,15, 16, 17 while Lee et al. assessed the defined features in a group of 10 people.18
As the present study supports the utility of Microsoft Azure Kinect DK for diagnostic and monitoring purposes, another interesting issue that might attract researchers’ attention is the possibility of using it to assess the functional direction of wrist joint motion. It has been determined that most activities of daily life are performed using functional wrist oblique motion that occurs in the plane of the dart-throwing motion (DTM), specifically from radial extension to ulnar flexion.33, 34, 35, 36, 37, 38 So far, inertial measurement units, optoelectronics systems with reflective skin markers and standard goniometry have been used to measure the range of the DTM.33, 39, 40
Limitations
The main limitation of our study is that the accuracy of the Microsoft Azure Kinect DK has not been compared to an optoelectronic system or other motion sensors. So far, the Microsoft Azure Kinect DK has been compared to the Vicon 3D system and Microsoft Kinect V2 in the context of treadmill walking by Albert et al.,17 and to the Vicon 3D system in the context of the assessment of postural control by Antico et al.15 Therefore, when using Microsoft Azure Kinect DK, raw data should not be compared to raw data recorded by another sensor until research on this topic is available.
As in our study, reliability tests are performed on healthy individuals. The next step should be to validate the wrist and forearm ROM measurements using Microsoft Azure Kinect DK on a group of patients with hand and wrist dysfunctions to confirm its clinical capacity as a hand assessment device and hand therapy tool.
Conclusions
The developed software using Microsoft Azure Kinect DK demonstrated high reliability in measuring hand and forearm active ROM. The promising results support Microsoft Azure Kinect becoming a potential hand assessment and rehabilitation tool. However, it should be confirmed in studies using a clinical population of patients with hand and wrist dysfunctions.


