
















Abstract
Background. Serum beta-human chorionic gonadotropin (β-hCG) is an important biomarker for the detection of ectopic pregnancies (EPs). The β-hCG levels between days 1 and 4 after methotrexate (MTX) treatment as an indicator of the success of the MTX in EP have been the focus of research.
Objectives. To determine whether the change in the β-hCG levels at day 1 and 4 and pretreatment at 48-hour increments can predict early treatment failure of single-dose MTX in EP.
Materials and methods. This was a retrospective study of 1120 EPs treated with a single dose of MTX. Treatment failure was defined as an obligation to proceed to surgery or the need for additional doses of MTX.
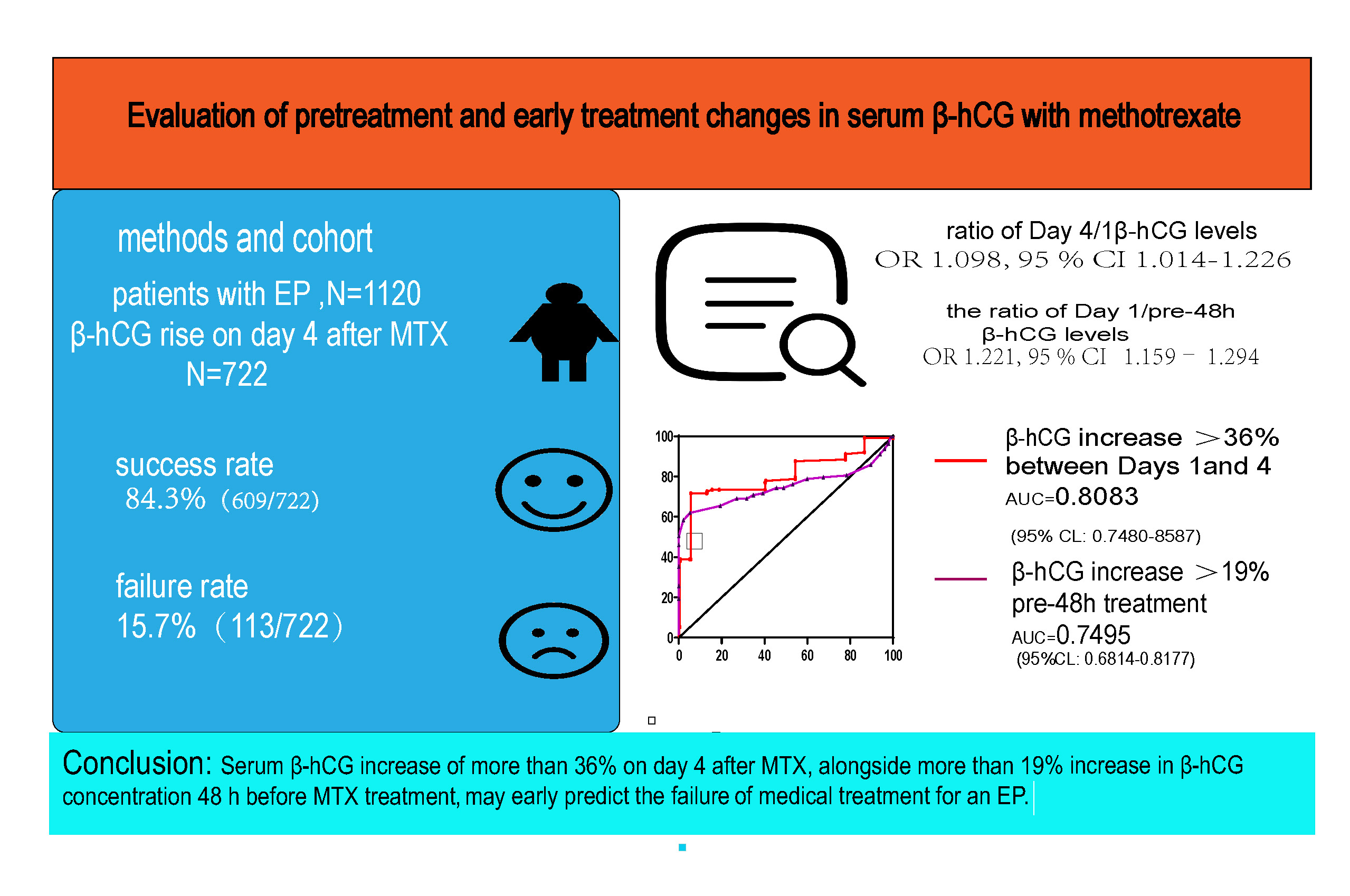
Results. A total 722 out of 1120 EPs had an increase in β-hCG on day 4 after MTX treatment. The logistic regression analysis indicated that 3 dependents were significantly associated with treatment failure: 1) a pretreatment 48-hour increase in β-hCG (odds ratio (OR): 1.249, 95% confidence interval (95% CI): 1.008–2.049, p < 0.001); 2) a change in β-hCG between day 1 and 4 (OR: 1.384, 95% CI: 1.097–2.198, p < 0.001); and 3) a history of EP (OR: 1.208, 95% CI: 1.041– 2.011, p < 0.001). The optimal cutoff point for the prediction of treatment failure was an increase of more than 19% in the 48 h before the treatment, and an increase of more than 36% between day 1 and day 4 in β-hCG concentrations. Patients with an increase in β-hCG levels of less than 36% on day 4 experienced MTX treatment failure in 4.2% (n = 25), compared to 74.5% (n = 88) of the patients with an increase above 36%.
Conclusions. A serum β-hCG increase of more than 36% on day 4 after the administration of MTX alongside a more than 19% increase in β-hCG concentration 48 h before the MTX treatment may predict the early failure of medical treatment for an EP.
Key words: β-hCG, methotrexate, ectopic pregnancy
Background
Ectopic pregnancy (EP) is a common acute gynecological issue. Its incidence has increased significantly all over the world in recent years. Tubal pregnancies are approx. 2% of all pregnancies. An available treatment of non-ruptured tubal pregnancy used all over the world is a single dose of methotrexate (MTX). It was first identified for the treatment of tubal pregnancies by Stovall et al.1 The tubal EP and MTX treatment protocol have attracted the attention of researchers in recent years.2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15 Jurkovic et al. followed up EP with low serum beta-human chorionic gonadotropin (β-hCG) levels (<1500 IU/L) and confirmed the diagnose of EP by ultrasonography. They administered a single-dose injection of MTX at 50 mg/m2 to the treatment group. In the group of patients who did not undergo a surgical protocol, a decrease in serum β-hCG to <20 IU/L or a negative pregnancy test was determined as a successful treatment.2 It has been stated that the success rate of MTX may be more effective in subgroups with lower values of serum β-hCG, especially below 2000 mUI/mL.14 In another study, it has been suggested that MTX treatment administered as a single dose had increased success rates in EP with lower serum β-hCG at the start of treatment. They reported that changes in serum β-hCG within the first 4 days are important in determining the treatment protocol and efficacy. Similarly, if the serum β-hCG level is lower than 4% or increases in the first 4 days, an additional dose of MTX should be given on day 4.3, 7 In a study in which EP was evaluated retrospectively, the success rate of MTX administered at a dose of 1 mg/kg intramuscularly was assessed.4 Similar to our study, serum β-hCG levels on days 0, 4 and 7 were evaluated after the administration of MTX, and it was suggested that differences in β-hCG levels between days 0 and 4 may serve as an early indicator for treatment outcome.5 According to Hoyos et al., the morbidly obese were 5 times more likely to require an additional dose compared to non-morbidly obese.6 Helvacioglu and Doğan reported that MTX administered in 2 doses significantly affected serum β-hCG levels and achieved successful results.8 It has been reported that a positive response in patients who are adequately treated with MTX, together with the low and decreasing serum β-hCG levels, rarely results in ruptured EP,9 and it reminded again that it should not be overlooked in the surgical procedure.9 It was stated that in cases where ovulation is high and patients underwent laparoscopic left salpingectomy, serum β-hCG should be followed up after the definitive treatment of tubal EP including surgical interventions.11 Lin and Hsieh found the initial serum β-hCG level to be 1,258 mIU/mL. They reported that they applied laparoscopic salpingectomy at the end because the increase continued and did not fall into the acceptable range after 1 month despite the 2nd and 3rd doses of MTX given to the patients.10 Grigoriu et al. reported that right salpingectomy was performed after unsuccessful MTX treatment.14 Cohen et al. observed that women with an increase in serum β-hCG >69% within 48 h prior to MTX had an 85% probability of tubal rupture, and that women with serum β-hCG elevation <20% had a lower absolute risk for tubal rupture.12 They also reported that medical treatment with a single dose of oral mifepristone, as well as systemic multi-dose MTX with folinic acid were required when a living fetus and high serum β-hCG levels were present.13
The success rates of MTX treatment have been determined to be between 52% and 96%, and the fertility rate with delivery after medical treatment for tubal EP is 67–80.7%. These rates are comparable to the success rates of surgical procedures.16, 17, 18, 19, 20 Serum β-hCG levels were measured on the 1st, 4th and 7th day after MTX treatment, and surgical intervention can be avoided when the levels decrease by more than 15% between the 4th and 7th day after a single dose of MTX.21 In recent years, researchers have observed a decrease in serum β-hCG levels between days 1 and 4 after MTX treatment in patients with EP, which significantly affects the success rates of treatment. The proper treatment protocol in a situation when serum β-hCG level rises on the 4th day is still being discussed among researchers.
This study aimed to comprehensively examine serum β-hCG level changes in the 48 h prior to the administration of MTX and changes between days 1 and 4 after MTX treatment to predict the early failure of MTX therapy.
Objectives
There are few studies reporting on increased serum β-hCG levels between days 1 and 4. Instead, many investigators wait until the 7th day to determine the treatment approach, while we aimed to determine it on day 4.
Materials and methods
Trial design
This retrospective study was conducted on patients in Shanghai First Birth and Infant Hospital, China, specifically women with EP who received 50 mg/m2 of MTX. The study obtained approval No. KS1959 from the Ethics Committee of Shanghai First Maternity and Infant Hospital. The Chinese Clinical Trial Registry number is ChiCTR2000030658.
Follow-up and procedures for patients
We reviewed patient records from the period from January 1, 2003, to December 31, 2019, using the hospital pharmacy MTX database. Ectopic pregnancy was diagnosed according to the standard criteria.21 In total, 1135 patients were admitted with the diagnosis of EP and received MTX treatment. Serum β-hCG values were measured on the 1st, 4th and 7th day in pregnant women administered MTX. Patients whose serum β-levels increased on day 4 were selected. An additional dose of MTX was given to the pregnant women when their serum β-hCG levels on the 7th day were less than 15% of the value measured between the 4th and 7th days. Study groups included a success group and a failure group, evaluated in terms of treatment outcomes. Successful treatment was defined as a decrease of more than 15% in serum β-hCG levels between the 4th and 7th day and no need for 2nd MTX treatment or surgery. Treatment failure was determined as the need for a 2nd MTX treatment or surgery in patients with EP. The values for these patients were not included in the statistical analysis.
Inclusion criteria were pretreatment serum β-hCG concentration ≤2000 U/L, no cardiac problems, gestational sac width <4 cm, biochemical values within expected values, and no problems with blood circulation. Exclusion criteria were ruptured tubal duct, non-tubal EP, or surgical intervention before the 4th day of MTX therapy. Methotrexate was administered to patients who met the specified criteria.
The day on which 50 mg/m2 of MTX was administered was defined as the 1st day. Serum β-hCG levels were then measured on days 4 and 7. All eligible patients consented to receive MTX therapy. In cases where serum β-hCG levels measured between days 4 and 7 decreased by >15%, serum β-hCG levels were not followed until negative values were detected. An additional dose of MTX was administered if serum β-hCG levels decreased by <15% with a stable condition, as was a 3rd dose of MTX if the patient would like to receive the treatment once again. In this situation, the patients have the choice to decide whether get a 3rd dose or have the surgery, in case of no contraindication of MTX therapy. Surgery was performed when levels decreased by <15%, there was an aggravated clinical syndrome or unstable condition, or the patient refused the 2nd dose of MTX. Additionally, during MTX treatment, we monitored the patients’ condition, including blood pressure, pulse and vaginal bleeding. Furthermore, we advised the patients to abstain from sex during treatment.
Statistical analyses
Statistical analyses were performed using IBM SPSS v. 19 (IBM Corp., Armonk, USA). The normal data distribution of continuous variables was verified with the Kolmogorov–Smirnov test. The Student’s t-test was used to analyze continuous variables with a normal distribution, and the results are presented as mean and standard deviation (M ±SD). When the data distribution was non-normal, the comparison was performed using the Mann–Whitney test. Categorical variables were compared using the χ2 test. In this study, we reported statistically significant positive and negative predictive values. The best cutoff value for changes in serum β-hCG levels between days 1 and 4 was determined using the receiver operating characteristic (ROC) curve method. When using the binary logistic regression model, the best model was built with the use of the Akaike information criterion (AIC), and the R-package “stats”, run in the R software v. 4.1.0 (R Core Team 2021, R Foundation for Statistical Computing, Vienna, Austria). Significant features in the logistic regression model evaluating MTX treatment were the ratio of day 4 to day 1 serum β-hCG levels, the ratio of day 1 to the day before the 48-hour treatment serum β-hCG levels, and day 1 serum β-hCG levels. The p-values <0.05 were considered statistically significant.
Results
A total of 1350 patients who received MTX treatment for tubal EP at the Shanghai First Birth and Infant Hospital Department between January 1, 2003, and December 31, 2019, were enrolled into the study. A total of 230 patients were excluded because they did not meet our criteria, of which 155 were due to suspected none-tubal EP or pregnancy of unknown location (PUL), 20 due to loss to follow-up, 25 due to incomplete records, and 30 due to abnormal blood circulation or surgery before the 4th day. The records of 1120 patients met the criteria for this study.
Baseline data
In total, 65% (722/1120) of patients had a serum β-hCG rise on day 4 and 35% (398/1120) had a drop on day 4 (Figure 1). In patients whose serum β-hCG levels increased on the 4th day after a single dose of MTX treatment, successful results were obtained in 609 patients (84.3%) and treatment failure was observed in 113 patients (15.7%). An additional dose of MTX was administered as supplemental therapy to 91 patients (80.5%) who did not respond to treatment. Twenty-two female patients (19.5%) who initially responded positively to MTX required surgical intervention. The main characteristics of the participants are presented in Table 1. There were no statistically significant age-related differences between the evaluated groups, gravidity, parity, days since last menstrual period (LMP), ectopic size, history of cesarean section, history of EP, and initial progesterone values. Endometrial thickness [mm] was significantly higher in the failure group compared to the success group (6.69 (6.50–6.88) compared to 8.13 (8.51–9.75); p = 0.000, Z = 7.952).
Evaluation of treatment results using serum β-hCG levels
Serum β-hCG levels on day 1 were 1075 (836–1252.5) mIU/mL in the success group compared to 1180 (986–1484) mIU/mL in the failure group. The difference was statistically significant (p < 0.001). This difference in serum β-hCG values was also found on day 4 (p < 0.001) and day 7 (p < 0.001). The median 48-hour pretreatment increment in β-hCG levels was lower in the success group (10% compared to 21%, p = 0.001). The ratio between differences on days 1 and 4 and between days 4 and 7 was calculated for each group. When serum β-hCG levels were compared between days 1 and 4, an increase in serum β-hCG levels was more pronounced in the failure group (p < 0.001). On the other hand, the decrease in serum β-hCG levels between days 4 and 7 was statistically significant in the success group (p < 0.001). These data are shown in Table 2.
The best cutoff value for the rise in serum β-hCG levels from day 1 to day 4 was 36%. This cutoff value provided a sensitivity of 72.57%, a specificity of 86.86%, and the area under ROC curve (AUC) of 0.8083 (95% confidence interval (95% CI): 0.7480–8587). The most significant rate of increase in serum β-hCG before 48 h of treatment was 19%. This cutoff value provided a sensitivity of 61.95%, a specificity of 94.75% and an AUC of 0.7495 (95% CI: 0.6814–0.8177). The most significant cutoff value for the determined serum β-hCG value on day 1 was 18%. This cutoff value provided a sensitivity of 80.95%, a specificity of 93.98% and an AUC of 0.9182 (95% CI: 0.8540–0.9825) (Figure 2).
Evaluation of serum β-hCG levels after MTX treatment
Binary logistic regression was performed based on AIC using the R environment. The best logistic regression model of AIC was found to be 344.9. The important covariates were the ratio of serum β-hCG levels on day 4 to day 1, the ratio of serum β-hCG levels on day 1 to 48-hour pretreatment, and day 1 serum β-hCG levels, the coefficients of which were 0.0941, 0.2003 and 0.0016, respectively. The odds ratios (ORs) (95% CIs) of these 3 covariates are shown in Figure 3.
In the group of patients whose β-hCG levels increased by less than 36% in the first 4 days of MTX treatment, the failure rate was 4.2%, while the success rate was 95.8% (579/604). On the other hand, when serum β-hCG level increased by more than 36% in the first 4 days, the success rate was 25% and the failure rate was 75% (Table 3).
Discussion
Changes in serum β-hCG levels in the first 4 days after a single dose of MTX, along with the concomitant need for a 2nd dose of MTX, can help determine whether an emergency surgery is necessary. However, the question remains whether it is an efficient indicator. The purpose of our research was to identify the association between the changes in serum β-hCG levels in the first 4 days after a single dose of MTX and MTX treatment outcome. Recently, the role of day 4 serum β-hCG levels has become a topic of debate among researchers; however, there are only few studies on increased serum β-hCG levels on day 4. In clinic, the question whether the treatment was successful after single-dose MTX when the day 4 serum β-hCG level increased was often discussed. Often, we could only wait for the assessment of serum β-hCG level on day 7. Based on the increase in serum β-hCG level on the 4th day, we aimed to investigate whether a surgical protocol could be applied. The percentage of serum β-hCG change during the first 4 days was considered an important criterion for the need for additional doses of MTX. Akselim et al. determined the threshold value of percent serum β-hCG ratio during the first 4 days to be 4% (sensitivity 72.9%, specificity 78.9%, positive predictive value 88.6%, and negative predictive value 56.6%).7 Some researchers found a transient increase in serum β-hCG levels of 26–60% due to a single dose of MTX.22, 23, 24 On the other hand, Helvacioglu and Doğan suggested that a 2-dose MTX protocol had a reasonable success rate on serum β-hCG levels.8 In a study examining serum β-hCG, progesterone levels and patient characteristics, they observed that the success rates were similar in both groups. They achieved success with MTX in 83% of patients and with placebo in 76%, and found that this difference was not significant in their statistical analysis. They reported that the MTX treatment was successful in 125 patients and unsuccessful in 37. When the serum β-hCG values measured on days 0, 4 and 7 were compared in pairs, the difference was reported to be statistically significant (p < 0.001). The mean serum β-hCG value was 783.0 in the success group and 1802.0 in the failure group (p < 0.001). However, they reported that the increase in serum β-hCG values during the first 4 days was 21.6% in the success group and 25.7% in the failure group (p < 0.001). This paper reported that MTX treatment was successful in 117 patients (73.6%) out of 159 women included in the study, while it was unsuccessful in 42 patients (26.4%). They observed that most of the patients (58.9%) had a tendency for decreased serum β-hCG values during the first 4 days, unlike the failure group, which had an increase in serum β-hCG values (76.2%). These researchers accepted a >18% decrease in serum β-hCG levels as an indicator of treatment success.8
Therefore, the key to this problem was the percentage of serum β-hCG change. In our study, 64.9% (737/1135) of patients had an increased serum β-hCG level in the first 4 days, with an initial level of less than 2000 mIU/mL, and all patients were selected strictly according to the inclusion criteria. However, treatment success was achieved in 82.6% (609/737) of these cases. Furthermore, in our study, the most influential covariates were 1) the ratio of day 4 to day 1 serum β-hCG level and 2) the cutoff value of a 36% increase on day 4, which predicted treatment success with a sensitivity of 72.57%, a specificity of 86.86% and an AUC of 0.8083 (95% CI: 0.7480–8587). For this reason, increased serum β-hCG levels on day 4 after the administration of MTX cannot be considered a criterion for treatment failure. This success could be explained by the theory that the vast majority of trophoblastic cells died after MTX therapy, released hCG, and then the MTX therapy failed. This was also demonstrated by our statistical data. Upon exceeding the cutoff value of the percentage increase, the greater the percentage increase on day 4, the lower the prediction sensitivity. This was the answer we had been looking for.
Other studies have shown decreased serum β-hCG levels within the first 4 days after the MTX treatment, with success rates ranging from 88% to 100%, which is consistent with our 84.82% success rate.22, 23, 24 Brunello et al. determined the threshold value for a decrease in serum β-hCG after the MTX treatment to be 10–22%, whereas in our study this rate was determined as 13%.25 The difference in cutoff values among these studies might be due to differences between patients (especially between different ethnic groups), inclusion/exclusion criteria, or definition of the treatment success. However, some studies have suggested that the lower the serum β-hCG level, the higher the probability of treatment success.26, 27, 28 In contrast, Gabbur et al. suggested that β-hCG levels on the 4th day could not be evaluated as an indicator of treatment success.29 Similarly, Cohen et al. concluded that neither absolute serum β-hCG levels nor percent changes in serum β-hCG levels within the first 4 days could predict treatment success after a single dose of MTX.30 In other studies, serum β-hCG values on day 4 and 7 were a better diagnostic criterion than the percentage decrease of serum β-hCG values between days 1 and 4. Çelik et al. reported that a decreased percentage between days 1 and 4 did not seem to be a better predictor than that between days 4 and 7.31 Girija et al. reported that the MTX treatment could be successful not only in patients whose serum β-hCG levels decreased on the 4th day, but also those whose serum β-hCG level increased on the 4th day. They observed that a >50% increase in serum β-hCG levels in the first 4 days significantly increased the risk of MTX treatment failure, as in our study.32 Although the sensitivity of the cutoff value for the rise in serum β-hCG levels from day 1 to day 4 was higher in our study, we should not make a decision arbitrarily. We took the 48-hour pretreatment increase in serum β-hCG into consideration. In our research, the best cutoff value for the rise in the serum β-hCG levels 48 h before treatment was 19%. This cutoff value provided a sensitivity of 61.95%, a specificity of 94.75% and an AUC of 0.7495 (95% CI: 0.6814–0.8177). The greater the increase 48 h before treatment, the higher the specificity.
If we had applied the 36% threshold level of serum β-hCG increase on the 4th day after a single dose of MTX, all patients who exceeded the 36% would have undergone surgery. However, a total of 55 patients would had not been included and the correct protocol would had not been applied. Based on this statistically significant result, we are aware that the most appropriate treatment in patients with serum β-hCG levels below 36% is conservative care. However, when serum β-hCG levels rise above 36%, the decision for surgery cannot be made definitively. Once we meet these criteria, we must pay attention to the 48-hour pretreatment increase in serum β-hCG. If an increase of more than 19% in 48-hour pretreatment serum β-hCG occurs, the possibility of surgery or a 2nd dose of MTX should be considered. By applying the increased serum β-hCG cutoff level, we were able to reduce the failure rate of patients with serum β-hCG levels that had an increase below 36% to 4.2%. However, we found in our study that 25.5% of patients with serum β-hCG levels above 36% were treated surgically and a single dose of MTX therapy was indeed successful. According to the results of our research, thanks to the increased serum β-hCG levels on the 4th day after a single dose of MTX treatment, the patient’s anxiety can be minimized and unnecessary surgeries reduced.
Limitations
The main limitations of our study are its retrospective nature and lack of case-control studies with a large number of patients for reference. It is obvious that there is a need for more comprehensive and prospective research on this population.
Conclusions
An increment of more than 19% in the 48 h before MTX treatment and an increase of more than 36% between the day 1 and 4 β-hCG concentrations were found to be good predictors of treatment failure. We think that we applied the treatment in the most accurate way in the follow-up evaluation after MTX treatment.


