Abstract
Background. High-resolution melting (HRM) analysis is a genotyping method which has the advantages of simple, rapid, low-cost and closed-tube operation.
Objectives. This study evaluated HRM analysis as an option for detecting the single nucleotide polymorphism (SNP) of cytokine, and profiled the distribution of cytokine gene polymorphism in the lung transplant recipients (LTRs).
Materials and methods. High-resolution melting-polymerase chain reaction (HRM-PCR) assays for genotyping tumor necrosis factor alpha (TNF-α) (–308 A/G), tumor growth factor beta 1 (TGF-β1) (+869 T/C), interleukin 10 (IL-10) (–592 C/A, –819 T/C, –1082 G/A), and interferon gamma (IFN-γ) (+874 T/A) SNPs were developed on the LightCycler® 480. The SNPs of the aforementioned cytokine genes in 322 LTRs and 266 normal controls were detected using HRM-PCR approach. To confirm the accuracy of the HRM-PCR assay, we randomly selected 100 samples from the LTRs and detected the aforementioned SNPs with sequence-specific primer-polymerase chain reaction (SSP-PCR) method, using a commercial kit.
Results. The data show that the HRM-PCR assay can distinguish all the cytokine SNPs, and the results of HRM-PCR analysis are in complete concordance to the genotyping results obtained using a commercial kit (κ = 1.0). Our data also show that the allele and genotype frequencies of the abovementioned cytokine are not significantly different between the LTRs and the control groups (p > 0.05). In addition, we found the genotypes of TGF-β1 +869 associated with high expression phenotype were prevalent in the LTRs. On the contrary, for TNF-α –308, IL-10 and IFN-γ, the genotypes associated with low expression phenotype were most common in the LTRs.
Conclusions. In this study, we described a rapid, low-cost and high-throughput HRM-PCR technology for genotyping cytokine SNPs. Our data may be utilized for future studies examining the associations of cytokine gene polymorphisms with the prognosis of the LTRs.
Key words: single nucleotide polymorphism, cytokine, lung transplantation, high-resolution melt analysis
Background
Cytokines are crucial signal molecules of immune-mediated diseases and transplant complications. The individual variability in cytokine production is determined through the effect of polymorphisms within regulatory regions of cytokine genes. In general terms, we can describe high, intermediate and low cytokine producer status according to the genotype. For tumor necrosis factor alpha (TNF-α), at position –308 within the promoter region, A/A, A/G and T/T genotypes correlate with a high, intermediate and low TNF-α production, respectively.1 Similarly, the substitutions in codon 10 (+869) and codon 25 (+915) of tumor growth factor beta 1 (TGF-β1) gene correlate with the protein production.2 The codon 10 *T (Leu) and codon 25 *G (Arg) of TGF-β1 are the high responder alleles. For interleukin 10 (IL-10), 3 single nucleotide polymorphisms (SNPs) at positions –1082, –819 and –592 comprise 3 haplotypes: ACC, ATA and GCC. The genotypes of ACC/ACC, ACC/ATA and ATA/ATA are classified as low, GCC/ACC and GCC/ATA as intermediate, and GCC/GCC as high IL-10 producer genotypes.3 Finally, at position +874 within the intron 1 of interferon gamma (IFN-γ) gene, the genotypes T/T, T/A and A/A are associated with high, intermediate and low expression, respectively.4
Studying cytokine gene polymorphism is important to understand the cause of interindividual variation in the pathogenesis, identify disease susceptibility and poor clinical outcomes, and develop novel strategies to prevent or delay the disease process. Therefore, much effort has been committed to developing rapid, accurate and cost-effective technologies for cytokine SNP analysis. Various strategies amenable to cytokine genotyping include restriction fragment length polymorphism (RFLP),5 sequence-specific primer-polymerase chain reaction (SSP-PCR),6 allele-specific oligonucleotide (ASO) hybridization,7 TaqMan genotyping assay,8 and direct DNA sequencing.9 Each approach has certain advantages in cytokine genotyping. However, these methods are also labor-intensive, time-consuming and expensive, especially for large genetic screening. High-resolution melting-polymerase chain reaction (HRM-PCR) analysis is an emerging sequence variation scanning technology.10 This relatively novel approach is based on the melting properties of double-stranded DNA. Sequence variations in PCR amplicon are detected using changes in melting profiles as the temperature is increased in the presence of DNA intercalating dyes. The HRM analysis is a simple, flexile, inexpensive, sensitive, and specific method. Indeed, this technique has been widely employed to screen gene variants, such as mutation detection,11 SNP typing,12 methylation analysis,13 and differentiation of bacterial strains.14 Therefore, we considered developing an HRM-PCR method for cytokine genotyping.
Lung transplantation is the only available treatment for various end-stage lung diseases. Despite recent advances in immunosuppressive therapy and human leukocyte antigen (HLA)-matching, acute or chronic graft rejection are common complications faced by the lung transplant recipients (LTRs), which occur in approx. 40% of patients during the first 6 months after allograft transplantation.15 Studies have shown that certain cytokine polymorphisms are implicated in acute rejection or the occurrence of chronic graft failure.16, 17, 18 It is proposed that cytokine SNPs analysis can help improve the medication design and the graft outcome after transplantation.19 Consequently, we profiled the distribution of cytokine polymorphism in the LTRs in the Chinese population.
In addition, the genetic heterogeneity in different ethnic populations results in the diverse distribution of cytokine polymorphism.20 Therefore, we compared the control results with those from other healthy populations and identified significant differences.
Objectives
The aim of this study is to develop HRM technology for detecting the SNP of cytokine and to profile the distribution of cytokine gene polymorphism in LTRs.
Materials and methods
Study population
In the present study, 322 patients who received lung transplantation between December 2004 and June 2016 were enrolled. The LTRs consisted of 90 females and 232 males, from 14 to 80 years of age (51.42 ±14.22 years, mean ± standard deviation (SD)). All patients were of the Chinese Han nationality and received the transplantation at the Department of Pulmonary Transplantation, Wuxi People’s Hospital of Nanjing Medical University, China. The characteristics of the study LTRs are displayed in Table 1. The differences in HLA molecules between the donor and the host make a crucial contribution to the alloreactivity. Recipients and donors were genotyped with SSP-PCR (HLA-ABDR kit; One Lambda, Los Angeles, USA), following the manufacturer’s instructions. The patient who best matched the donor HLA was selected as recipient for the lung transplantation.
Two hundred and sixty-six individuals (137 males and 129 females, aged 56.70 ±12.80 years, mean ±SD) from the same ethnicity and without systemic diseases were enrolled into the study as a control group. The differences in sex composition and age distribution are significant (χ2 = 26.31, p < 0.001; t = 4.687, p < 0.01, respectively) between the LTR and the control group.
All protocols were approved by the ethics committee on clinical new technologies and scientific research of Wuxi People’s Hospital of Nanjing Medical University, China, before the study began, and the protocols conformed with the ethical guidelines of the 1975 Declaration of Helsinki.
DNA extraction
Whole blood samples were collected before the transplantation and placed in test tubes containing EDTA-K2 anticoagulant. Genomic DNA was extracted using genomic DNA purification kit (Promega, Madison, USA), according to the manufacturer’s instructions. Briefly, 900 µL of Cell Lysis Solution was added to 300 µL of whole blood, mixed by inversion, incubated for 10 min at room temperature, and then centrifuged at 16,000 × g for 20 s. After centrifugation, the supernatant was discarded. Then, 300 µL of Nuclei Lysis Solution was added and it was pipetted to lyse the white blood cells. Next, 100 µL of Protein Precipitation Solution was added and vortexed for 20 s, and then centrifuged at 16,000 × g for 3 min. Finally, 300 µL of supernatant was transferred to a new tube containing 300 µL of isopropanol, mixed and centrifuged at 16,000 × g for 1 min. After centrifugation, the supernatant was discarded. Then, 300 µL of 70% ethanol was added and centrifuged as described in the step above. Next, the ethanol was aspirated and the pellet was air-dried for 10 min. The DNA was rehydrated in the appropriate volume of DNA Rehydration Solution for 1 h at 65°C.
Genotyping of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C,
and −1082 G/A), and IFN-γ (+874 T/A) genes with HRM-PCR assay
The HRM-PCR was performed on a LightCycler® 480 instrument (Roche, Basel, Switzerland) with 96-well trays. The primers for genotyping TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes were listed in Table 2. The PCR was performed in 20 μL volumes; the mixture included 2.5 mM MgCl2, 0.5 μM of both forward and reverse primer, 200 μM of each deoxynucleoside triphosphate (dNTP), 0.5 U of Taq DNA Polymerase (Promega), 1.0 μL of EvaGreen® (Biotium, Fremont, USA), and about 75 ng of DNA. All 6 cytokine amplicons were amplified with a touchdown PCR, as follows: an initial denaturation step at 95°C for 2 min; then the initial annealing temperature of 65°C was decreased by 0.5°C each cycle for 20 cycles and held at 55°C for 10 s for the next 30 cycles. For all cycles, denaturation at 95°C for 10 s and the extension at 72°C for 15 s were performed. The HRM was conducted at the end of each reaction and it consisted of increasing the temperature from 70°C to 99°C at intervals (ramps) of 0.02°C/s. The HRM analysis was carried out with the gene-scanning module software v. 1.5 (Roche). The software employs a three-step analysis: 1) the normalization by selecting linear regions before (100% fluorescence) and after (0% fluorescence) the melting transition; 2) the temperature shifting by moving the curves along the x-axis, facilitating grouping; and 3) the use of the auto-group function.
Genotyping of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes with commercial kit
The SSP-PCR is a highly sensitive and specific method of detecting sequence polymorphism, based on the sequence-specific primer with the first 3’-terminal base matching of the specific base of each allele. To confirm the accuracy of HRM-PCR analysis, we randomly selected 100 samples from the LTRs and tested the cytokine SNPs using Cytokine Genotyping Primer Pack (One Lambda), which employs the SSP-PCR method. Briefly, 19 µL of genomic DNA (50–100 ng/µL) was mixed with 140 µL of D-Mix and 5 U of Taq DNA polymerase (Promega). This DNA mixture was dispensed into 96-well trays prealiquoted with primers and amplified on an ABI 9700 thermal cycler (Applied Biosystems, Waltham, USA). Thermocycling conditions were 10 cycles of 94°C for 10 s, 65°C for 60 s, followed by 20 cycles of 94°C for 10 s, 61°C for 50 s and 72°C for 30 s. The amplified products were electrophoresed on 2% agarose gels. The reliability of SSP-PCR reaction was judged using a negative control tube and internal positive control in each tube. The typing results were interpreted using the worksheet provided with the product.
Comparison of allele frequencies of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10
(−592 C/A, −819 T/C and −1082 G/A),
and IFN-γ (+874 T/A) genes between Chinese and other national populations
The genetic heterogeneity in populations of different ethnicities may result in the diverse distribution of cytokine polymorphism. To explore the differences in the distribution of cytokine gene polymorphisms, we reviewed the available literature and compared the results from the control group with those from other healthy populations.
Statistical analyses
Statistical analysis was carried out using the SPSS v. 15 software (SPSS Inc., Chicago, USA). Allele and genotype frequencies were calculated by direct counting. The Hardy–Weinberg equilibrium (HWE) was tested using a χ2 test with one degree of freedom to compare the observed and expected genotype frequencies. The frequency differences for the cytokine alleles and genotypes were estimated using the χ2 test or the Fisher’s exact test. The agreement between the 2 methods for SNP genotyping was determined with a Kappa test. A probability value of p < 0.05 was considered statistically significant and all the reported p-values were two-tailed.
Results
Analysis of HWE for cytokine frequencies in the LTRs and control groups
The HWE testing for TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C, −1082 G/A), and IFN-γ (+874 T/A) genotypes revealed no significant deviation in the LTR group (χ2 test: χ2 = 1.49, p = 0.22; χ2 = 0.20, p = 0.66; χ2 = 2.21, p = 0.14; χ2 = 2.21, p = 0.14; χ2 = 1.49, p = 0.22; and χ2 = 0.66, p = 0.42, respectively) and in the control group (χ2 test: χ2 = 1.85, p = 0.17; χ2 = 0.06, p = 0.81; χ2 = 3.75, p = 0.05; χ2 = 3.75, p = 0.05; χ2 = 0.88, p = 0.35; and χ2 = 0.98, p = 0.32, respectively).
Genotyping of TNF-α (–308 A/G), TGF-β1 (+869 T/C), IL-10 (–592 C/A, –819 T/C and –1082 G/A), and IFN-γ (+874 T/A) genes with HRM-PCR assay
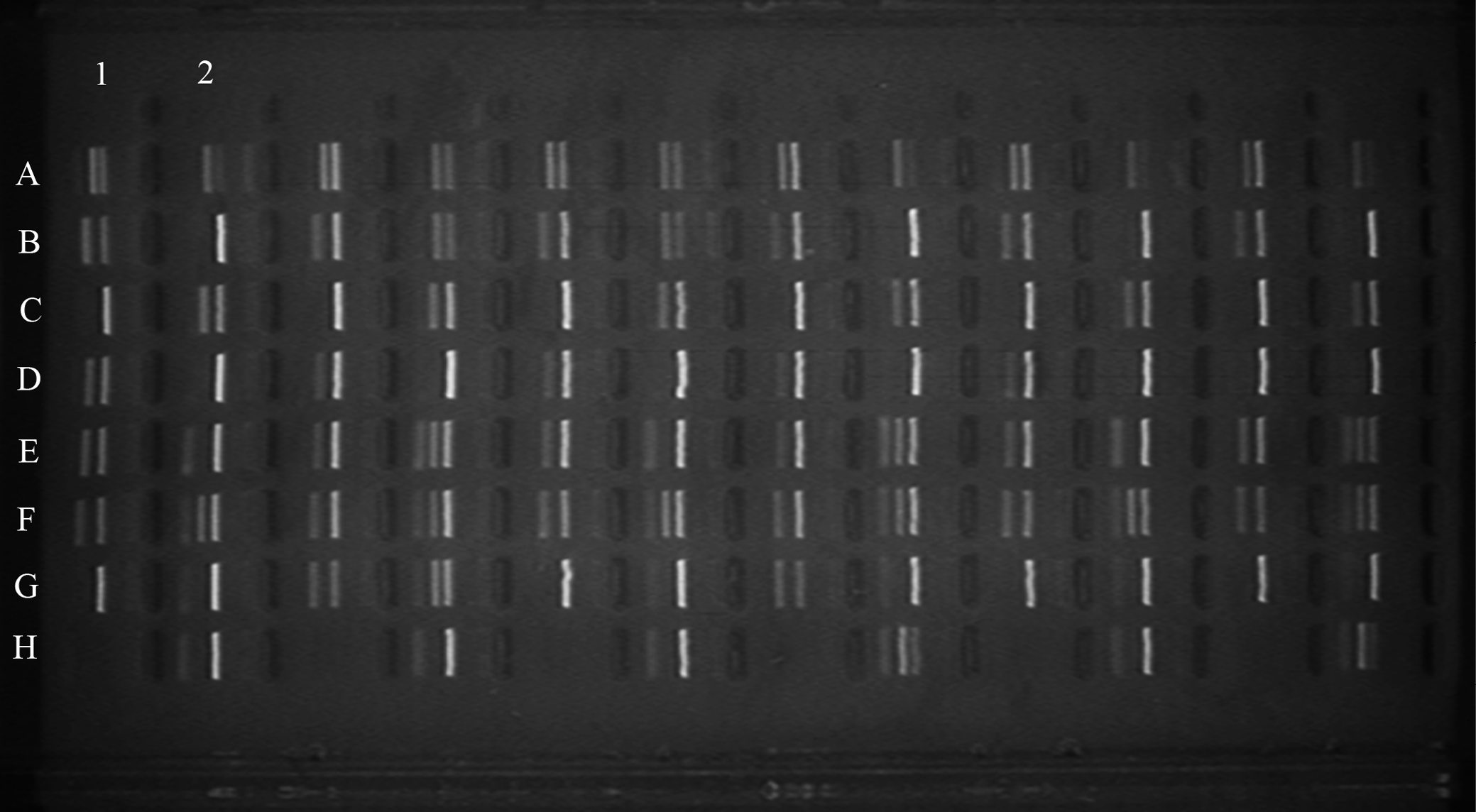
The HRM-PCR analysis effectively distinguished the polymorphism of TNF-α (–308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes. Figure 1 shows the curves of melting profiles of normalized data of TNF-α (–308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes, and distinguishable inferences between the 3 genotypes are clearly observable. Using specified post-melting parameters, all the cytokine variants from the LTRs and the control were identified. To confirm the accuracy of the HRM-PCR assays, we detected the cytokine SNPs of 100 LTRs samples with the SSP-PCR method, using a commercial kit (One Lambda) (Figure 2). When analyzing the data of these 100 specimens, we found a 100% concordance between the HRM-PCR analysis and the SSP-PCR assay for the abovementioned cytokine SNPs, with a Kappa test value of 1.0 (data not shown).
Distribution of cytokine genotype in LTRs of different age and gender group
Because there are differences in gender and age composition between the LTRs and the control group, it may lead to differences in cytokine genotype distribution. Therefore, we analyzed the distribution of LTRs cytokine genotypes in different gender and age groups. The data show that there are no differences in genotype distribution of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) between the male and female patients (χ2 test: χ2 = 0.04, p = 0.841; χ2 = 4.37, p = 0.112; χ2 = 3.0, p = 0.223; χ2 = 3.0, p = 0.223; χ2 = 0.67, p = 0.412; χ2 = 5.80, p = 0.055, respectively, at degrees of freedom (df) = 1, 2, 2, 2, 1, and 2, respectively). The data also show that there are no differences in genotype distribution of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) between ≤30, 31–45, 46–60, and ≥61 years groups (χ2 test: χ2 = 1.90, p = 0.594; χ2 = 3.96, p = 0.681; χ2 = 7.87, p = 0.247; χ2 = 7.87, p = 0.247; χ2 = 4.60, p = 0.203; χ2 = 3.49, p = 0.321, respectively, at df = 3, 6, 6, 6, 3, and 6, respectively). The data confirm that the differences in gender and age composition do not lead to differences in cytokine genotype distribution.
Alleles and genotypes distribution of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A,
−819 T/C and −1082 G/A), and IFN-γ
(+874 T/A) in LTRs and the control subjects
Figure 3A and 3B show the allele and genotype frequencies distribution of selective cytokine in LTRs and control subjects. The data show that there are no significant differences in the allele and genotype distribution of cytokine between the LTRs and the control subjects. As shown in Table 3, the genotype frequency of TNF-α −308 associated with low expression phenotype among LTRs is prevalent with 87.27%. For TGF-β1, combined effect of codon 10 (+869) and codon 25 (+915) determine the protein production. In Chinese population, we found that the genotype frequency of G/G at position −915 was predominant with 98%, which was obtained from the genotyping results of 100 samples using the SSP-PCR method. Therefore, we hypothesized that all LTRs had G/G genotype at position −915 and found that the genotypes associated with high expression phenotype were prevalent with 75.46%. On the contrary, as for IL-10 and IFN-γ, the genotypes associated with low expression phenotype were most prevalent in the LTRs with 87.89% and 78.26%, respectively.
Distribution of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) polymorphisms in LTRs with pulmonary fibrosis, idiopathic pulmonary fibrosis and chronic obstructive pulmonary disease as primary disease
In present study, most of the primary diseases leading to lung transplantation were pulmonary fibrosis (83/322, 25.78%), followed by idiopathic pulmonary fibrosis (IPF; 66/322, 20.50%) and chronic obstructive pulmonary disease (COPD; 53/322, 16.46%). To investigate whether cytokine gene polymorphisms are associated with these diseases, we compared the distribution of cytokine polymorphisms between pulmonary fibrosis, IPF and COPD groups with normal control. The data show that there are no significant differences in the allele and genotype distribution of cytokine between the 3 disease groups and the control subjects (data not shown).
Allele frequencies of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes in Chinese compared with other populations
Allele frequencies of these cytokine polymorphisms in control individuals were compared to those reported in other healthy populations, including Slovak,21 Greek Cypriot,22 Macedonian,23 Lebanese,24 Iran,25 Brazilian,26 Mexican,27 and Thai28 populations (as shown in Table 4). The data show that the distribution of TNF-α −308 A/G polymorphism is similar in Chinese, Greek Cypriot, Lebanese, and Mexican populations, but the frequencies of TNF-α −308 A allele in Slovak, Macedonians, Iran, Brazilian, and Thai populations are higher than those in the Chinese population. For TGF-β1 at position +869, the allele frequencies of T in Lebanese and Brazilian populations increased significantly compared to those in the Chinese population, but decreased in the Thai population. As for IL-10 at positions −592, −819 and −1082, frequencies of the less common allele are high in Slovak, Greek Cypriot, Macedonian, Lebanese, Iran, Brazilian, and Mexican populations compared to those in the Chinese population, and they are similar in Chinese and Thai populations. Besides, the frequency of the less common T allele of IFN-γ +874 is lower in the Chinese population than those in Slovak, Greek Cypriot, Lebanese, Brazilian, and Thai populations.
Discussion
Several SNP genotyping methods vary in terms of detection system, reaction format and allelic discrimination. However, the conventional methods for detecting cytokine SNP are time-consuming and potentially more expensive. Cytokine research urgently requires a low-cost and high-throughput genotyping technique. Therefore, we decided to develop an economic and time-, labor- and cost-saving analysis system to genotype TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) polymorphisms.
The HRM-PCR analysis is a recently developed genotyping method, based on the characteristics of the amplicon thermal denaturation. The HRM-PCR method involves the PCR analysis of the target gene in the presence of a saturating intercalating double-stranded DNA fluorescent dye, and subsequent melting of the amplicon by gradually increasing the temperature, which results in a decrease in fluorescence caused by the release of intercalating dyes from DNA. The specific melting profile depends on the base composition, DNA sequence and amplicon length.29, 30 The HRM-PCR analysis is highly suitable for the detection of single-base variants, deletions or insertions.31 In addition, HRM-PCR method offers several advantages over other conventional gene scanning methods, such as no post-PCR processing steps, complete closed tube format and short turnaround time.32, 33 Thus, it is an attractive technique due to the increased demand for rapid, economic, easy, and high-throughput genotyping analyses. Here, we have presented the HRM-PCR assay to identify cytokine SNPs. The data show that the differences between the 3 allelic forms of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) genes are distinguishable as a result of the melting curve shape. To confirm the accuracy of the HRM-PCR assay, we randomly selected 100 samples from the LTRs and detected cytokine SNPs with the SSP-PCR method using a commercial kit. The data showed a 100% concordance between the HRM-PCR and the SSP-PCR assays for cytokine SNPs, with a Kappa test value of 1.0. All of these suggest that the HRM-PCR assay is a reliable single-tube technology for genotyping the polymorphisms of the abovementioned cytokines. In addition, HRM-PCR assay can genotype 96 samples in 1.5 h on our platform. Therefore, HRM-PCR may be a good choice for cytokines genotyping, as it is a high-throughput, cheap and time-saving method with the further advantage of no post-PCR handling.
Proinflammatory and anti-inflammatory cytokine networks lead to different responses to infection, graft tolerance or rejection. In particular, high levels of pro-inflammatory TNF-α and IFN-γ enhance cell-mediated immune response, causing allograft rejection.34, 35 In contrast, high levels of anti-inflammatory IL-10 suppress the inflammation and are associated with tolerance.36 Besides, high levels of TGF-β1 with immunosuppressive properties are thought to contribute to the development of chronic allograft nephropathy.37 The SNPs of cytokine genes mainly influence the production of proteins, which determines the microenvironment of the graft.38, 39 Pretransplant genetic testing of cytokine may provide a clinically useful means for risk stratification in solid organ transplant patients. In the present study, we explored the profiles of TNF-α (−308 A/G), TGF-β1 (+869 T/C), IL-10 (−592 C/A, −819 T/C and −1082 G/A), and IFN-γ (+874 T/A) SNPs in the LTRs and the control group. Our results show that there are no significant differences in the allele and genotype distribution of cytokines between the LTRs and control groups. In addition, we found that the genotypes of TGF-β1 +869 associated with high expression phenotype were prevalent among LTRs. On the contrary, as for TNF-α −308, IL-10 and IFN-γ, the genotypes associated with low expression phenotype are the most prevalent in the LTRs.
The allelic frequency of a particular gene may vary significantly in different ethnic populations. Previous studies have showed the associations between ethnicity and cytokine gene polymorphisms.20, 27 In the present work, we compared the control results of cytokine gene polymorphisms with those from other national populations. We found dramatic differences in allele frequency of cytokine among different races. The data showed that there were 5, 3, 7, and 5 differences in the allele frequencies of TNF-α −308, TGF-β1 +869, IL-10 (−592, −819 and −1082), and IFN-γ +874 between Chinese and other 8 national populations, respectively. The differences in cytokine allelic frequencies can lead to diverse secretory profiles, responses to stimuli or susceptibility to diseases. Therefore, the studies on distribution of cytokine gene polymorphisms within populations may be helpful in understanding the observed differences in cytokine secretion profiles, which are the basis for various immunological phenomena, such as infectious, autoimmune disorders and transplant rejections. Therefore, we also explored the association between the cytokine polymorphisms and top 3 of the primary diseases leading to lung transplantation. However, we did not find a significant correlation between the cytokine polymorphisms and pulmonary fibrosis, IPF or COPD.
Limitations
The limitations of this study should be mentioned. Firstly, the HRM technology for detecting the SNP of cytokine may not be applicable to other fluorescent PCR instruments. Secondly, in view of the limited sample size and due to the fact that the sample is limited to the Chinese population only, the conclusions may not be applied to other ethnic populations, due to the genetic differences in race.
Conclusions
In conclusion, this study presents a rapid, low-cost and high-throughput HRM-PCR technology for genotyping TNF-α, TGF-β1, IL-10, and IFN-γ genes. It can be widely adopted in diagnostic laboratories to facilitate cytokine gene SNP screening. Moreover, our study profiles the cytokine secretion patterns in the LTRs in Chinese population, which may be utilized in optimizing drug use and improving the prognosis of LTRs.