Abstract
The increasing digitalization of health systems has transformed the ways in which individuals and communities interact with information, health services, and decisions related to their wellbeing. In this context, health literacy, media health literacy, and the digital divide in health have emerged as critical determinants of informed and equitable participation in digital environments. The aim of this conceptual review is to examine the interconnections between health literacy, media health literacy, and the digital divide, and to propose an integrated conceptual framework to inform equitable public health practice, policy, and research in the digital era. The article provides a critical and integrated analysis of these constructs, highlighting their conceptual relationships, key methodological challenges, and implications for clinical practice, health policy development, and public health research. The findings indicate that approaches focused exclusively on individual skill development are insufficient to address digital health inequities. Without attention to structural and organizational determinants, the expansion of health technologies may reproduce or exacerbate pre-existing social and health inequalities. Accordingly, the review underscores the need for multilevel approaches that align literacy development, digital inclusion, and health system design to strengthen equity in the digital era.
Key words: health equity, health literacy, digital health, digital divide, media literacy
Introduction
The digital transformation of health systems has positioned information and technology at the core of healthcare delivery, disease prevention, and health promotion. Within this context, 3 constructs are essential for understanding both the opportunities and risks associated with this transformation: health literacy, media health literacy, and the digital divide in health.1, 2
Health literacy has become established as a key determinant of healthcare quality and health outcomes. In contrast, media health literacy has become increasingly relevant in light of the rapid spread of health misinformation in digital environments.3, 4 In parallel, the digital divide in health highlights how unequal access to technologies, skills, and the benefits of digitalization may reproduce or even amplify pre-existing social and health inequalities.5, 6
Available evidence from cross-sectional studies indicates that a substantial proportion of healthcare professionals lack specific training in these domains, thereby limiting their ability to tailor communication, identify comprehension barriers, or anticipate instances of digital exclusion.7, 8 Similarly, health-related digital and media competencies among the general population and vulnerable groups remain heterogeneous and, in many cases, insufficient.9, 10 For this reason, integrating these concepts into clinical practice, public health, and professional education represents a strategic necessity for advancing more equitable health systems. However, persistent conceptual gaps and methodological tensions remain within the health literacy literature and warrant explicit examination. Notably, there is no universal consensus on its definition or the dimensions it should encompass, such as functional skills vs critical and contextual competencies, which complicates cross-study comparisons and the validation of measurement tools. This misalignment illustrates how existing definitions often fail to correspond with the instruments used in current research, thereby generating a gap between theory and practice.11
Moreover, although a growing body of interventions has been developed to improve health literacy, systematic reviews report substantial methodological heterogeneity and mixed effects, with outcomes that are not consistently statistically significant or transferable across population contexts.12 Consequently, several key analytical questions must be addressed. Where do current interventions fail to achieve sustainable improvements in literacy and health behaviors across diverse settings? What unexamined assumptions, such as the belief that increasing information automatically leads to better decision-making, underpin these programs?
This critical examination is particularly relevant when contrasting approaches that conceptualize health literacy as an isolated individual skill with broader perspectives that view health, media, and organizational literacy as emerging from interactions among individuals, health systems, and structurally shaped social environments.1 This conceptual review critically examines the interconnections among health literacy, media health literacy, and the digital divide and proposes an integrated conceptual framework to inform equitable public health practice, policy, and research in the digital era. Throughout this review, it is important to distinguish between empirically established findings and interpretative or conceptual contributions, particularly given the heterogeneity of the available evidence.
To achieve the study objective, a conceptual narrative review was conducted using a structured literature search strategy to enhance transparency and comprehensiveness. The search was performed in 2 major databases (PubMed and Scopus). The time frame covered publications from 2000 to 2025, encompassing both the initial conceptual development of health literacy and its more recent evolution in relation to digitalization and media environments.
The search strategy combined key terms such as “health literacy,” “media literacy,” “digital divide,” and “digital health literacy,” using Boolean operators to maximize sensitivity. Inclusion criteria comprised peer-reviewed articles, including systematic and scoping reviews, and empirical studies that made relevant conceptual, theoretical, or evidence-based contributions to the 3 domains examined. Non-peer-reviewed publications, opinion papers without a clear methodological basis, and studies not directly related to the health context were excluded.
The selection process involved an initial screening of titles and abstracts, followed by a full-text review of potentially relevant articles. Priority was given to studies that contributed to conceptual clarification, addressed multilevel determinants (individual, organizational, and structural), or provided evidence on interventions and outcomes related to health literacy and digital inequalities.
Although a formal systematic review protocol was not applied, this structured approach was adopted to improve transparency, reproducibility, and analytical rigor, in line with the study’s integrative and conceptual nature.
Objectives
The primary objective of this conceptual review is to provide conceptual clarification and examine the interconnections among health literacy, media health literacy, and the digital divide. By establishing the boundaries and overlaps of these constructs, this study aims to:
1. Consolidate a multidimensional understanding of these concepts that moves beyond individual skills to include structural and organizational factors;
2. Develop an integrated conceptual framework that shows how these domains interact to shape equity in digital health systems;
3. Identify systemic barriers where the lack of integrated literacy and access reinforces health inequalities.
Health literacy
Health literacy is defined as the set of cognitive and social skills that enable individuals to access, understand, evaluate, and use health information to make well-informed decisions and take action regarding their health.2, 13 Since its recognition as a public health issue at the beginning of the 21st century, the concept has evolved from a perspective focused exclusively on reading comprehension toward a multidimensional approach that integrates individual, social, and contextual factors.14 Accordingly, in 2025, the World Health Organization (WHO) updated its definition of health literacy as “the knowledge and competencies that people accumulate through their daily activities, social interactions, and intergenerational experiences to access, understand, evaluate, and use health information and services in ways that promote and maintain their own health and wellbeing, as well as that of their communities.” This approach recognizes that health literacy depends not only on individual reading and comprehension skills but also on the availability of resources, structures, and institutional systems that facilitate access to understandable and reliable information. The WHO emphasizes that improving health literacy is essential for empowering individuals to make informed decisions, fostering collective participation in health promotion efforts, and reducing health inequalities, as insufficient health literacy may reinforce existing social gaps.15
Numerous studies have shown that low health literacy is consistently associated with poorer clinical outcomes, lower therapeutic adherence, increased use of emergency services, more frequent hospitalizations, and higher healthcare costs.16, 17 These associations are observed even among individuals with high levels of formal education, particularly in situations involving stress, acute illness, or therapeutic complexity.18 Health literacy is not evenly distributed across the population. Factors such as older age, lower educational attainment, limited income, membership in ethnic or cultural minority groups, and limited proficiency in the dominant language are associated with a higher likelihood of inadequate health literacy.19 These disparities reflect the influence of social and structural determinants that shape access to understandable information and appropriately tailored healthcare services.20
In this regard, health literacy cannot be understood solely as an individual responsibility. The concept of organizational health literacy emphasizes the role of healthcare institutions in creating environments that facilitate understanding, navigation of the system, and informed decision-making.21, 22 Available evidence indicates that, in many cases, the communicative and administrative demands imposed by healthcare organizations exceed the average skill level of the population, thereby reinforcing the need for institutional-level interventions.23
Strategies to improve health literacy include educational interventions across the life course, culturally adapted community-based programs, and targeted training for healthcare professionals in clear and person-centered communication.24, 25 Systematic assessment of health literacy further enables the identification of specific needs and informs policies and programs aimed at reducing health inequalities.26
Despite their widespread adoption, dominant models of health literacy, such as the conceptual framework and measurement instruments derived from the European Health Literacy Survey (HLS-EU), have faced substantive criticism in the scientific literature, particularly for their focus on self-reported individual skills. Although these models have been widely adopted, several authors argue that they tend to operationalize health literacy primarily through self-reported individual skills, which may obscure the influence of structural, organizational, and political factors shaping the understanding and use of health information.14 In addition, this approach has been criticized for potentially contributing, albeit unintentionally, to the medicalization of everyday life and to the excessive individualization of responsibility for health-related decisions and outcomes. Such framing may shift attention away from health system limitations toward presumed individual deficits in competencies.27, 28 From a critical perspective, measuring and attempting to “correct” health literacy without questioning message complexity, service navigability, or power asymmetries in clinical communication may reinforce existing inequities rather than reduce them. This concern underscores the need to integrate organizational and structural approaches into the assessment and promotion of health literacy.29
Media health literacy
Media health literacy refers to the competencies required to access, analyze, critically evaluate, and use health-related information originating from both traditional and digital media sources.1 In an environment characterized by information overload and the rapid dissemination of content through social media, this competence has become an essential component of contemporary health literacy.30 Media health literacy involves understanding the social, economic, and ideological contexts in which media messages are produced, identifying underlying commercial or political interests, and assessing the credibility of information sources.31 These skills are fundamental for distinguishing reliable health information from misleading or explicitly false content, the proliferation of which has been widely documented, particularly during recent public health crises.3, 4
Evidence indicates a positive association between media literacy and health literacy, suggesting that developing media-related competencies may strengthen individuals’ ability to process and appropriately use health information.31 However, numerous studies show that a substantial proportion of the population has not received formal media literacy training, which limits their capacity to engage critically with available health information.30 Educational interventions in media health literacy have shown promising results, particularly when implemented within formal educational settings or public health programs targeting young people and other vulnerable groups.32 Such interventions may enhance the ability to evaluate the credibility of information, reduce susceptibility to misinformation, and promote responsible health information-seeking and use behaviors.33
Despite its relevance, media health literacy faces important limitations in countering highly emotional health misinformation. Empirical studies suggest that content appealing to fear, anger, or group identity can influence health beliefs, although the magnitude of this effect varies across contexts and populations.34, 35 Recent studies indicate that individual critical capacity alone is not always sufficient to offset the persistence and impact of false information when it is repeatedly disseminated and socially reinforced in digital environments, particularly during public health crises.4 In this context, several authors emphasize the need to move beyond exclusively individual-centered approaches and to incorporate analyses of the structural role of digital platforms. Emerging evidence suggests that recommendation algorithms and attention-based models may amplify polarizing or misleading health content, although this remains an area of ongoing research.36 Recognizing these platforms as active actors in shaping the information ecosystem is essential to understanding why media literacy, if not accompanied by regulation, responsible design, and public policy interventions, may have limited impact in effectively reducing health misinformation.
Digital divide in health
The digital divide in health is defined as the set of inequalities in access to, competencies related to, and benefits derived from the use of digital technologies applied to health.5, 15 This divide represents a specific manifestation of the broader digital divide and constitutes a central challenge to equity, effectiveness, and justice in contemporary health systems.6 Access-related inequalities include the availability of devices, internet connectivity, and the quality of technological infrastructure. These factors disproportionately affect individuals with lower income, residents of rural areas, and certain social groups.5, 15 However, access alone does not guarantee the effective use of digital health technologies.37
The competency dimension of the digital divide refers to the skills required to use digital technologies autonomously and critically, including the ability to search for, evaluate, and apply health information in digital environments.38 Deficits in these competencies may limit the use of services such as telemedicine, patient portals, or mobile health applications, with direct consequences for participation and health outcomes.9 Finally, the digital divide in health is also reflected in the unequal distribution of the benefits generated by digitalization. Individuals with higher levels of education and greater resources tend to benefit more from digital innovations, while vulnerable groups face a heightened risk of exclusion, thereby widening existing inequalities.32
Analyzing the digital divide in health requires explicit consideration of the role of public policies on digital health. Available evidence suggests that the expansion of health technologies, in the absence of inclusive policies, may reinforce pre-existing inequalities.39 Several studies caution that many national digital health strategies have prioritized technological innovation and system efficiency while paying comparatively less attention to equity, community participation, and adaptation to local sociocultural contexts.
In this regard, scholars have highlighted the risks of promoting so-called universal technological solutions, such as standardized telemedicine platforms or mobile health applications, that assume homogeneous conditions of access, digital skills, and institutional trust. Such assumptions often overlook the realities of rural populations, older adults, and socially vulnerable groups.40 The literature has emphasized that without context-sensitive approaches and co-design with end users, digital health policies may generate new forms of exclusion and further deepen the digital divide in health, underscoring the need for digital governance frameworks explicitly oriented toward equity.41
Interconnections between health literacy, media health literacy, and the digital divide
Health literacy, media health literacy, and the digital divide interact dynamically and together shape an integrated conceptual framework. At their intersection emerges the concept of digital health literacy, understood as the capacity to access, understand, evaluate, and use health information and services in digital environments in a critical and goal-oriented manner.1, 42
Digital health literacy integrates health, digital, and media-related competencies and is essential for equitable participation in increasingly digitalized health systems.9, 10 Evidence indicates that, even in contexts with high levels of technological penetration, difficulties in identifying reliable health information and resisting misinformation persist. This finding underscores the need for integrated approaches rather than isolated interventions.4
The digital divide further shapes the development of these forms of literacy, as limitations in access or competencies restrict opportunities for learning and the effective use of digital health resources. Addressing these 3 domains in isolation is therefore insufficient. A holistic approach that explicitly recognizes their interdependence is required.6
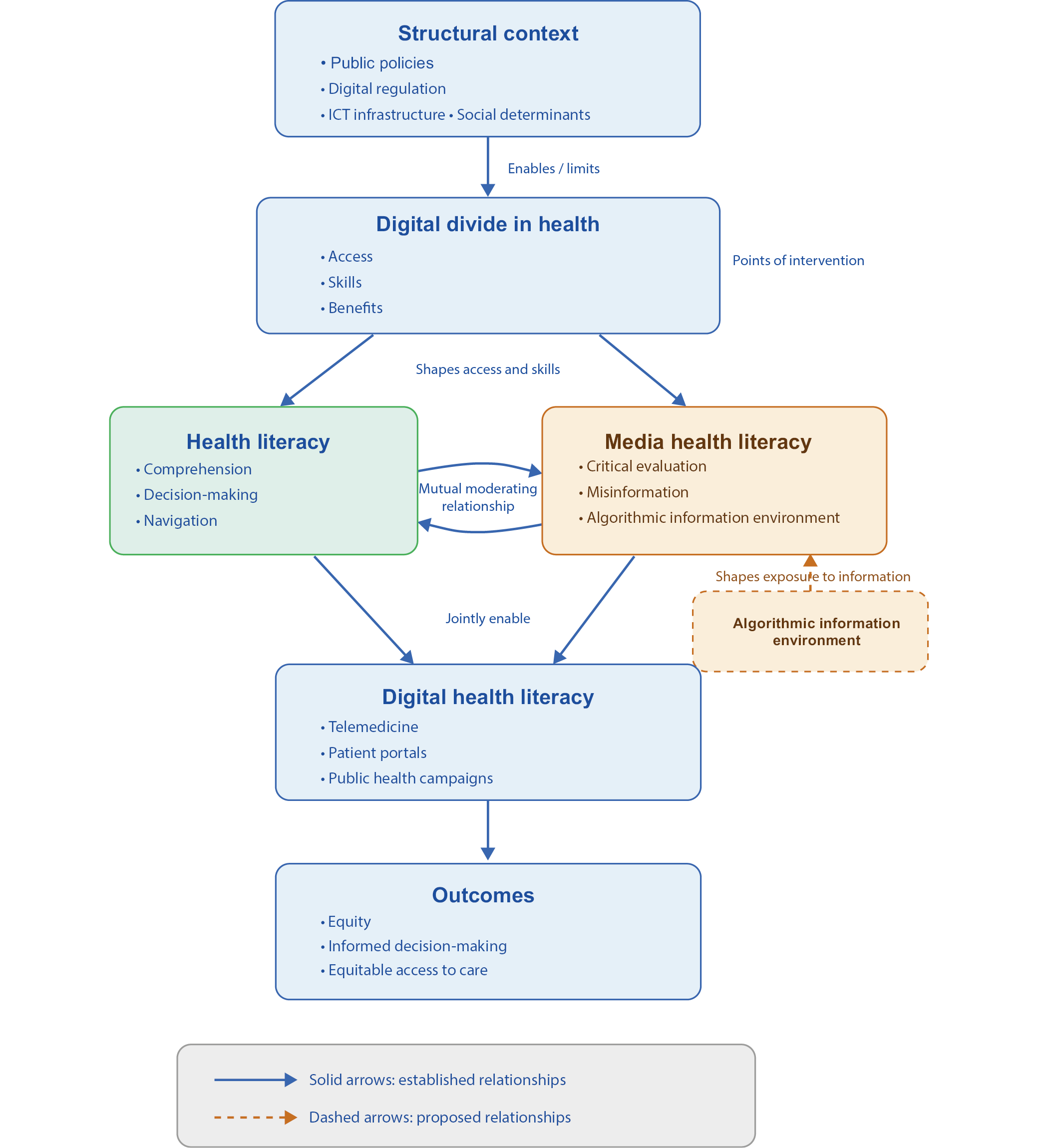
The interrelationship between health literacy, media health literacy, and the digital divide becomes particularly evident in concrete digital health applications such as telemedicine, patient portals, and digital public health campaigns. Evidence suggests that the effective use of telemedicine depends not only on technological access but also on users’ ability to understand clinical instructions, assess the reliability of information received, and navigate digital platforms. These competencies are closely linked to both health literacy and media literacy.40 Similarly, studies on patient portals indicate that individuals with lower levels of digital health literacy experience greater difficulties in interpreting test results, communicating with healthcare professionals, and benefiting from these tools. If not designed inclusively, such systems may contribute to widening health inequities.43 In the context of digital public health campaigns, research has shown that exposure to health messages on social media requires media literacy skills to distinguish reliable information from misinformation, particularly in emotionally charged contexts.44, 45 Taken together, these examples reinforce the need to incorporate a visual conceptual model that synthesizes the dynamic interrelations among individual competencies, digital media environments, and structural access conditions. Such a model facilitates understanding of how these dimensions converge to shape participation and equity in digitalized health systems.14 Figure 1 presents an integrated conceptual model illustrating the dynamic interactions among health literacy, media health literacy, and the digital divide, and their implications for public policy and clinical practice in digital health systems. Beyond synthesizing existing literature, the proposed conceptual model introduces several novel contributions. First, it explicitly integrates 3 analytical levels – structural, competency-based, and systemic – that are typically addressed in a fragmented manner. Second, it incorporates the roles of digital platforms and algorithmic dynamics as active determinants that shape the health information environment, moving beyond approaches focused solely on individual competencies. Third, the model proposes explicit conceptual relationships between literacy, access, and health outcomes, enabling the formulation of empirically testable hypotheses. Specifically, the framework suggests that: 1) media health literacy may moderate the impact of misinformation on health beliefs and behaviors; 2) digital access conditions influence the development and distribution of digital health competencies; and 3) structural and organizational interventions may have greater potential to reduce inequalities than interventions focused exclusively on individuals.
These contributions enhance the model’s explanatory and operational value and open new avenues for applied research and policy evaluation. In this context, although numerous studies highlight the positive role of digital health literacy in promoting informed health behaviors, others report limited effectiveness when structural and organizational conditions are unfavorable. Some evidence suggests that improvements in individual competencies do not always translate into equitable health outcomes, revealing tensions between observed gains and the persistence of inequalities.
Furthermore, evidence on the interaction between algorithmic content curation and health literacy remains limited, highlighting important gaps in understanding how digital platforms may amplify or mitigate health inequalities. These findings reinforce the need to consider both individual competencies and systemic determinants and underscore the importance of future empirical research to test the pathways proposed in the integrated multilevel model.
Targeted interventions
Available evidence from systematic reviews suggests that interventions aimed at improving health and digital health literacy show variable effectiveness, depending on population characteristics and implementation settings. This variability underscores the need to clearly distinguish among individual, community, organizational, and systemic interventions. Interventions designed to improve health literacy and digital health literacy tend to be more effective when targeted at individuals and groups with low baseline competency levels.46 Recent evidence indicates that tailored educational programs can produce significant improvements in knowledge, skills, and health-related digital behaviors, particularly among vulnerable populations.47 At the individual level, educational programs focused on enhancing knowledge and skills show modest positive effects, especially among populations with lower initial literacy levels. However, their impact is often limited when not accompanied by changes in the informational and care environments.14, 46 Among the most promising strategies are multicomponent community-based interventions, targeted training for vulnerable groups, inclusive design of digital health services, and capacity building for healthcare professionals in clear communication and equitable use of digital technologies.48, 49 It is also essential to incorporate rigorous evaluation and long-term follow-up to ensure that these interventions do not generate new forms of inequity.50, 51 Community-based interventions, particularly those that are culturally adapted and co-designed with participants, have demonstrated greater effectiveness in reducing access barriers, strengthening trust, and promoting more critical engagement with health information. These effects are especially evident among vulnerable and marginalized populations.26 At the organizational level, the adoption of organizational health literacy principles, such as process simplification, inclusive design of digital services, and professional training in clear communication, is associated with more sustained improvements in comprehension, system navigation, and patient participation.21
Finally, systemic interventions, including public policies on connectivity, regulation of digital platforms, and national digital health strategies with an explicit equity focus, are essential for creating the structural conditions that allow lower-level interventions to be effective and not solely dependent on individual capacities.41 The literature, however, cautions that poorly designed interventions or those implemented without an equity impact assessment may exacerbate inequalities by disproportionately benefiting individuals with greater educational and digital resources. This phenomenon has been described as the amplification of advantage in digital health contexts.40 Accordingly, identifying what works, for whom, and under what conditions emerges as a central principle in designing effective and equitable interventions in the era of health system digitalization. Overall, the evidence remains heterogeneous, and the findings should be interpreted with caution given variations in study design, population, and outcome measures.
Table 11, 5, 21, 23, 25, 26, 39, 45, 46, 48, 49, 52 highlights the risk associated with the so-called digital inverse care law, which posits that those who stand to benefit most from digital health innovations are often the least likely to access or use them effectively.40, 41, 52, 53 This phenomenon arises when digital interventions are implemented without consideration of pre-existing inequalities in literacy, access, institutional trust, and social conditions, thereby amplifying advantage among groups with higher levels of digital and educational capital. These dynamics reinforce the need for multilevel, context-sensitive approaches, as interventions focused exclusively on individuals are not only insufficient but may also inadvertently deepen digital health inequities.
To facilitate understanding and comparison of interventions addressing health literacy and digital health, we provide a structured synthesis organized by intervention level (individual, community, organizational, and systemic/policy), highlighting key components, target populations, evaluation indicators, and associated risks. This structure enables linking each type of intervention to relevant empirical or conceptual evidence, showing how actions aimed at strengthening individual competencies, community engagement, organizational health literacy, and public policy may help reduce inequalities in access to and use of digital health tools. The selected indicators, such as improvements in digital competencies, patient understanding, community participation, and reductions in access gaps, support the assessment of effectiveness, while the identification of risks and limitations underscores the importance of structural and contextual conditions for sustaining outcomes. Table 11, 5, 21, 23, 25, 26, 39, 45, 46, 48, 49, 52 summarizes these interventions together with key references supporting their implementation and effectiveness.
Implications for practice and policy
Advancing toward equitable digital health systems requires that health literacy, media health literacy, and the reduction of the digital divide move beyond theoretical constructs and become operational priorities.14, 39
At the policy level, decision-makers should conduct digital equity impact assessments before deploying new technologies, avoiding one-size-fits-all solutions that disregard local contexts. Regulatory frameworks should promote transparency in health-related algorithms and ensure equitable access to digital infrastructure, particularly in underserved areas.39
In clinical practice, healthcare professionals require specific training not only in using digital tools but also in clear digital communication strategies. For example, the systematic use of the teach-back method in teleconsultations can help ensure patient understanding.46 Additionally, prescribing trusted digital resources may help patients navigate health information and reduce exposure to misinformation.1
At the organizational level, healthcare institutions should conduct usability and navigability audits of digital platforms to ensure accessibility for individuals with low levels of health literacy.21 The introduction of dedicated roles among healthcare professionals to support vulnerable patients in using digital health services may further reduce exclusion and improve equitable access.23
Implications for research
Future research should move beyond traditional approaches that focus exclusively on individual competencies and adopt a more integrated, systemic perspective.1 From an equity-oriented standpoint, studies should not only assess whether a digital intervention is effective, but also identify which strategies work, for whom, and under which implementation conditions, taking into account literacy levels and socioeconomic context.46
Participatory and mixed-methods approaches should be prioritized, particularly those involving vulnerable populations in the co-design of digital tools and services. These approaches may help ensure that proposed solutions address real structural barriers rather than only technical usability criteria.23 In addition, future research should examine more closely how the power dynamics of digital platforms and their algorithms shape the production, circulation, and consumption of health information, as well as how current regulatory frameworks may affect patient autonomy and health equity.39
Limitations of the study
This conceptual review presents several limitations to consider when interpreting its findings. First, although a structured search strategy was applied, the selection of studies does not guarantee exhaustive coverage of the literature. Second, although all included publications were peer-reviewed, no formal methodological quality assessment was conducted, limiting the ability to weigh findings by level of evidence. Finally, the primarily conceptual nature of the review, without direct empirical analysis, limits the generalizability of the conclusions. These limitations highlight the need for future research, including both quantitative and qualitative studies, to empirically test and refine the relationships proposed in this framework.
Conclusions
Health literacy, media health literacy, and the digital divide are deeply interconnected and jointly shape individuals’ ability to navigate health information in digital environments. Addressing these dimensions in isolation is insufficient and may overlook the structural and organizational conditions that influence access to, understanding of, and use of digital health resources. An integrated approach combining individual, community, organizational, and policy-level actions is essential to ensure equitable participation in digital health systems. Without such a perspective, digital transformation risks reproducing or exacerbating existing health inequalities. The proposed conceptual framework provides a foundation for designing and evaluating equity-oriented digital health interventions, contributing to the development of more inclusive and just health systems in the digital era.
Use of AI and AI-assisted technologies
The authors declare that Gen AI was used in the creation of this manuscript. Generative AI was specifically used to assist in translating the manuscript into English, using OpenAI’s ChatGPT. Grammarly AI was used to review grammar and style. The authors take full responsibility for this use.