Abstract
Background. Intracardiac leads commonly produce metal artifacts on computed tomography (CT) images. These artifacts may be reduced using dedicated metal artifact reduction algorithms, such as metal artifact reduction (MAR).
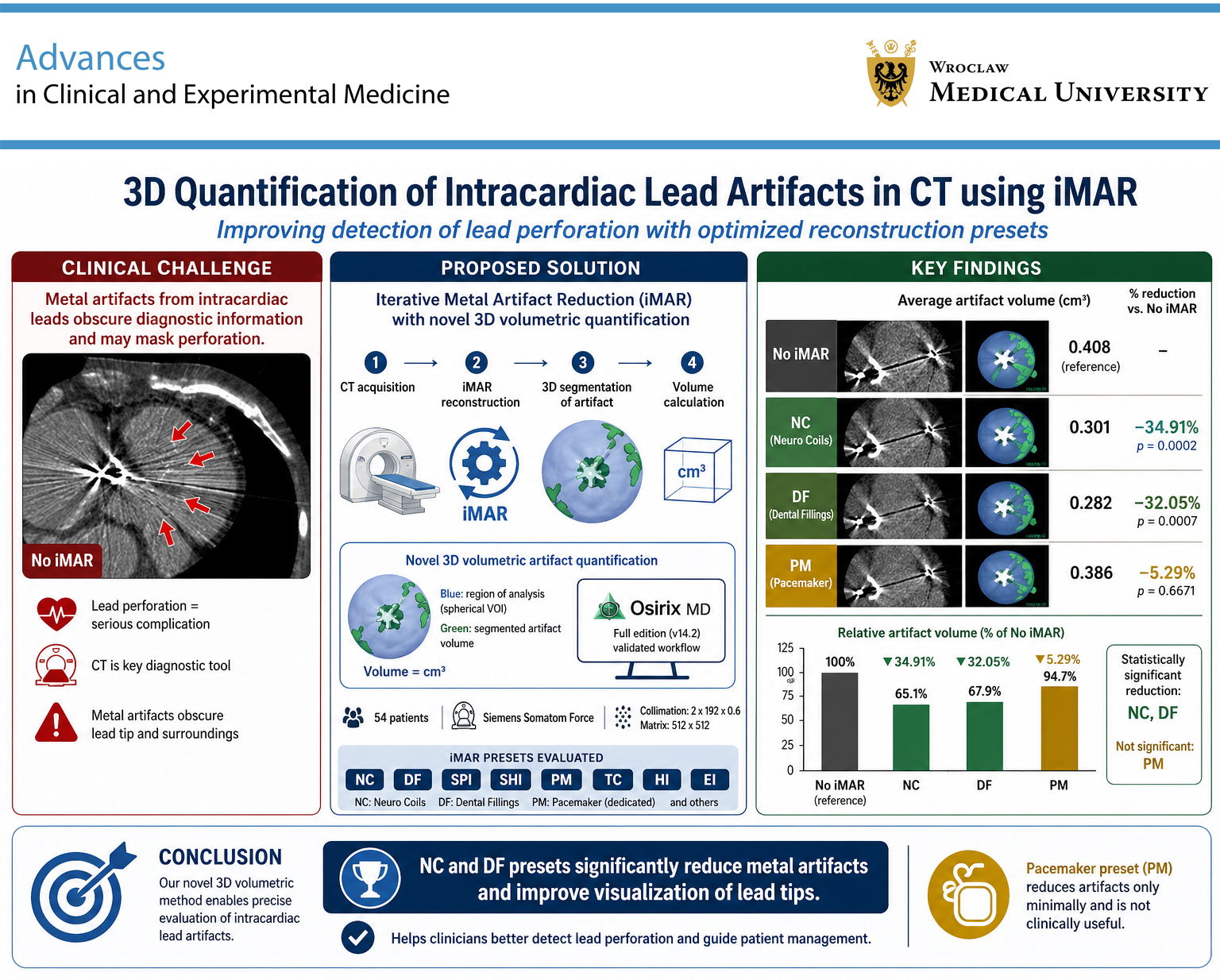
Objectives. The aim of this study was to develop a method for measuring lead-related artifacts in CT and to assess the suitability of various reconstruction presets for lead visualization.
Materials and methods. Fifty-four patients (mean age: 73.9 ±11.32 years) with implanted cardiac implantable electronic devices (CIEDs) who underwent cardiac CT, chest CT, or pulmonary angio-CT were included in the study. Images were reconstructed using at least 2 kernels (soft tissue and lung) with slice thicknesses of 0.6 mm or 1.0 mm. A tissue density volume >1,000 HU, corresponding to the presumed volume of hyperdense artifacts, was isolated within a manually drawn spherical region of interest (ROI), and the values were recorded. The obtained values for each iterative metal artifact reduction (iMAR) reconstruction preset were compared with native images (without iMAR) to calculate the percentage reduction in hyperdense artifacts.
Results. All tested algorithm variants reduced artifact volume; however, only 2 presets achieved statistically significant reductions: “dental fillings” (p = 0.001) and “neuro coils” (p = 0.000). Pacemaker-dedicated presets reduced metal artifacts in all cases, although the reductions were not statistically significant (p = 0.667), which may limit their reliability in routine clinical practice.
Conclusions. We proposed a method for evaluating intracardiac leads that enables precise three-dimensional (3D) assessment of hyperdense artifacts. The metal artifact reduction technique demonstrated promising results, particularly for the “dental fillings” and “neuro coils” presets.
Key words: cardiac implanted electronic devices, metal artifact reduction, artifacts
Background
Cardiac implantable electronic device (CIED) implantation is one of the established methods for the treatment of cardiac arrhythmias and conduction disturbances, most commonly sinus node dysfunction and atrioventricular block.1, 2 Although this therapeutic approach has undergone continuous technological development, it is still associated with a certain risk of complications.3, 4, 5 Due to their structure and mechanism of action, complications most frequently involve the leads. In a Danish study, lead-related interventions (2.4%) were identified as the most common serious complications,6 with lead perforations occurring in 0.3–0.7% of cases. According to the definition, lead perforation occurs when the lead penetrates through the myocardium into the epicardial space, pericardium, or chest wall.7, 8 In the same registry, complications associated with left ventricular (LV) leads reached 4.3%, representing the most frequent lead-related complications. Complications related to right atrial (RA) leads (2.3%) and right ventricular (RV) leads (2.2%) were observed with similar frequency.9 Lead perforation is usually considered a serious complication of electrotherapy procedures. In such cases, electrocardiologists often rely on imaging specialists and radiologists to determine the extent and location of lead perforation. This information is crucial for planning further treatment. Computed tomography (CT) appears to be the most useful imaging modality for this purpose.10, 11, 12 However, intracardiac leads, particularly lead tips, tend to generate metal artifacts on CT images. These artifacts may be reduced using dedicated metal artifact reduction algorithms, such as iMAR (iterative metal artifact reduction). Many CT equipment manufacturers have developed their own artifact reduction algorithms,13, 14 most of which also include additional presets. Clinical experience suggests that dedicated presets do not always provide optimal performance in specific clinical situations. Therefore, the question remains as to which presets are most effective.
Objectives
The aim of this study was to develop a method for measuring lead-related artifacts in CT and to assess the suitability of various reconstruction presets for lead visualization.
Materials and methods
The study was approved by the Ethics Committee of the Medical University of Silesia (Katowice, Poland; approval No. BNW/NWN/0052/KB/68/24) and was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its subsequent amendments. All participants provided informed consent prior to inclusion in the study.
The study population consisted of 54 patients (mean age: 73.9 ±11.32 years) with implanted CIEDs, including implantable cardioverter-defibrillators (ICDs; n = 15) and pacemakers (n = 39), who underwent cardiac CT, chest CT, or pulmonary angio-CT for clinical indications between 2022 and 2023.
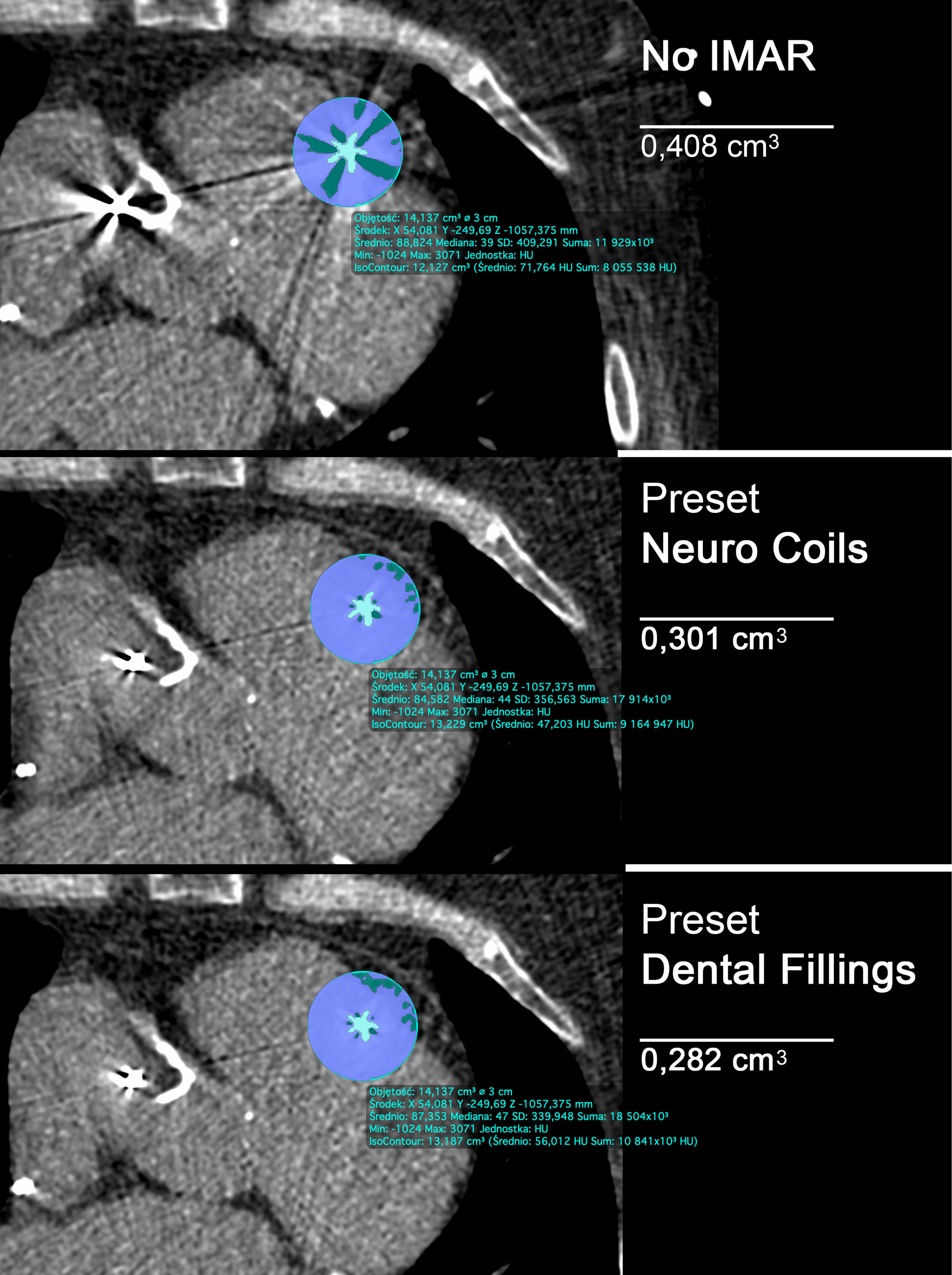
Cardiac and chest CT examinations, both contrast-enhanced and non-contrast-enhanced, were performed for clinical purposes using a Siemens Somatom Force scanner with VB20_SP2 software (Siemens Healthineers, Forchheim, Germany). The collimation was set at 2 × 192 × 0.6 mm using a 512 × 512 matrix. Cardiac CT examinations were performed following intravenous contrast administration and appropriate premedication. Depending on clinical indications, nitroglycerin and/or β-blockers were administered. Scans were acquired at 120 kVp with automatic tube current modulation using the CARE Dose system (Siemens Healthineers) and ECG gating. No intravenous contrast administration or premedication was required for chest CT examinations, which were performed at 120 kVp with automatic tube current modulation. Pulmonary angio-CT examinations were performed following intravenous contrast administration, without premedication, at 120 kVp with automatic tube current modulation. Images were reconstructed using at least 2 kernels (soft tissue and lung) with a slice thickness of 0.6 mm or 1.0 mm. Additionally, iMAR (Siemens Healthineers) reconstructions were generated for each examination using 8 different presets: “spine implants” (SpI), “shoulder implants” (ShI), “pacemaker” (PM), “thoracic coils” (TC), “hip implants” (HI), “extremity implants” (EI), “dental fillings” (DF), and “neuro coils” (NC). Image analysis was performed using syngo.via software v. VB30A_HF06 (Siemens Healthineers) and OsiriX MD software v. 14.2 (Pixmeo SARL, Geneva, Switzerland), both certified for medical imaging applications. A tissue density volume >1,000 HU, corresponding to the presumed volume of hyperdense artifacts, was isolated within a manually drawn spherical region of interest (ROI), and the obtained values were recorded. A spherical ROI with a radius of 15 mm was selected to fully encompass the lead tip and its associated artifacts in the region where accurate assessment of lead tip position is most critical for excluding perforation. In CT imaging, 1,000 HU represents the upper limit of physiological tissue density in adjacent structures, such as the rib cortex, as well as contrast enhancement within the right ventricle (500–600 HU). Therefore, applying a threshold of >1,000 HU ensured exclusion of biological tissues and contrast material from the measurements. The obtained values for each iMAR reconstruction preset were compared with native images (without iMAR) to calculate the percentage reduction in hyperdense artifacts.
Statistical analyses
The obtained data were assessed for distribution normality. As the variables did not follow a normal distribution, the nonparametric Mann–Whitney U test was applied. Data are presented as the median (Me) and the 1st (Q1) and 3rd quartiles (Q3), allowing for characterization of the variable distribution while accounting for asymmetry and minimizing the influence of outliers. The Bonferroni correction was applied to reduce the risk of type I error associated with multiple comparisons. Accordingly, the significance level (α) was adjusted by dividing it by the number of performed comparisons (k). The resulting adjusted significance threshold (α/k), corresponding to p = 0.006, was used as the criterion for statistical significance. Statistical analyses were performed using MedCalc v. 23.5.5 (MedCalc Software, Ostend, Belgium).
Results
Contrast-enhanced examinations were performed in 28 cases, representing 51.8% of the study population. Among the included patients, 72.2% (n = 39) had implanted cardiac resynchronization therapy (CRT) devices, whereas 27.8% (n = 15) had implanted ICDs.
The mean volume of cardiac lead artifacts in native images (without iMAR) and after application of different iMAR presets is presented in Table 1. Lower artifact volumes indicated more effective artifact reduction. The table also includes the percentage reduction in artifact volume achieved with each preset. All tested algorithm variants reduced artifact volume; however, only 2 presets achieved statistically significant reductions: “dental fillings” (p = 0.001) and “neuro coils” (p = 0.000). Representative examples of the graphical analyses are presented in Figure 1. The pacemaker-dedicated preset reduced metal artifacts in all cases; however, the reduction was not statistically significant (p = 0.667), which may limit its reliability in routine clinical practice.
The next step of the analysis was to validate the overall results in specific subgroups. First, the study population was divided according to the type of implanted lead: pacing or defibrillation (ICD). In the subgroup with pacing leads, a statistically significant reduction in artifact volume was observed only for the “neuro coils” preset (Me = 0.206 (Q1 0.143–Q3 0.264)) compared with native images without iMAR (Me = 0.274 (Q1 0.228–Q3 0.444)); p = 0.002.
In the subgroup with defibrillation leads, which are thicker, no statistically significant differences were observed either for the neuro coils preset (Me = 0.317 (Q1 0.246–Q3 0.499)) compared with native images without iMAR (Me = 0.473 (Q1 0.352–Q3 0.840)); p = 0.040, or for the dental fillings preset (Me = 0.320 (Q1 0.226–Q3 0.506)) compared with native images without iMAR (Me = 0.473 (Q1 0.352–Q3 0.840)); p = 0.020. The final step of the analysis involved dividing the study population according to the type of CT examination performed: contrast-enhanced or non-contrast-enhanced. In contrast-enhanced examinations, no statistically significant reduction in artifact volume was observed, including for the neuro coils preset (Me = 0.195 (Q1 0.142–Q3 0.259)) compared with native images without iMAR (Me = 0.302 (Q1 0.229–Q3 0.470)); p = 0.016. In non-contrast-enhanced examinations, statistically significant reductions in artifact volume were observed both for the neuro coils preset (Me = 0.262 (Q1 0.207–Q3 0.381)) compared with native images without iMAR (Me = 0.358 (Q1 0.267–Q3 0.569)); p = 0.005, and for the dental fillings preset (Me = 0.246 (Q1 0.194–Q3 0.340)) compared with native images without iMAR (Me = 0.358 (Q1 0.267–Q3 0.569)); p = 0.005.
Discussion
Computed tomography-based lead analysis represents a valuable diagnostic support tool for clinicians. However, most intracardiac leads generate metal artifacts on CT images, particularly at the lead tip. These artifacts substantially hinder accurate assessment of lead tip position, which is especially important in the diagnosis of lead perforation or microperforation. Numerous factors influence the quality of lead visualization. For example, Reinartz et al. analyzed 400 CT images and demonstrated that a lead-tip angle of 70° was the critical angle at which diagnostic image quality was consistently maintained. They referred to this as the “magic angle” in CT pacemaker imaging.15 Our group has also investigated this issue extensively and demonstrated that the presence of implanted endocardial leads may limit the applicability of coronary CT angiography in patients with implanted antiarrhythmic devices, particularly in the region of the right coronary artery (RCA).16
Most CT scanner manufacturers have introduced dedicated algorithms for reducing lead-related artifacts. Takayanagi et al.17 and Tatsuagmi et al.18 evaluated the SEMAR (single-energy metal artifact reduction) technique and demonstrated that it reduced artifacts and significantly improved coronary lumen assessability. In addition, application of the proposed DyPAR+, a fully automatic Dynamic Pacemaker Artifact Reduction pipeline, in 9 clinical cases with implanted pacemakers resulted in a significant reduction of metal artifacts and demonstrated potential applicability in clinical practice. This method is based on neural network technology.19
Unfortunately, clinical practice indicates that presets developed for specific applications do not always meet expectations. Therefore, we sought to establish a scientific method for their objective evaluation. To achieve this, we proposed a novel method for three-dimensional (3D) localization of the lead tip and isolation of the volume of hyperdense artifacts in the surrounding area. This approach enabled an objective quantitative analysis of artifact intensity, independent of observer-related bias. The use of CT combined with dedicated postprocessing algorithms may reduce the impact of metal artifacts and improve diagnostic image quality in most cases. However, the actual occurrence of such artifacts and the extent of image quality impairment cannot currently be reliably predicted.20
Limitations of the study
To minimize the risk of type I error, the Bonferroni correction was applied. The sample size (n = 16) was not a contraindication to its use, as this correction is related to the number of performed comparisons rather than directly to the number of observations. However, it should be noted that, in small samples, the Bonferroni correction is highly conservative and may increase the risk of type II error, resulting in a failure to detect true differences. This may explain the lack of statistically significant reductions observed for defibrillation leads and contrast-enhanced examinations. Moreover, the present study demonstrated the usefulness of metal artifact reduction algorithms using solutions provided by a single manufacturer (Siemens Healthineers). In our opinion, the performance of dedicated presets should always be evaluated on the specific hardware platform for which they are intended. The proposed method for volumetric artifact analysis appears to be valuable regardless of the manufacturer; however, further studies and methodological refinements are required.
Conclusions
The proposed method for evaluating intracardiac leads enables precise 3D assessment of hyperdense artifacts. Our findings demonstrated that metal artifact reduction techniques provide promising results; however, the dedicated pacemaker preset did not show superior performance. Among the evaluated iMAR presets, “dental fillings” and “neuro coils” appeared to be the most effective options, particularly in cases of suspected lead perforation. No significant differences were observed between pacing and defibrillation leads.
Data Availability Statement
Data sharing is not applicable to this article, as all data are already included in the manuscript.
Consent for publication of personal information
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.