Abstract
Background. The clinicopathological significance and prognostic value of Delta-like ligand 4 (DLL4) expression in gastric cancer (GC) remain controversial. Therefore, we conducted a meta-analysis to ascertain the correlation between DLL4 expression and the clinicopathological features and prognosis of GC patients.
Objectives. To clarify the association between DLL4 expression, clinicopathological parameters, and the prognosis of GC patients, as well as to resolve the existing controversies.
Materials and methods. A systematic retrieval was performed according to the selection criteria. The hazard ratio (HR) or odds ratio (OR) and 95% confidence interval (95% CI) were applied to assess the clinicopathological and prognostic value of DLL4 expression in patients with GC.
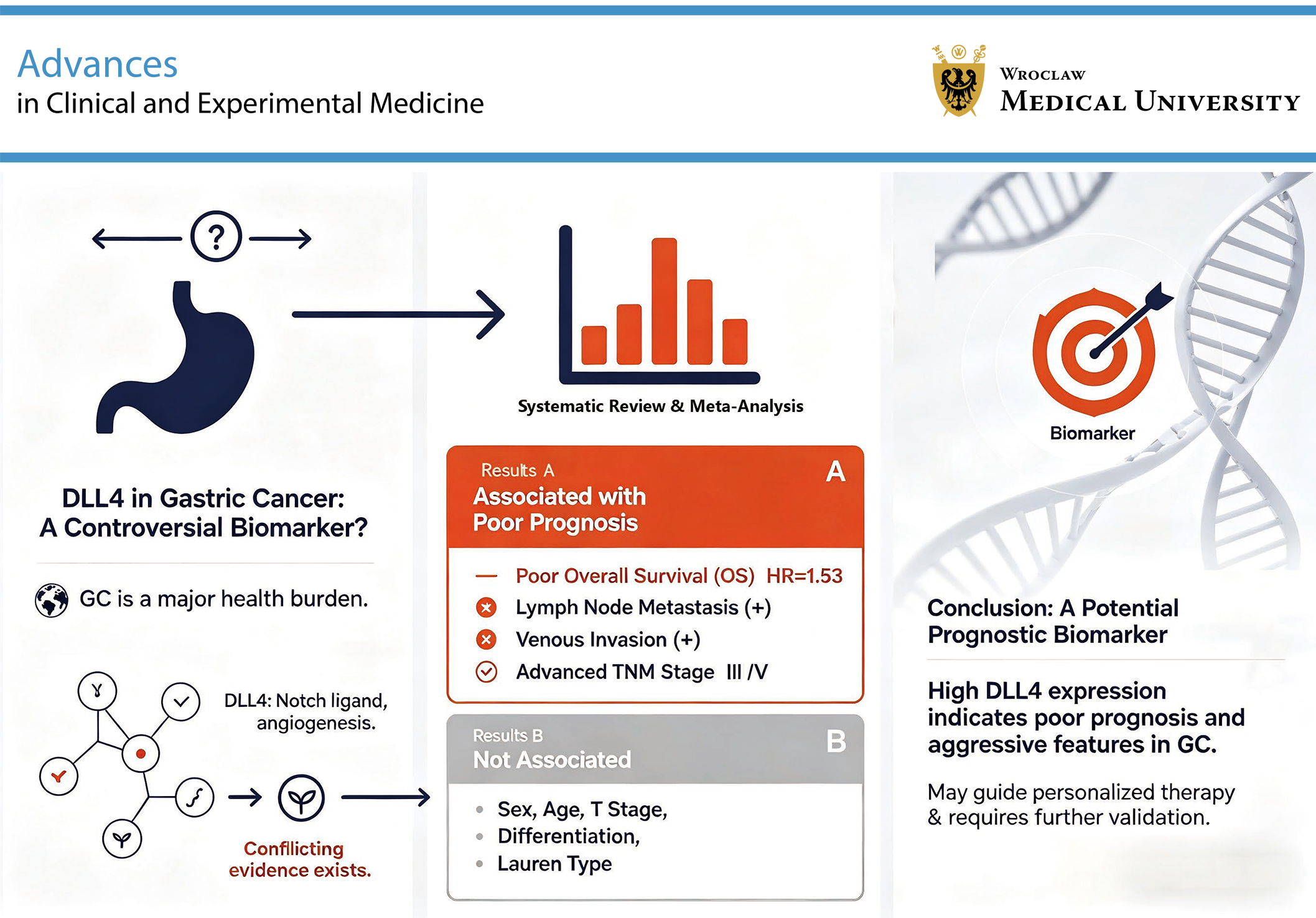
Results. A total of 1,535 patients with GC were included across 7 articles. DLL4 expression was correlated with lymph node metastasis (OR = 5.612, 95% CI: 1.332–23.644; p = 0.019), venous invasion (OR = 3.807, 95% CI: 1.557–9.310, p = 0.003), and TNM stage (OR = 4.183, 95% CI: 1.270–13.775, p = 0.003). However, DLL4 expression was not related to sex (OR = 0.976, 95% CI: 0.767–1.242, p = 0.845), age (OR = 0.765, 95% CI: 0.389–1.506, p = 0.438), T stage (OR = 1.306, 95% CI: 0.717–2.380, p = 0.384), tumor differentiation (OR = 0.952, 95% CI: 0.687–1.318, p = 0.072), or Lauren classification (OR = 1.224, 95% CI: 0.620–2.417, p = 0.560). Furthermore, high DLL4 expression was associated with poorer overall survival (OS) (HR = 1.530, 95% CI: 1.272–1.841, p = 0.000) in patients with GC. The Kaplan–Meier Plotter database confirmed that patients with high DLL4 expression in GC had a poorer prognosis (HR = 1.35, 95% CI: 1.08–1.68, p = 0.009).
Conclusions. DLL4 expression was associated with venous invasion, lymph node metastasis, TNM stage, and poor OS in GC patients, but was not associated with age, sex, T stage, Lauren classification, or tumor differentiation.
Key words: prognosis, meta-analysis, DLL4, gastric cancer, clinicopathological parameters
Introduction
Gastric cancer (GC) was the 5th most commonly diagnosed malignancy worldwide in 2020, with 1,089,103 new cases accounting for 5.6% of all newly diagnosed cancers.1 Gastric cancer also ranked as the 4th leading cause of cancer-related mortality worldwide. Despite substantial advances in modern diagnostic and therapeutic strategies, GC morbidity and mortality remain high, largely because many patients are diagnosed at an advanced stage. Early detection of solid tumors primarily relies on imaging techniques and the identification of serum or tissue biomarkers. Compared with imaging methods, biomarker detection is faster and more convenient and cost-effective.2 Therefore, the identification of reliable biomarkers for early diagnosis and prognostic assessment remains crucial in GC management.
Delta-like ligand 4 (DLL4) is one of the ligands involved in the regulation of the Notch signaling pathway.3 DLL4 plays a critical role in essential biological processes, including angiogenesis and cell proliferation.4 Angiogenesis, a key mechanism underlying tumor growth and progression, contributes to tumor invasion, gastric vascular dysplasia, and the development of metastatic lesions.5, 6 Previous studies have demonstrated that DLL4 expression is associated with prognosis in breast, colon, and nasopharyngeal cancers.7, 8, 9 More recently, increasing evidence has shown that DLL4 is also overexpressed in GC.10, 11, 12, 13, 14, 15, 16 However, the clinicopathological and prognostic significance of DLL4 expression in GC remains controversial. Kim et al. reported no association between high DLL4 expression and lymph node metastasis or vascular invasion in GC.10 In contrast, Ishigami et al. demonstrated significant associations between high DLL4 expression and tumor invasion depth, venous invasion, and lymph node metastasis.11
Objectives
The aim of this meta-analysis was to evaluate the association between DLL4 expression, clinicopathological characteristics, and prognosis in patients with GC, and to clarify the existing controversies regarding its clinical significance.
Materials and methods
Search studies
First, a comprehensive search was conducted in the Web of Science, PubMed, China National Knowledge Infrastructure (CNKI), Cochrane Library, and WanFang databases from inception to September 30, 2024. The following keywords were used: (“gastric carcinoma” OR “gastric cancer” OR “stomach cancer” OR “GC”) AND (“Delta-like 4” OR “DLL4”). In addition, the reference lists of the identified studies were screened to ensure comprehensive inclusion of eligible articles. This study was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Selection criteria
The following inclusion criteria were applied to identify eligible studies: 1) patients diagnosed with GC based on pathological examination; 2) studies evaluating the association between DLL4 expression and clinicopathological parameters (e.g., sex, age, TNM stage, and lymph node metastasis) and/or prognosis in patients with GC; and 3) studies providing sufficient data to calculate 95% confidence intervals (95% CIs).
The exclusion criteria were as follows: 1) studies involving other cancer types; 2) patients who received radiotherapy or chemotherapy before surgery; 3) review articles, conference abstracts, systematic reviews, case reports, letters, and meta-analyses; 4) unavailable full text; and 5) duplicate publications or overlapping patient cohorts. These criteria were applied to minimize potential bias and improve the reliability of the meta-analysis.
Data extraction
Two researchers (Q.D. and C.Z.) independently screened the titles and abstracts of the studies identified through the database search and excluded irrelevant or low-quality articles. The extracted data included the authors, study period, country, publication year, study design, age, sex, tumor differentiation, T stage, lymph node metastasis, venous invasion, Lauren classification, TNM stage, and overall survival (OS). Any discrepancies between the 2 researchers were resolved through discussion. Effect estimates were reported as hazard ratios (HRs) with 95% CIs. Study quality was independently assessed by 2 researchers (Q.D. and C.Z.) using the Newcastle–Ottawa Scale (NOS), which ranges from 0 to 9 points. Studies with NOS scores of 6–9 were considered high-quality.
Statistical analyses
Stata v. 15.0 (StataCorp, College Station, USA) was used for statistical analyses. Review Manager (RevMan) v. 5.4 (The Nordic Cochrane Center, Cochrane Collaboration, Copenhagen, Denmark) was used to assess the quality of the included studies. The Kaplan–Meier Plotter database (http://www.kmplot.com) was used to evaluate the association between DLL4 expression and OS in patients with GC. Odds ratios (ORs), HRs and 95% CIs were extracted or calculated to assess the association between DLL4 expression and clinicopathological characteristics and prognosis in GC patients. Statistical heterogeneity was assessed using Cochran’s Q test and the I2 statistic. I2 values of 25%, 50%, and 75% were considered to indicate low, moderate, and high heterogeneity, respectively. Heterogeneity was prioritized as the primary criterion for model selection, and a half-normal prior distribution was applied for the heterogeneity parameter τ. Specifically, the positive expression rate of DLL4 in GC patients was calculated separately for each of the 7 included studies, and the median value (0.48) was used as the prior estimate. Accordingly, τ was assigned a half-normal (0, 0.48) prior distribution. A random-effects model was applied when the posterior mean of τ was >0, whereas a fixed-effects model was used when τ was approx. 0. Clinical considerations took precedence over statistical heterogeneity when selecting the meta-analytic model. If clinically relevant differences existed among the included studies, a random-effects model was applied regardless of the statistical heterogeneity results. A leave-one-out approach was used for sensitivity analysis.17 Each study was sequentially excluded, and the pooled OR/HR and 95% CI were recalculated after each exclusion. If the pooled effect estimates showed no substantial fluctuation and statistical significance remained consistent following removal of any single study, the meta-analysis results were considered stable and unlikely to be substantially influenced by an individual study. Conversely, marked changes in the pooled estimates suggested potential instability, and the heterogeneity and quality of the included studies required further evaluation.
Results
Literature search and study characteristics and risk of bias assessment
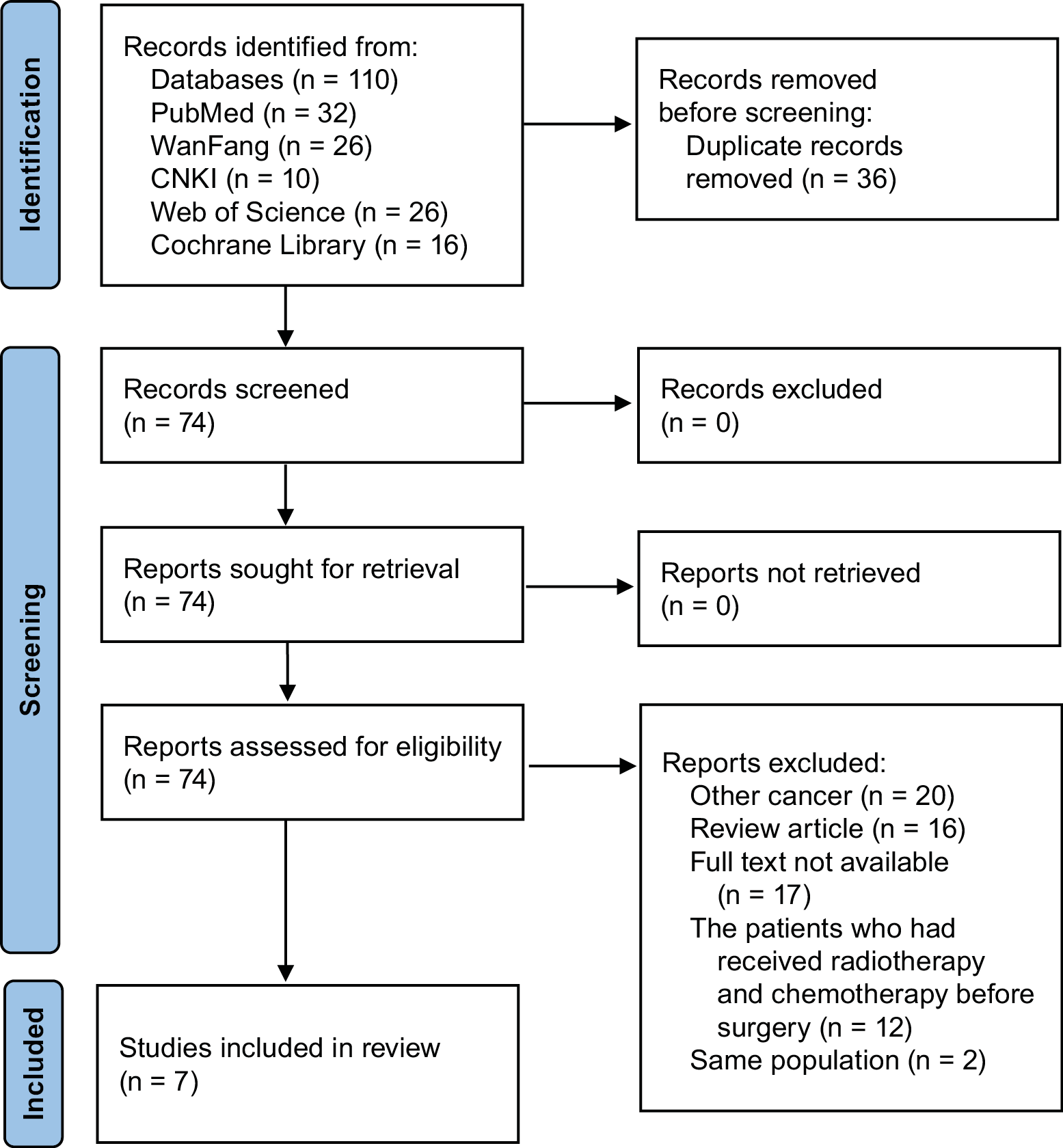
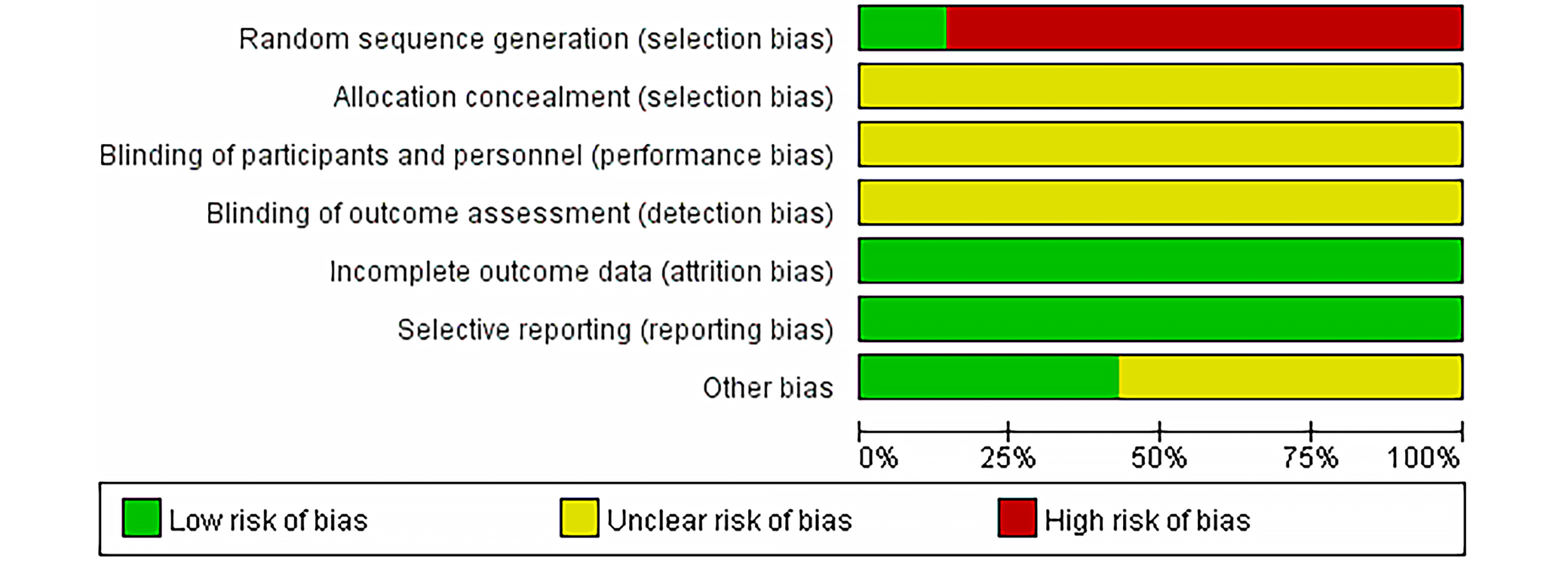
Initially, 110 articles were identified through the database search. After screening the titles and abstracts, 103 articles were excluded, including duplicate studies (n = 36), studies involving other cancer types (n = 20), review articles (n = 16), unavailable full texts (n = 17), studies including patients who had received radiotherapy or chemotherapy before surgery (n = 12), and studies with overlapping populations (n = 2). Ultimately, 7 studies were included in the meta-analysis. The study selection process is presented in Figure 1, and the risk-of-bias assessment generated using RevMan is shown in Figure 2. In total, the meta-analysis included 1,535 patients with GC. The main characteristics and quality assessments of the included studies are summarized in Table 1.10, 11, 12, 13, 14, 15, 16
DLL4 expression and clinicopathological factors
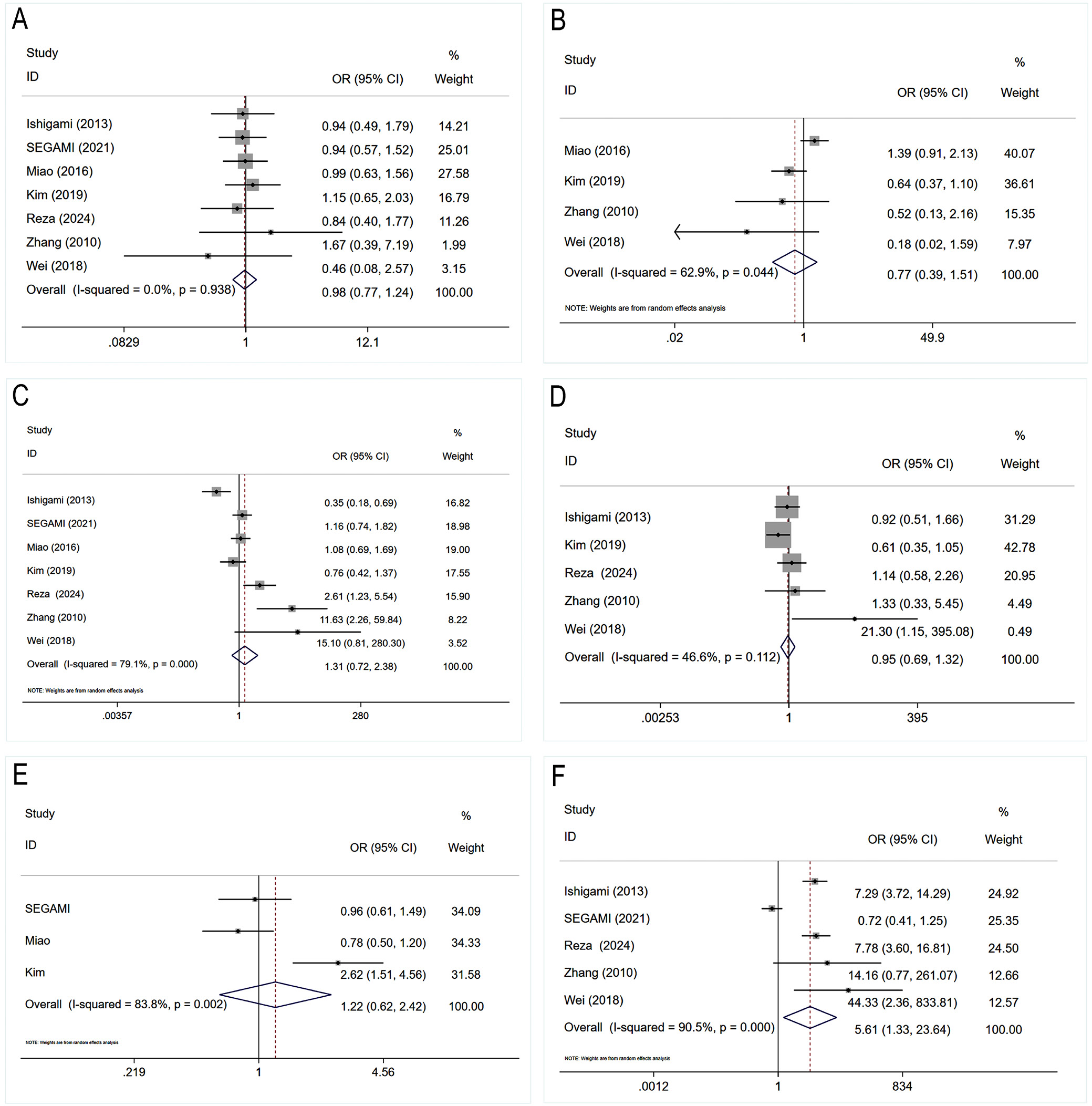
The associations between DLL4 expression and the clinicopathological characteristics of GC are presented in Table 210, 11, 12, 13, 14, 15, 16 and Figure 3. The pooled analysis showed that DLL4 expression was not significantly associated with sex (OR = 0.976, 95% CI: 0.767–1.242, p = 0.845) (Figure 3A), age (OR = 0.765, 95% CI: 0.389–1.506, p = 0.438) (Figure 3B), T stage (OR = 1.306, 95% CI: 0.717–2.380, p = 0.384) (Figure 3C), tumor differentiation (OR = 0.952, 95% CI: 0.687–1.318, p = 0.772) (Figure 3D), or Lauren classification (OR = 1.224, 95% CI: 0.620–2.417, p = 0.560) (Figure 3E). In contrast, high DLL4 expression was significantly associated with lymph node metastasis (OR = 5.612, 95% CI: 1.332–23.644, p = 0.019) (Figure 3F), venous invasion (OR = 3.807, 95% CI: 1.557–9.310, p = 0.003) (Supplementary Fig. 1A), and advanced TNM stage (OR = 4.183, 95% CI: 1.270–13.775, p = 0.003) (Supplementary Fig. 1B).
Publication bias
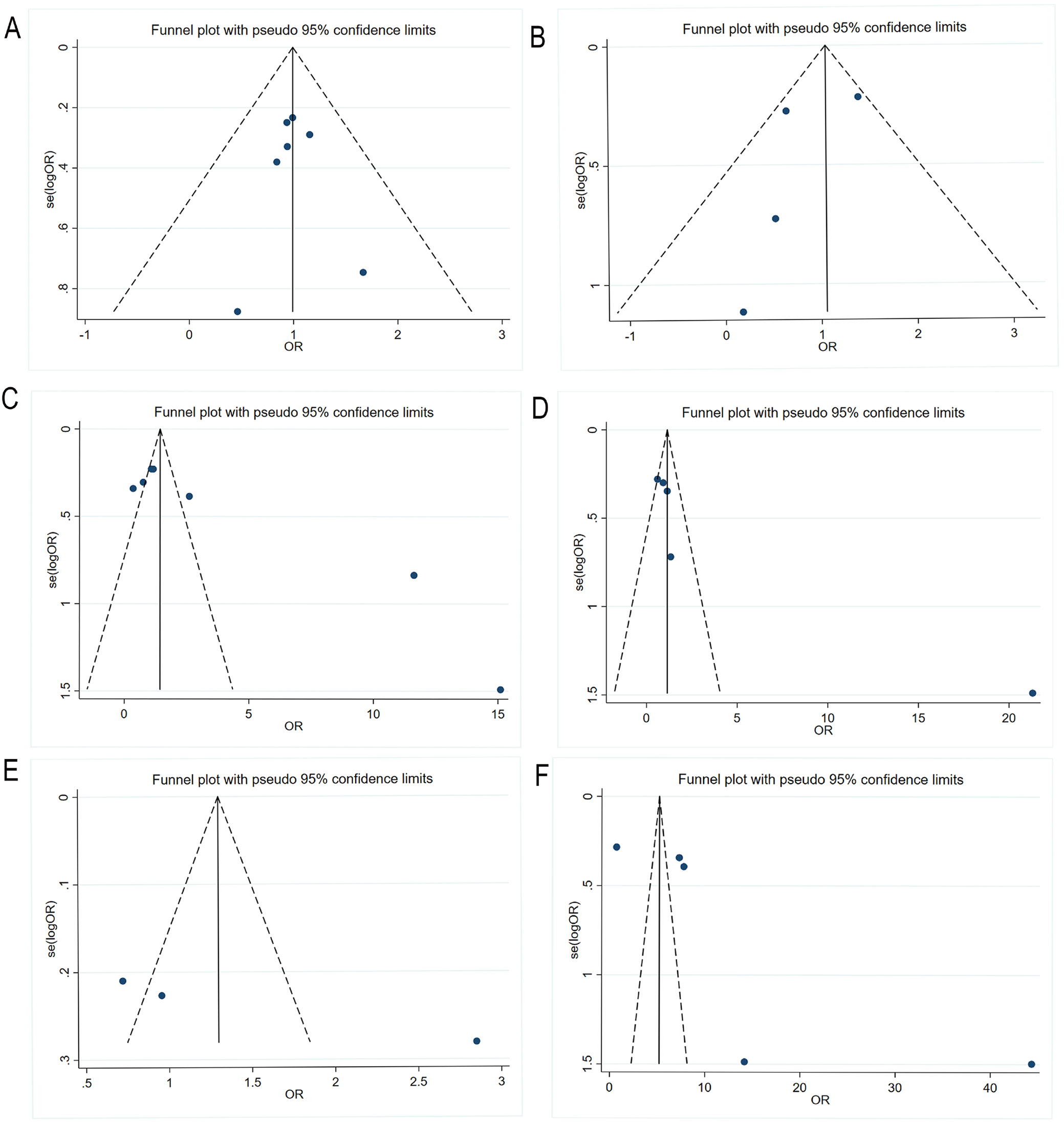
Publication bias was assessed visually using funnel plots. The funnel plots illustrate the distribution of standard error (SE) against the OR for the analyzed clinicopathological parameters. In Figure 4A, B, C, and E, the data points were distributed relatively symmetrically around the central vertical line, suggesting no major asymmetry in the effect estimates. In contrast, Figure 4D and F and Supplementary Fig. 1C and D showed a sparser distribution of data points, with several studies located near the outer boundaries of the pseudo 95% confidence limits, indicating variability in estimate precision. Nevertheless, the overall funnel plot patterns remained approximately symmetrical. No evident publication bias was observed for the associations between DLL4 expression and sex (Figure 4A), age (Figure 4B), T stage (Figure 4C), tumor differentiation (Figure 4D), Lauren classification (Figure 4E), lymph node metastasis (Figure 4F), venous invasion (Supplementary Fig. 1C), or TNM stage (Supplementary Fig. 1D).
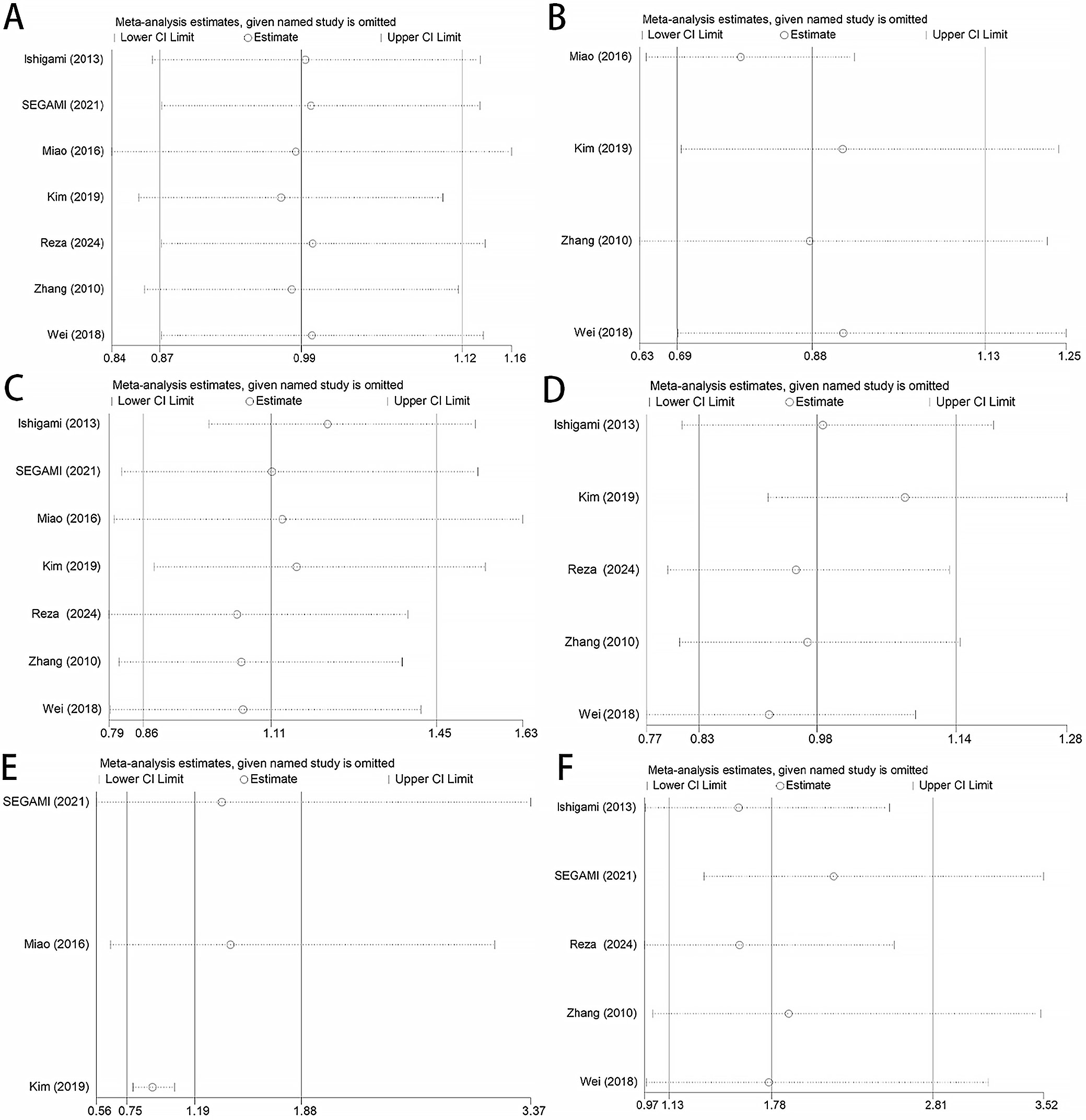
Sensitivity analysis
Sensitivity analysis was performed to evaluate the stability and reliability of the associations between DLL4 expression and clinicopathological characteristics in patients with GC. The results demonstrated that the pooled estimates for sex (Figure 5A), age (Figure 5B), T stage (Figure 5C), tumor differentiation (Figure 5D), Lauren classification (Figure 5E), lymph node metastasis (Figure 5F), venous invasion (Supplementary Fig. 1E), and TNM stage (Supplementary Fig. 1F) remained stable after sequential exclusion of individual studies, indicating good robustness of the meta-analysis results.
Descriptive statistical analysis
Descriptive statistical analyses were performed for 3 clinicopathological parameters (venous invasion, Lauren classification, and TNM stage), as these analyses were based on only 3 included studies and the corresponding results from the forest plots, funnel plots, and sensitivity analyses may therefore be unreliable. The findings of the descriptive analyses for these 3 clinicopathological parameters are summarized in Table 3.
DLL4 expression and OS of GC patients
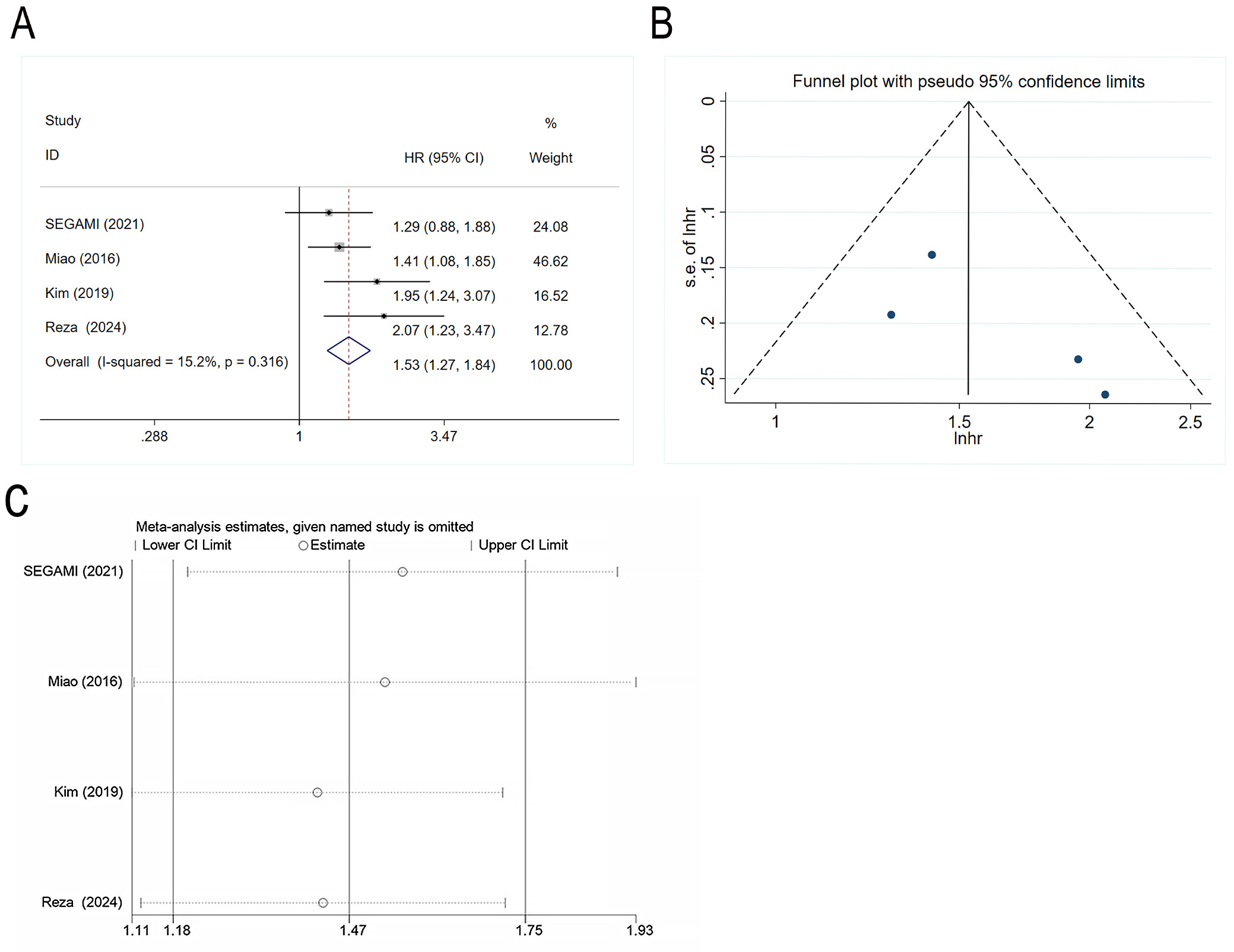
A total of 1,267 patients with GC from 4 studies were included in the analysis evaluating the association between DLL4 expression and OS. The pooled analysis demonstrated that high DLL4 expression was significantly associated with poor prognosis in GC patients (HR = 1.530, 95% CI: 1.272–1.841, p < 0.001) (Figure 6A). The funnel plot shown in Figure 6B demonstrated a relatively symmetrical distribution of data points around the central vertical line, suggesting no major asymmetry in the effect estimates. No evident publication bias was observed for the association between DLL4 expression and OS. Sensitivity analysis showed that sequential exclusion of individual studies did not substantially alter the pooled results, indicating good robustness of the findings (Figure 6C).
Database validation and differential expression analysis
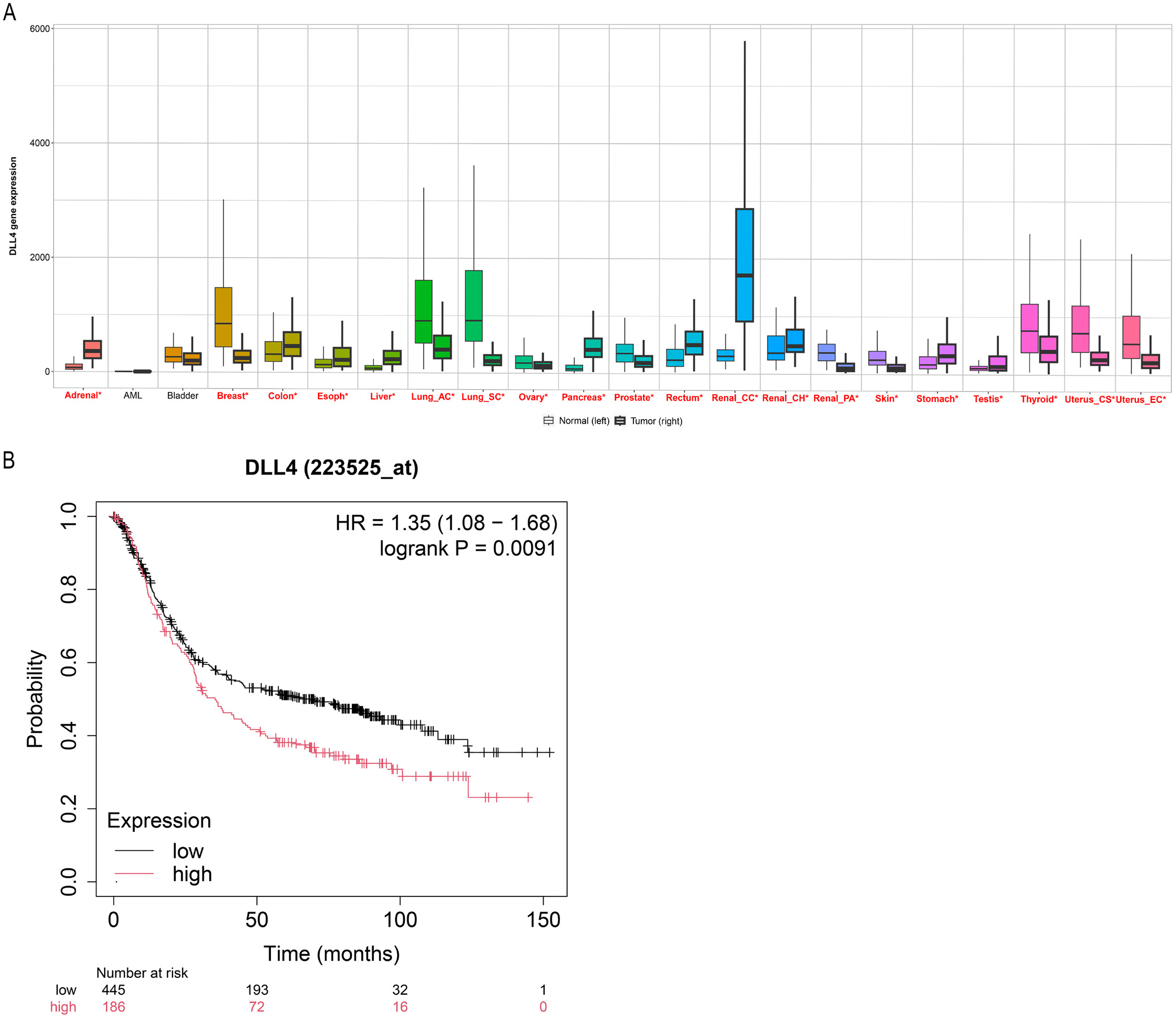
Analysis using the Kaplan–Meier Plotter database (https://www.kmplot.com/analysis/) demonstrated that DLL4 expression was significantly higher in GC tissue than in normal gastric tissue (Figure 7A). Survival curve analysis further showed that high DLL4 expression was significantly associated with poorer OS in patients with GC (HR = 1.35, 95% CI: 1.08–1.68, p = 0.009) (Figure 7B).
Discussion
Cancer is a major cause of mortality in both developed and developing countries. Gastric cancer is one of the most common malignancies of the digestive tract and a leading cause of cancer-related death worldwide. It ranks as the 5th most frequently diagnosed cancer globally in terms of newly diagnosed cases.17 Several studies have demonstrated that early diagnosis and treatment can significantly improve the prognosis of GC patients.18, 19 Therefore, the identification of effective biomarkers for early diagnosis and prognostic assessment remains essential in GC. Our previous research demonstrated that UCP2 is associated with the clinicopathological characteristics and prognosis of GC patients and may serve as a useful prognostic biomarker.20 Recent studies have also suggested that DLL4 is associated with the clinicopathological features and prognosis of GC; however, the reported findings remain controversial. In the present meta-analysis, high DLL4 expression was significantly associated with advanced TNM stage, lymph node metastasis, venous invasion, and poor OS, but not with sex, age, T stage, tumor differentiation, or Lauren classification in GC patients. These findings suggest that high DLL4 expression may serve as a prognostic biomarker in GC.
Angiogenesis is a fundamental process in tumor growth and progression that contributes to aggressive and metastatic tumor behavior.17 Accumulating evidence indicates that the Notch signaling pathway plays a critical role in cell proliferation, differentiation, vascular development, and angiogenesis.21 Notably, DLL4 is a key regulator of tumor angiogenesis and neovascularization.22, 23, 24 Overexpression of DLL4 has been associated with clinicopathological characteristics and prognosis in multiple cancer types. Wang et al. reported that increased DLL4 protein expression in breast cancer was associated with shorter OS.25 Kim et al. demonstrated that patients with positive DLL4 expression had significantly poorer OS than those with negative DLL4 expression in colorectal cancer.26 Kuramoto et al. confirmed that DLL4 plays a crucial role in liver metastasis of small cell lung cancer.27 Drouillard et al. reported that high DLL4 expression predicted poorer OS and shorter disease-free survival (DFS) following resection of pancreatic adenocarcinoma.28 Furthermore, several studies have investigated the role of DLL4 expression in GC tissues.10, 12, 13, 14 Previous studies demonstrated that DLL4 expression is significantly elevated in GC cells and tissues.29 In addition, associations between DLL4 expression and clinicopathological characteristics of GC patients have been reported. Several studies showed that high DLL4 expression was associated with venous invasion in GC. However, the relationship between DLL4 expression and clinicopathological characteristics in GC remains controversial. Kim et al. found no significant association between DLL4 expression and venous invasion in 336 GC patients.10 Moreover, some studies suggested that DLL4 expression is associated with TNM stage in GC.10, 15, 16 In contrast, Ishigami et al. reported no significant association between DLL4 expression and TNM stage in GC tissues.11 According to our meta-analysis, high DLL4 expression was significantly associated with advanced TNM stage, lymph node metastasis, and venous invasion.
Several studies have assessed the effect of anti-DLL4 therapy on the frequency of cancer stem cells. These findings showed that anti-DLL4 treatment led to a twofold reduction in cancer stem cell frequency.30 Additionally, some authors reported a significant correlation between T stage and high DLL4 expression in patients,14, 15, 16 whereas others found no such association in patients with GC.10, 11, 12, 13 Similarly, several studies reported no correlation between DLL4 expression and Lauren classification,10, 11, 13 and others found no association between DLL4 expression and tumor differentiation.10, 11, 14, 15, 16
In our study, DLL4 expression was not associated with tumor differentiation, T stage, or Lauren classification. However, the clinical significance of DLL4 expression and its relationship with T stage, tumor differentiation, and Lauren classification in GC patients should be further investigated in randomized controlled trials (RCTs) with larger sample sizes. Further studies are also needed to elucidate the key regulatory mechanisms of the DLL4 signaling pathway in GC cells.
DLL4 plays a significant role in several cancer types and acts as an oncogene-like factor.25, 26, 27, 28 Numerous studies have demonstrated that DLL4 expression is associated with poor survival across a variety of tumor types.25, 26, 28, 31 Furthermore, several authors have evaluated the potential prognostic significance of DLL4 expression in patients with GC. However, the relationship between DLL4 expression and OS in GC patients remains controversial. According to Segami et al., there was no significant difference in the 5-year survival rate between GC patients with DLL4-positive and DLL4-negative expression.12 In contrast, other studies reported lower survival rates in GC patients with high DLL4 expression compared with those with low DLL4 expression.10, 11, 13, 14
Our meta-analysis demonstrated that GC patients with high DLL4 expression had poorer OS. The Cancer Genome Atlas (TCGA) database and a comprehensive survival analysis using the Kaplan–Meier Plotter were further used to validate these findings.
Limitations of the study
Several limitations of this meta-analysis should be acknowledged. First, although extensive searches were conducted across multiple databases, the relatively small number of included studies may have introduced bias into the findings. Second, the included studies applied different criteria for certain clinicopathological parameters, including patient selection and research methodologies, and the heterogeneity resulting from these differences could not be ignored. Finally, the relatively limited sample size prevented detailed analyses of individual cases.
Conclusions
This meta-analysis revealed that DLL4 expression was associated with venous invasion, lymph node metastasis, TNM stage, and poor OS, but was not associated with age, T stage, sex, tumor differentiation, or Lauren classification. These findings suggest that DLL4 may serve as a predictor of poor prognosis in GC patients. Further large-scale studies with more homogeneous patient populations are needed to better clarify the relationship between DLL4 expression and the clinicopathological characteristics and prognosis of GC patients.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.19742186. The package contains the following files:
Supplementary Fig. 1. Forest plots for the relationship of DLL4 expression with venous invasion (A) and TNM stage (B). Funnel plots for the relationship between DLL4 expression with venous invasion (C) and TNM stage (D). Sensitivity analysis for the relationship between DLL4 expression with venous invasion (E) and TNM stage (F).
Use of AI and AI-assisted technologies
Not applicable.