Abstract
Ageism, defined as stereotypes, prejudice, and discrimination toward older adults, represents a global challenge with negative consequences for health, wellbeing, and quality of care. This review aimed to analyze the characteristics and effectiveness of educational interventions designed to reduce ageism in healthcare settings. A systematic review was conducted using PubMed, Embase, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Scopus. Eleven primary studies met the inclusion criteria: 1) educational or training interventions targeting healthcare professionals or students; 2) primary studies; 3) quantitative or mixed-methods designs with extractable quantitative outcomes; 4) published between 2020 and 2025; and 5) articles in English or Spanish. Three main types of interventions were identified. First, gerontological education has shown promising effects, particularly when explicitly addressing ageism, although the evidence remains limited. Second, clinical simulation-based interventions yielded mixed results, especially when not supported by structured educational components. Third, empathy-focused interventions were insufficient to reduce ageist attitudes. Only 1 randomized trial was conducted among healthcare professionals. Educational multicomponent interventions, particularly those incorporating gerontological content, may help reduce ageism in healthcare settings. However, the available evidence is limited and heterogeneous, and remains largely restricted to student populations. Further methodologically robust studies, particularly among practicing healthcare professionals and in real clinical settings, are needed to determine whether improvements in attitudes translate into sustained changes in clinical practice.
Keywords: ageism, health personnel, medical education, aged, quality of healthcare
Introduction
Ageism in society
Since antiquity, age has been a central axis of social organization, shaped by demographic transformations that continuously redefine generational boundaries and their sociocultural implications.1, 2 In many societies, these transformations have contributed to the emergence and consolidation of negative perceptions of aging, normalizing stereotypes and discriminatory attitudes collectively referred to as ageism.3, 4
According to a World Health Organization (WHO) report,5 ageism encompasses stereotypes (how we think), prejudice (how we feel), and discrimination (how we act) directed at individuals based on their age. This phenomenon may operate at institutional, interpersonal, or self-directed levels.
Institutional ageism refers to policies, norms, and practices that perpetuate age-based inequalities within organizations and social systems, restricting equitable access to opportunities and resources (e.g., a company that prioritizes recruiting individuals under 40). Interpersonal ageism manifests in everyday interactions when one person holds or expresses stereotypes or prejudices toward another person (e.g., a physician addressing an older patient as though they were unable to understand basic information).
Self-directed ageism occurs when individuals internalize age-related stereotypes and apply them to themselves (e.g., an older adult avoiding a course because they believe it is “too late to learn”), which can adversely affect wellbeing, health, and behavior. Collectively, these forms of ageism generate substantial societal costs, amounting to billions of euros annually.5
Institutional ageism in healthcare
Healthcare systems are not immune to ageism. In healthcare settings, ageism reduces equity in access to diagnosis, treatment, and rehabilitation, leading to fragmented care pathways that may contribute to disease chronicity and increased readmission rates.5, 6 In Spain, chronic conditions disproportionately affect older adults: more than half of individuals aged 85 years or older have at least 1 chronic disease, and 10.9% of those aged over 65 report severe limitations in basic activities of daily living, according to data from the Spanish National Research Council (CSIC) and the National Institute of Statistics (INE).7
These conditions, combined with erroneous assumptions about older adults’ physical and cognitive capacities, lead to less proactive care and reduced clinical follow-up.8 Prior studies indicate that unequal treatment can produce significant biopsychosocial consequences, including a higher risk of depression, increased risky behaviors, deterioration in quality of life, and greater loneliness and social isolation.9 Overall, ageist attitudes degrade the quality of care and directly affect older adults’ health and wellbeing.10
Ageism among healthcare professionals has been assessed using a range of instruments that capture cognitive (stereotypes), affective (prejudices), and behavioral (discrimination) dimensions. Commonly used measures include the Fraboni Scale of Ageism (FSA),11 which assesses negative attitudes toward older adults across 3 subdimensions (isolation, stereotypes, and avoidance); Kogan’s Attitudes Toward Old People Scale (KAOP),12 which evaluates both positive and negative perceptions of older adults; the Questionnaire of Negative Stereotypes Toward Older People (CENVE),13 which focuses on negative stereotypes about aging; and the WHO Ageism Scale,14 designed to measure ageism at the individual, interpersonal, and structural levels. These instruments help to identify how stereotypes and prejudices may translate into discriminatory practices.15, 16
However, recent reviews have reported substantial variability in ageism levels across studies, alongside considerable methodological heterogeneity. This variability complicates direct comparisons and highlights the need for more robust, context-specific research.17, 18
Interventions to reduce ageism
Interventions to reduce ageism have attracted growing scientific interest. A pioneering systematic review in the general population by Burnes et al. found that the most effective strategies combine education and intergenerational contact, producing significant attitude changes.19 More recent reviews confirm that multicomponent programs, particularly those integrating direct experiences with older adults, have a more sustained impact on prejudice reduction.20 In higher education, a recent systematic review and meta-analysis by Martínez-Arnau et al., including studies published up to 2020, identified 3 effective intervention types for reducing ageism among undergraduate healthcare students: empathy-based, aging knowledge-based, and clinical skills-based approaches.21 However, the effectiveness of similar interventions among healthcare professionals remains unclear, as clinical practice is influenced by organizational factors, workload pressures, and care models that may limit how well learning transfers to practice.22, 23
Furthermore, in recent years, there has been a growing interest in ageism, particularly following the COVID-19 pandemic. The wider adoption of active learning methodologies such as clinical simulation and experiential learning,3, 4, 15 and increased institutional emphasis on empathy, person-centered communication, and care for vulnerable populations5, 17, 24 underscore the need to update the available evidence on these interventions, both in students and qualified healthcare professionals, as well as to adapt and evaluate anti-ageism programs in real professional contexts to ensure durable improvements in the quality of care for older adults.
Unlike previous reviews that examined ageism in the general population or evaluated interventions without distinguishing between educational and clinical contexts, the present review focuses specifically on the healthcare setting, integrating both students and practicing professionals. This approach enables an exploration of the transferability of learning to clinical practice. It includes a critical methodological analysis of experimental designs, with particular attention to causal inference, examining elements such as the presence and type of control group and group × time interaction effects. Consequently, this review aims not only to identify which interventions appear effective but also to examine which educational components are associated with more consistent outcomes, thereby informing the design of future training programs and more methodologically robust research in healthcare contexts.
Objectives
The objective of this study was to update and critically analyze the effectiveness and characteristics of educational and training interventions aimed at reducing ageism in healthcare through a systematic review.
Materials and methods
A systematic review of interventions to reduce ageism among healthcare students and professionals was conducted. The review was registered in PROSPERO on April 22, 2025 (ID: 1037975) and followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.25
Using a PICO approach, we sought to identify and analyze the implementation of programs (Intervention) directed at healthcare professionals and students (Population), compared with usual training or no intervention (Comparison), to evaluate the impact on the reduction of discrimination, stereotypes, and inequality toward older adults (Outcome).
Eligibility criteria
To identify current effective interventions to combat ageism in healthcare settings, we conducted a systematic review of the scientific literature. The following inclusion criteria were applied: 1) studies reporting educational or training interventions targeting healthcare professionals or healthcare students; 2) primary research studies; 3) quantitative or mixed-methods designs reporting extractable quantitative outcomes; 4) publications between 2020 and 2025; and 5) articles published in English or Spanish. The search was limited to articles published between 2020 and 2025, given prior evidence from reviews by Burnes et al. and Martínez-Arnau et al. in the general population and among healthcare students, respectively.19, 21
The exclusion criteria were: 1) studies not reporting intervention-related outcomes; and 2) studies involving participants under 18 years of age.
Search strategy
A bibliographic search was performed in PubMed, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), and Scopus. Search terms were developed to reflect population, context, and objectives. The initial search was conducted on March 12, 2025, and the last search on November 10, 2025. Search strategies were developed across databases around 3 conceptual blocks to ensure equivalence: 1) terms related to ageism and age-related constructs (e.g., ageism, ageist, elder, aging, older, senior); 2) terms identifying the target population of healthcare students and professionals (e.g., healthcare personnel, health student, college); and 3) terms capturing educational or training interventions (e.g., intervention, education, clinical trial, program). The detailed search strategy is presented in Table 1.
Study selection
The retrieved records were imported into RefWorks (ProQuest LLC, Ann Arbor, USA), and duplicate entries were removed. Two reviewers (A.C.B. and E.C.S.) independently screened titles and abstracts against predefined inclusion and exclusion criteria. The full texts of potentially eligible articles were then independently assessed by 2 authors (A.C.B. and E.C.S.); any disagreements were resolved through discussion or, when necessary, consultation with a 3rd reviewer (L.F.P.).
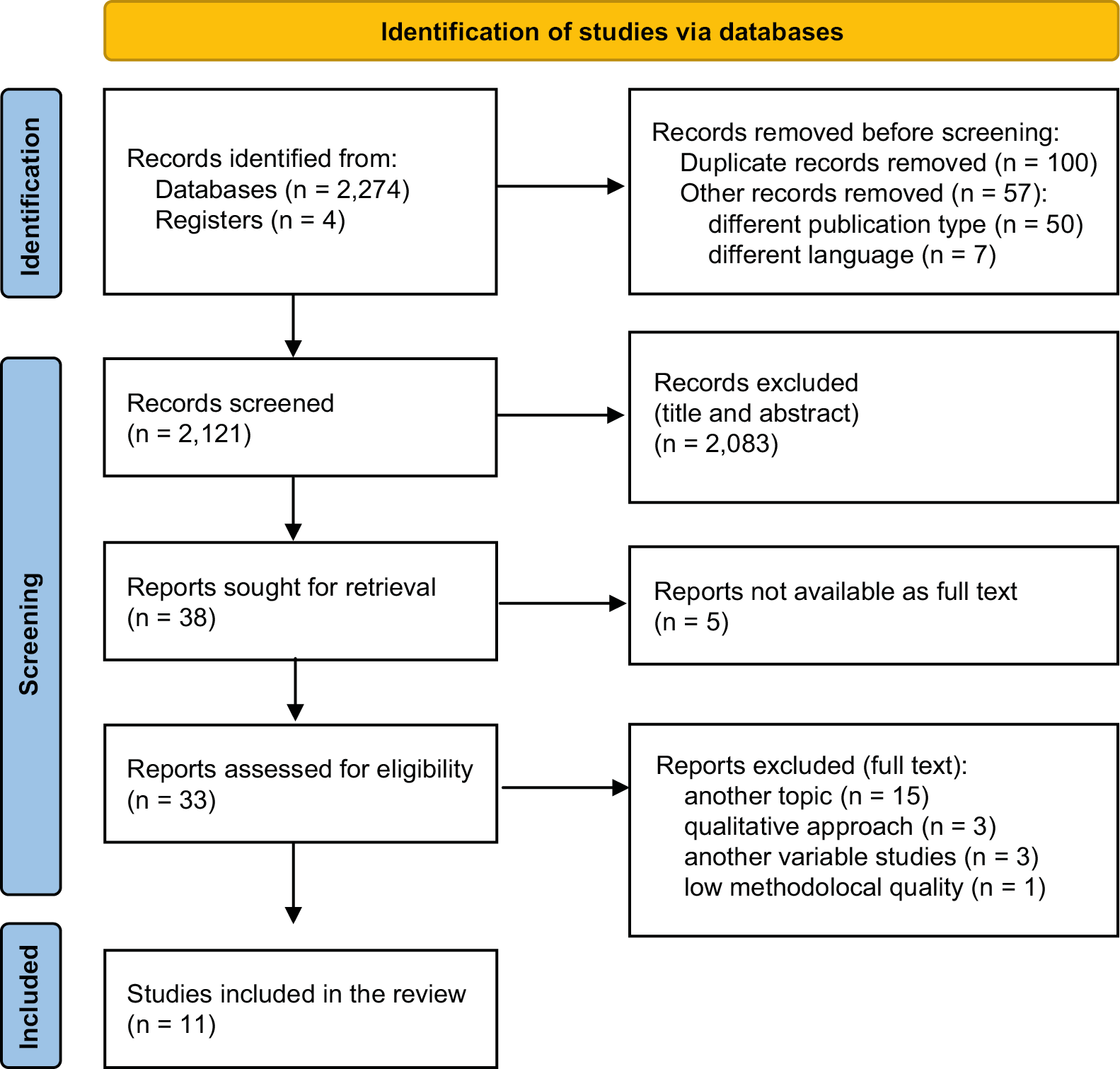
To minimize subjectivity in exclusion decisions, a sequential prioritization approach was used. In total, 2,278 records were identified. Initially, 7 studies were excluded for not being published in English or for being deemed unrelated to the study’s aim. After title and abstract screening, 2,083 records were excluded, and full-text retrieval was not possible for 5 reports.
Finally, 15 records were excluded for addressing a different topic; 3 for using a qualitative approach exclusively; 3 for measuring outcomes other than ageism (e.g., caring competence or empathy); and 1 study was excluded due to low methodological quality, specifically due to the use of non-validated ad hoc questionnaires and the absence of a control group and follow-up assessment. Finally, 11 studies met the eligibility criteria following full-text review. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
Data extraction
Data were extracted using a predefined matrix developed by consensus among reviewers. Two reviewers (A.C.B. and L.F.P.) independently extracted data, and a 3rd reviewer (A.M.S.) resolved discrepancies. Extracted items included: authors, year of publication, geographic region, study design, population, intervention type, professional characteristics, ageism scale used, other instruments, analyses performed, publication quality, and outcomes. Key confounders recorded were age, sex, marital status, years of education, professional category, years of work experience, cohabitation with older adults, and willingness to work with older people.
A meta-analysis was not feasible due to substantial heterogeneity across studies in terms of intervention type, outcome domains, measurement instruments, and study design. In addition, assessment time points varied considerably, and several studies did not report effect sizes or provide sufficient data for quantitative synthesis. Conducting a meta-analysis under these conditions could yield misleading estimates; therefore, a narrative synthesis was considered the most appropriate approach.
Studies were categorized by participant type (students vs healthcare professionals) and intervention modality. Within these categories, common design and implementation features were systematically examined to explore how different approaches influenced ageist attitudes, perceptions, and behaviors.
Quality appraisal
Two authors independently assessed study quality using the Joanna Briggs Institute (JBI) Critical Appraisal Tools.26, 27 The JBI checklists for non-randomized studies (9 items) and randomized controlled trials (RCTs; 13 items) were used. Each criterion was rated as present, absent, unclear, or not applicable. The JBI tool evaluates the representativeness of the sample, study design, and the use of statistical tests. Results are summarized in Table 2.28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38
Results
Eleven studies were included in the presented review. Characteristics are summarized in Table 3.28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38 Four studies used quasi-experimental designs,29, 31, 33, 38 while the remainder were RCTs.28, 30, 32, 34, 35, 36, 37 Most studies were conducted with health sciences students (nursing, medicine, pharmacy, psychology, physiotherapy), aged 18–25. Only 1 study34 included healthcare professionals (registered nurses aged 30–65). Geographically, 5 studies originated in Turkey,29,32,35–37 2 in Spain,30, 31 and the remainder in various Asian countries.28, 33, 34
Overall methodological quality ranged from moderate to high across the 11 included studies (Table 2). Nevertheless, potential biases and limitations were identified across most of the included studies, as discussed below.28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38 Interventions were heterogeneous, but they were grouped into 3 main types: 1) simulation programs using aging suits or practical scenarios28, 29, 31, 37, 38; 2) structured educational programs30, 33, 34, 35; and 3) empathy-focused interventions.32, 36 Some studies combined 2 types (e.g., simulation plus education28, 29 or intergenerational contact plus education30, 33, 35). Regarding the control group (CG), 4 articles received no intervention32, 33, 34, 38; 2 did not include a CG31, 38; and the remaining studies received reduced or alternative versions of the main intervention,28, 29, 30, 35, 36 which may have introduced performance bias in outcome assessment. Baseline analyses generally showed no significant sociodemographic differences between groups, except in Kim and Nam,33 where the CG showed higher baseline ageism and anxiety about aging than the intervention group (IG). Moreover, Pekçetin et al. did not adequately describe baseline group differences.35 All included studies used validated instruments. The Kogan’s Attitudes Toward Old People Scale (KAOP) was the most frequently used questionnaire to assess ageist attitudes. In the sole study with healthcare professionals,34 the Ageism in Nursing Care of Older People Scale was used to assess ageism.
Educational interventions and intergenerational contact
Four studies implemented interventions, either alone or in combination with intergenerational contact, focused on gerontological and geriatric education and on raising awareness of ageism and its societal implications.
On the one hand, studies that combined structured gerontological education with intergenerational contact include Fernández-Gutiérrez et al.,30 Kim and Nam,33 and Pekçetin et al.35 They share a multi-session design (6–8 sessions) of 90–120 min each, in which healthcare students receive targeted instruction on aging and ageism and participate in direct interaction activities with older adults. Fernández-Gutiérrez et al.30 and Pekçetin et al.35 found improvements in attitudes on IG. However, only the study by Pekçetin et al.35 reported non-significant group x time interaction effects, likely due to the small sample size, which reduced statistical power to detect differences. Regarding the study by Kim and Nam,33 which reported a lack of effectiveness, baseline differences were observed between groups (IG and CG) in some measures, including FSA. Therefore, interventions combining an educational component with intergenerational contact may be effective; however, more methodologically robust studies are needed to confirm these findings.
Only 1 study implemented a specific geriatric training program explicitly aimed at reducing ageism among its participants. This study was notably more extensive, comprising 6 sessions, and more methodologically robust, with results favoring the intervention.34 It is also worth noting that this was the only study conducted among healthcare professionals.
Interventions based on clinical simulation
Five studies used simulation-based interventions, using aging suits or clinical cases, either fully or partially, to reduce ageist beliefs and attitudes among healthcare students. However, despite sharing a common pedagogical rationale, these interventions varied substantially, limiting the strength and consistency of their findings.
Among these, 2 studies share a common pedagogical rationale: combining an immersive experiential component with a brief educational program.28, 29 Both studies reported improvements in ageist attitudes, as measured using the KAOP scale; however, neither included an analysis of the group × time interaction, thereby limiting causal interpretation. Additionally, in the study by Cheng et al.,28 post-test measures were administered on the same day as the intervention, precluding assessment of longer-term effectiveness.
On the other hand, the 3 remaining studies emphasize structured analysis of clinical scenarios involving older adults, aiming to foster critical reflection and improve understanding of this population’s needs without using an educational program.31, 37, 38 Each intervention consisted of a single brief session lasting 60–90 min, followed by a debriefing. Both Gil-Pons et al.31 and Söylemez et al.37 reported improvements in the IG for the presence of ageism, whereas White et al.38 did not find differences over time. Additionally, the only study that used group × time interaction effects failed to demonstrate substantial changes across groups and time.37 The absence of a more structured and sustained intervention design may have contributed to the limited results observed in this group of interventions.
Empathy-focused programs
This section includes studies that primarily targeted empathy, notably those conducted by Gür and Yilmaz32 and Sari et al.36 Both sought to develop interventions focused on empathy through mindfulness programs32 or an aging awareness program.36
Although the 2 studies differed significantly in their intervention details, they showed similar results: empathy scores increased significantly in both cases, whereas ageist attitudes remained unchanged. Specifically, Gür and Yilmaz32 reported minimal changes in attitudes toward older adults, while Sari et al.36 found no significant change. These findings suggest that interventions focused solely on empathy are insufficient to reduce ageist attitudes.
Discussion
The primary aim of this review was to update and critically appraise the effectiveness of existing interventions designed to reduce ageist behaviors among healthcare professionals and students and to examine potential barriers and facilitators. Specifically, 3 main types of interventions were identified: clinical simulation-based interventions, educational programs alone or combined with intergenerational contact, and empathy-focused programs.
A key strength of this review lies in its focus on moving beyond a purely descriptive synthesis of outcomes to address the methodological issue of causal attribution. However, the available evidence is heterogeneous and should be interpreted cautiously. Rather than assuming that post-intervention improvements necessarily indicate effectiveness, this review evaluated whether the included studies met minimum criteria for causal inference, including a control-group design, baseline group comparability, and adequate statistical analyses. This analytical approach highlights that a substantial proportion of the existing literature presents methodological limitations that may hinder the confident attribution of observed changes in ageist attitudes to the interventions themselves.
Regarding educational interventions, to our knowledge, only 1 study conducted among healthcare professionals34 demonstrated that an educational intervention specifically aimed at reducing ageism was effective in reducing prejudice and negative attitudes toward older patients in healthcare settings. These results are consistent with the findings of Martínez-Arnau et al., who reported the effectiveness of this type of intervention among undergraduate healthcare students.21 This study extends this evidence to practicing professionals for the first time. However, although its results are encouraging, further research is needed to confirm these findings.
Additionally, when intergenerational contact was added to the education program, results also appeared effective. Nevertheless, further studies are needed to confirm these findings, given the methodological limitations identified, including selection bias33 and the absence of group × time interaction analyses.30 These findings are consistent with previous reviews indicating that multicomponent interventions (education combined with intergenerational contact) tend to produce greater effects than didactic-only approaches in both the general population19 and among health and social sciences students.21 This approach is grounded in the PEACE theoretical framework (Positive Education about Aging and Contact Experiences), which posits that accurate education about aging, when combined with positive contact experiences and guided reflection,10 facilitates stereotype replacement and reduces anxiety about aging.39, 40 However, although educational interventions may help reduce ageism, the impact of programs combining education with intergenerational contact among practicing healthcare professionals remains largely unknown. Future research should build on evidence derived from student populations to evaluate the effectiveness of such interventions in clinical settings. In this regard, routine interactions between healthcare professionals and older patients may provide a valuable opportunity to design practice-based interventions that integrate education with real intergenerational contact.10
Similarly, clinical simulation appears to be associated with reductions in ageism among healthcare students, particularly when combined with educational components. This finding is consistent with the systematic review by Martínez-Arnau et al.,21 which also highlights the role of virtual patient simulation as an effective tool for enhancing empathy and communication skills among healthcare students.41 Indeed, simulation-based learning is currently considered a core educational strategy in healthcare training.42 However, the potential impact of combining patient-based simulation with structured educational components among healthcare professionals remains largely unexplored. The use of older standardized patients or real patients in structured training scenarios may represent a promising, contextually relevant alternative to traditional simulation approaches and warrants further investigation.
Regarding empathy-focused interventions, this review identified improvements in empathy but not in ageist attitudes, which contrasts with the findings reported by Martínez-Arnau et al.21 Differences in measurement instruments may partly explain this discrepancy. Studies included in Martínez-Arnau et al. relied on broader measures, such as the Aging Semantic Differential or empathy-specific scales, which may capture general attitudinal change toward older adults rather than ageism specifically.21 Beyond measurement issues, recent evidence suggests that empathy-based interventions yield inconsistent effects, possibly because empathy can be elicited through different mechanisms, including cognitive perspective-taking and affective emotional responses, each of which may have distinct implications for attitude change.43 These findings suggest that improvements in empathy alone may be insufficient to reduce ageist attitudes, as the cognitive components underlying age-based stereotypes may require more targeted interventions. Future research should therefore consider integrating empathy-based approaches with structured components, such as gerontological education, to achieve more consistent and meaningful reductions in ageism among both students and healthcare professionals.21, 41, 42, 43
Limitations of the study
This review has several important limitations that should be considered when interpreting the findings and extrapolating their applicability to real-world healthcare settings.
First, the temporal restriction to the last 5 years may have excluded earlier methodologically robust studies or pioneering interventions that could provide relevant evidence on effective strategies to reduce ageism. This temporal limitation was applied to focus on recent evidence in a context marked by substantial changes in healthcare education after the pandemic, the wider adoption of active learning methodologies such as clinical simulation and experiential learning, and increased institutional attention to empathy and person-centered communication. However, to mitigate this limitation as far as possible, the findings of the systematic reviews by Martínez-Arnau et al. and Burnes et al., which included studies in students and the general population, respectively, up to 2020, were taken into account when analyzing the results and drawing conclusions.19, 21
Second, among the included studies, there is considerable heterogeneity in the interventions, which yields disparate results that are difficult to interpret in real settings. The vast majority of interventions were conducted with students, and only 1 RCT involved practicing nurses. These results raise important questions about ecological validity and transferability: attitudes formed in academic environments may not withstand the structural pressures, time constraints, and institutional cultures of real clinical settings, where age-based discriminatory practices are often embedded in routines and protocols. Because the available evidence primarily evaluates students in educational contexts, findings cannot be assumed to transfer directly to clinical environments.
Third, with respect to study methodology, the more robust effects tend to come from studies with adequate designs, such as those by Miranzadeh et al.34 In contrast, the inclusion of uncontrolled studies31, 38 or pre–post designs without longer follow-up28, 31, 36 may have led to overestimation of effects. Likewise, many studies did not employ robust analyses of temporal interaction, which limits direct causal attribution.28, 29 These methodological shortcomings have been noted in previous reviews of anti-ageism interventions, which call for greater rigor and standardization.5, 19
Moreover, the primary outcome (ageism) was assessed almost exclusively using self-report scales (e.g., Jefferson Scale of Empathy (JSE), KAOP, Age Discrimination Attitude Scale (ADAS), CENVE), limiting direct comparability across studies and potentially introducing reporting bias. Importantly, the impact of these interventions on actual clinical behavior in care settings remains poorly documented. A broader systematic review suggests that, although attitudes and knowledge may improve following intervention, corresponding changes in clinical practice and their impact on the care of older adults remain insufficiently studied and largely unproven.19 Consequently, the real-world impact of these interventions on professional conduct in clinical settings remains uncertain and warrants further investigation using objective, behavior-based outcome measures.
Nevertheless, our findings provide novel evidence on the effectiveness of interventions to reduce ageism among both healthcare students and professionals. Further research is needed to deepen understanding of the mechanisms underlying ageist attitudes, beliefs, and behaviors in healthcare contexts and to develop methodologically robust studies capable of more accurately determining the effectiveness of such interventions in clinical practice.
Implications for practice
The findings of this review offer several tentative implications for both educational and clinical practice, though these should be interpreted cautiously given the methodological limitations of the available evidence.
In academic settings, integrating aging-related content more consistently into the core curricula of health sciences programs may help reduce ageist attitudes among future professionals. Educational programs may benefit from incorporating multiple components that combine gerontological theory, clinical simulation, intergenerational contact, and structured reflection.
From an organizational perspective, healthcare institutions might consider prioritizing continuing professional development initiatives that build on pedagogical components with the greatest promise in the existing literature, particularly structured gerontological education. Nevertheless, evidence from interventions targeting qualified healthcare professionals remains critically scarce, and further research is needed before these approaches can be confidently recommended for widespread implementation in clinical settings.
Future research should address current methodological limitations by implementing multicenter RCTs with follow-up periods of 6–12 months and by incorporating behavioral and performance-based outcome measures to determine whether attitudinal changes translate into sustained improvements in the quality of care provided to older patients.
Conclusions
Interventions based on theoretical education, alone or combined with clinical simulation, and/or intergenerational contact show the greatest potential to reduce ageism among students and healthcare professionals. However, the available evidence remains heterogeneous and largely derived from student populations. Future research should prioritize the development and evaluation of methodologically robust interventions targeting practicing healthcare professionals, building on pedagogical components identified in student populations, to determine whether improvements in attitudes toward older patients translate into sustained improvements in the quality of care.
Use of AI and AI-assisted technologies
Not applicable.