















Abstract
Adherence is defined as taking medications as prescribed to achieve a therapeutic outcome. It consists of 3 main components: initiation, implementation, and discontinuation. Methods of assessing adherence can be broadly classified as direct or indirect. Factors influencing adherence include patient-related, therapy-related, and healthcare system-related variables. Poor adherence in chronic disease management leads to a cascade of negative clinical, economic, and psychosocial outcomes. Evidence consistently demonstrates that non-adherence is not merely a patient-level issue but a systemic healthcare challenge. Effective strategies to improve adherence must therefore be comprehensive, targeting barriers at multiple levels to achieve meaningful improvements in patient outcomes and quality of life. These strategies include supporting the initiation phase, improving implementation, and addressing challenges related to treatment discontinuation. This paper presents key findings from a literature review on adherence and its importance in clinical practice, as well as current and emerging strategies to enhance medication adherence among patients with chronic diseases.
Key words: implementation, adherence, chronic disease, new technologies, discontinuation
Introduction
The global burden of chronic diseases, such as diabetes, hypertension, chronic obstructive pulmonary disease (COPD), and depression, continues to rise, significantly impacting public health systems worldwide. In recent decades, the prevalence of chronic diseases has steadily increased, driven by aging populations and improvements in healthcare that have reduced premature mortality.1, 2 Effective management of these conditions depends largely on patient adherence to prescribed medication regimens, which is critical for achieving therapeutic success, preventing complications, and improving quality of life.3
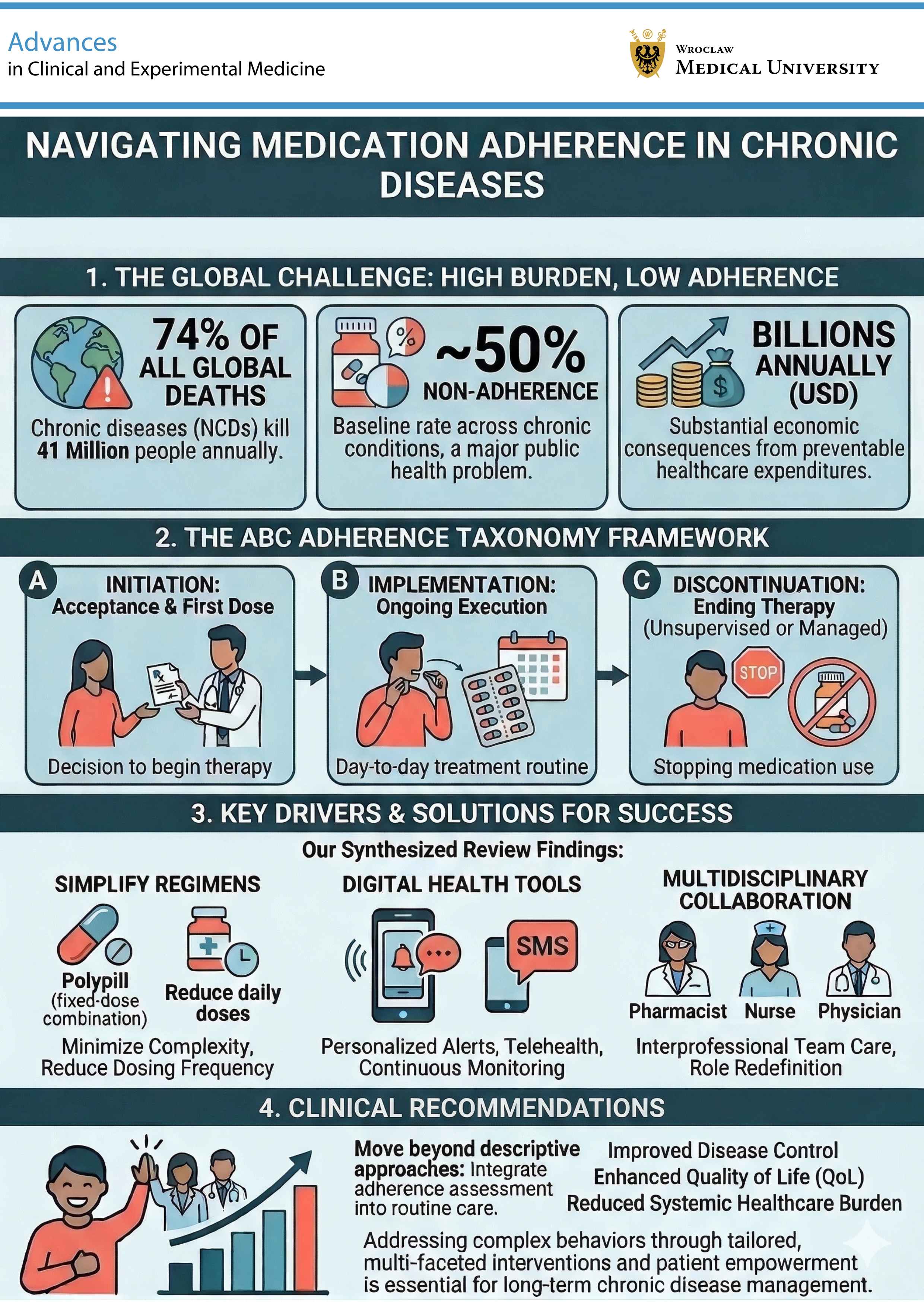
Despite the availability of highly effective treatments, medication adherence remains suboptimal, with rates often falling below 50% among patients with chronic conditions such as hypertension, diabetes, and depression.4, 5, 6, 7 This gap significantly contributes to poor disease control and is associated with increased healthcare costs, hospitalizations, and preventable morbidity and mortality.8, 9, 10 For example, medication non-adherence in patients with hypertension is linked to poor blood pressure control, increased cardiovascular complications, and higher overall mortality.11, 12
Medication adherence is a complex phenomenon influenced by multiple factors, including patient beliefs, treatment complexity, healthcare systems, and socio-economic contexts. Understanding this complexity is essential for developing effective strategies to address this issue.13, 14 Several innovative approaches have emerged to improve and accurately measure medication adherence. These include electronic monitoring devices, mobile health applications, ingestible biosensors, and artificial intelligence (AI)-driven technologies, all of which hold promise for improving measurement accuracy and clinical outcomes.15, 16, 17, 18
Objectives
The primary objective of this review is to address the persistent gap between therapeutic efficacy and real-world effectiveness in chronic disease management caused by suboptimal medication adherence. Specifically, this review aims to: 1) integrate existing evidence within a phase-based ABC framework; 2) critically examine determinants and measurement approaches; and 3) translate evidence into structured, phase-specific clinical strategies. By doing so, we seek to move beyond descriptive synthesis and provide an analytically grounded framework for improving adherence in clinical practice.
Review design and search strategy
This narrative review was aimed at synthesizing evidence on medication adherence and persistence in chronic diseases. The objective was to integrate biomedical, psychological, technological, and healthcare system perspectives within a unified conceptual framework based on the ABC adherence taxonomy (initiation–implementation–discontinuation).
Search strategy
A structured literature search was performed in MEDLINE (via PubMed), Scopus, and APA PsycInfo. The search covered publications from January 2001 to December 2025, ensuring the inclusion of both foundational adherence frameworks and recent developments in digital monitoring and long-acting therapies.
Search terms were combined using Boolean operators (AND/OR) and included: (“medication adherence” OR “treatment adherence” OR “persistence”) AND (“chronic disease” OR “hypertension” OR “diabetes” OR “cardiovascular disease” OR “heart failure” OR “COPD” OR “depression” OR “multimorbidity”) AND (“adherence measurement” OR “MMAS” OR “MARS” OR “BMQ” OR “MEMS” OR “MPR” OR “PDC”) AND (“motivational interviewing” OR “shared decision making” OR “digital health” OR “mHealth” OR “long-acting” therapy OR “polypill”).
Reference lists of included studies were manually screened to identify additional relevant publications. All records were imported into Zotero for reference management and deduplication. Additionally, seminal publications describing widely used adherence questionnaires published before 2001 (e.g., 1986 and 1999) were identified through manual reference screening and included to ensure appropriate conceptual and methodological context.
Eligibility criteria
Inclusion criteria: peer-reviewed articles; adult populations with chronic diseases; studies focusing on adherence definitions, determinants, measurement, outcomes, or interventions; English language; and full-text availability. Exclusion criteria: pediatric-only studies; non-peer-reviewed commentaries without data; and abstract-only publications. Due to the narrative design, no formal quality scoring system (e.g., GRADE) was applied; however, study types and methodological strength were considered during interpretation.
Understanding adherence
Definitions of medication adherence and persistence
Adherence is defined as taking medications as prescribed to achieve a therapeutic outcome. It refers to the extent to which patients take their medication as recommended and continue to do so. It depends on effective collaboration between the patient and the healthcare provider, as well as the patient’s active involvement in their treatment.19, 20, 21 Persistence is defined as the duration of time from initiation to discontinuation of therapy. It is operationalized in several ways, including the time to treatment discontinuation, the number of prescription refills, the proportion of patients with a specified days’ supply of medication, and the proportion of patients continuing treatment over a defined period.19, 22, 23 Both adherence and persistence are crucial for evaluating the effectiveness and cost-effectiveness of therapy.23, 24, 25
Phases of adherence
The process of adherence consists of 3 main components19: 1) Initiation: This stage refers to the start of therapy, defined as taking the first dose of a prescribed medication. Measuring initiation provides important information on primary non-adherence in both acute and chronic conditions. 2) Implementation: This phase reflects the extent to which a patient’s actual dosing corresponds to the prescribed regimen over time. It includes taking medications as prescribed and, where relevant, following recommended lifestyle modifications such as diet and physical activity. 3) Discontinuation: This stage refers to the point at which a patient stops taking the prescribed medication, thereby marking the end of therapy.21
Methods of measuring adherence
Methods for assessing medication adherence can be broadly classified as subjective or objective, as well as direct or indirect. Subjective methods involve assessing adherence behavior through patient or clinician reports, most commonly using questionnaires. Objective methods include pill counts, pharmacy refill records, and electronic medication monitoring, which provide more reliable estimates of adherence.26, 27, 28 Direct methods involve the measurement of drug or metabolite concentrations in biological fluids or the use of digital pills.29, 30 Indirect methods, which are more commonly used in adherence research, include self-reported measures, pill counts, pharmacy records, and electronic monitoring systems such as the Medication Event Monitoring System (MEMS).27, 31, 32, 33, 34, 35
Direct methods
Mobile health applications support medication adherence by providing features such as medication reminders, real-time monitoring,36, 37, 38 and opportunities for timely interventions.36, 37, 38, 39, 40 In patients with chronic diseases, including diabetes and cardiovascular conditions such as heart failure or chronic coronary syndrome, these tools can facilitate adherence by supporting treatment monitoring and self-management. However, most digital solutions are designed for single-drug administration, which may be challenging for patients with polypharmacy. Older adults are particularly vulnerable due to age-related comorbidities and complex treatment regimens.37, 41, 42
Direct methods of adherence assessment include the measurement of drug or metabolite concentrations in biological fluids and direct observation of medication intake. Measurement of drug concentrations in blood or urine is considered one of the most reliable methods.43, 44, 45, 46 High-performance liquid chromatography with tandem mass spectrometry (HPLC–MS/MS) is commonly used due to its high sensitivity, specificity, and selectivity.47, 48, 49 This approach allows for quantification of drug levels, which can be used to optimize dosing or estimate the timing of the last dose. However, it is costly and technically demanding.29, 30 Directly observed therapy (DOT) involves monitoring medication intake by healthcare professionals and may be effective in controlled settings, such as hospitals. However, it is often impractical in routine care and may be subject to behavioral bias.37, 42
Digital pills represent an emerging direct method of adherence assessment. These systems use ingestible sensors that transmit a signal upon ingestion, which is then detected by a wearable device and transferred to a mobile application accessible to both patients and healthcare providers.38, 50 Although they provide precise information on the timing of medication intake, their use is currently limited by cost and accessibility.42
Indirect methods
Questionnaires are standardized self-assessment tools used to assess adherence to a specific treatment regimen, as well as to identify disadvantages, beliefs, and knowledge about the disease and its treatment.51, 52 The most commonly used scales are the Morisky Medication Adherence Scale (MMAS-8),53 the Medication Adherence Reporting Scale (MARS),54 the Medication Beliefs Questionnaire (BMQ),55 the Medication Adherence Self-Efficacy Scale (MASES),56 and the Adherence to Refills and Medications Scale (ARMS).57 Self-assessment questionnaires are characterized by ease of administration, low cost, rapid feedback at the point of care, and ease of adaptation to different patient populations.37, 42, 52, 58, 59, 60, 61
MMAS-8 is the most commonly used scale due to its high sensitivity, specificity, validity, and reliability.62, 63 Initially, it was a 4-item scale,53 but it now consists of 8 questions, the first 7 of which are yes/no questions and the last of which uses a 5-point Likert scale. It has been used in randomized controlled trials (RCTs) to assess medication adherence in patients with chronic diseases.64 MARS is used for its ease of use.65, 66, 67 It is based on the Medication Attitudes Inventory, also known as the Drug Attitude Inventory (DAI), and the Medication Attitudes Questionnaire (MAQ), and assesses beliefs and barriers to medication adherence and overall disease control over the past week.68 MARS-5 and MARS-6 were developed for use in asthma, chronic obstructive pulmonary disease, diabetes, and rheumatoid arthritis.65, 66, 67 The BMQ provides information on general and specific needs and beliefs regarding medications. It is not intended for self-administration and requires a different measurement method. It has been used in patients with asthma, diabetes, mental disorders, and cardiovascular disease.69
A central electronic pharmacy register identifies the prescription issued by the physician and the date on which the patient filled it. The register is designed to ensure that prescriptions are filled accurately based on patients’ actual medication use.70 The register enables the identification of reasons for treatment discontinuation, e.g., due to adverse drug reactions.27, 31, 32, 33, 34, 59, 70 The most commonly used parameters in pharmacy databases are the medication possession rate (MPR) and the percentage of days covered by a prescription (PDC). The MPR is the share (or percentage) of days of drug availability obtained within a specific time period or between subsequent prescriptions. The PDC is a measure of the number of days of drug availability divided by the number of days in the study period.27, 71, 72
Electronic monitoring devices, such as the Medication Event Monitoring System (MEMS), store medication dosing history, including the date and time when the container was opened.73 They provide information on the number of doses taken and the intervals between doses. They are characterized by high accuracy and precision in data recording.73, 74, 75 Improper use of the device or opening the medication container without taking the medication can lead to false results.15, 37, 38, 51, 59, 60, 76 They can be inaccurate and do not account for missed doses or intervals between doses.77
The use of advanced AI devices to monitor medication adherence holds potential. These devices, equipped with multimodal sensors and AI-based analytics, enable real-time monitoring of physiological and biochemical parameters such as cardiac activity, glucose levels, and biomarkers, facilitating early disease detection, chronic disease management, and precision therapy. However, their widespread implementation still faces technical, ethical, and regulatory hurdles, including privacy concerns and algorithmic bias.78, 79
Factors influencing adherence
Medication adherence is best understood within a biopsychosocial and socioecological framework, where behavior emerges from interactions between individual characteristics (beliefs, personality, cognition), therapy-related factors (complexity, side effects), interpersonal influences (family, caregivers), healthcare system structures, and broader socioeconomic determinants.80 This multi-layered perspective aligns with the expanded ABC adherence model and allows the integration of clinical, psychological, and policy-level dimensions discussed in this review. Adherence is a complex phenomenon influenced by multiple factors; understanding these factors is crucial for implementing appropriate interventions.
Patient-related factors
Researchers from the Czech Republic recently presented the results of a study involving a population of over one million statin users. They found that adherence increases with age. Furthermore, male gender was associated with higher adherence.81 A study conducted in the USA on a group of individuals aged at least 35 years with diagnosed cardiovascular disease found that older age, male gender, and a diagnosis of hypertension were associated with significantly better adherence to statin use.82
Another multicenter study noted that smoking at hospitalization and negative affectivity were significantly associated with reduced statin adherence, regardless of the methodology used to assess adherence.83 Researchers from the UK conducted a study analyzing data from 76,000 UK Biobank participants and demonstrated the influence of specific genetic variants on statin adherence.84
A study conducted in Bahrain (209 patients) found young age, being single, not having regular blood pressure checks, and no family history of hypertension to be associated with lower adherence to antihypertensive medication.85 A study performed in Pakistan on a larger population (32,197 hypertensive patients) found male gender and graduate education compared to post-graduate education to be factors predisposing to greater adherence.86 According to another study, better adherence to antihypertensive medication was associated with more frequent blood pressure self-monitoring, a reduced salt intake, fewer daily supplements, more frequent reading of medication leaflets, and the receipt of specific information from pharmacists.87 It therefore seems that a greater interest in taking care of one’s health and a concern for one’s knowledge promote adherence. It is confirmed by a study conducted in Ethiopia, which found that college and higher education levels, as well as knowledge about hypertension, were associated with better adherence to antihypertensive medications.88
A study conducted in Peru among elderly individuals found that adherence to antihypertensive medication increases with age and stroke. However, no significant association was found with gender.89 On the other hand, a meta-analysis of statin adherence in individuals aged 65 years or older found that adherence was lower in those aged 75 years or older compared to those aged 65–75 years.90 It is important to note that findings regarding demographic determinants such as age and gender remain inconsistent across studies. These discrepancies may reflect differences in adherence definitions (self-report vs objective refill data), population characteristics, healthcare system context, and study design. Therefore, demographic predictors should not be interpreted as universal determinants but rather as context-dependent modifiers influenced by cultural and systemic factors.
Therapy-related factors
According to the results of an extensive study conducted in Japan, adherence to statin use is higher in patients receiving secondary prevention than in those receiving primary prevention.91 Researchers from New Zealand reached a similar conclusion.92 The same conclusions were also reported for acetylsalicylic acid. In secondary prevention, median adherence rates were 60% in Germany and 75% in the UK, while in primary prevention they were 50% in both countries.93 This may be explained by the fact that patients who have already experienced symptoms are more motivated to prevent them in the future. Moreover, adherence to statins was found to be higher in previously treated patients than in those newly started on treatment.94 High-intensity statin use has also been shown to be associated with better adherence.81, 82
Healthcare system-related factors
According to an American study, the use of the Statin Choice program was associated with a 5.75% increase in the likelihood of primary adherence (assessed 60 days after initiation). After 1 year, the effect of Statin Choice use was significant in univariate analysis but was not statistically significant after adjustment for patient-related factors.94 It has also been found that being under the care of a cardiologist promotes adherence to statin use.82 According to a study conducted in Ethiopia, having health insurance coverage, living within 10 km of a healthcare facility, and having social support were associated with better adherence to antihypertensive medications.88
Clinical “red flags” of non-adherence in practice
Assessing adherence for a specific patient is difficult but crucial in patient care. The search for objective methods to diagnose non-adherence is essential, as it has been shown that physicians’ intuition and experience have low sensitivity in identifying patients with non-adherence.95 Questionnaires dedicated to assessing adherence may be helpful in everyday clinical practice, but it should be noted that in some cases they may lead to overestimation.60 The most accurate method is to determine the concentration of prescribed medications in the blood or to check prescription refills in the patient’s electronic medical records.96, 97 However, it would be difficult to perform such tests in all patients, as this would be time-consuming and costly. As part of the initial assessment, it is worthwhile to verify the pharmacotherapy regimen declared by the patient and to inquire about their satisfaction with the treatment.96
Consequences of poor adherence
Adherence to prescribed pharmacological regimens is a cornerstone of effective chronic disease management. Poor adherence undermines therapeutic efficacy, compromises disease control, and contributes to increased morbidity, mortality, and healthcare costs. The consequences extend beyond the clinical sphere, affecting psychosocial wellbeing, quality of life, and healthcare system efficiency.
Clinical consequences
The most immediate impact of poor adherence is suboptimal disease control. In hypertension, low adherence is consistently associated with inadequate blood pressure management, leading to progressive target organ damage, including left ventricular hypertrophy and microalbuminuria.12 In diabetes mellitus, non-adherence results in persistent hyperglycemia, which accelerates the development of microvascular complications (nephropathy, retinopathy) and macrovascular outcomes (myocardial infarction, stroke).10 Cardiovascular diseases demonstrate particularly severe consequences. Premature discontinuation of statins or antihypertensive agents is associated with higher rates of recurrent myocardial infarction, stroke, and progression of heart failure.98 In chronic kidney disease, inadequate adherence to nephroprotective therapy accelerates the decline in renal function, hastening progression to end-stage renal disease.99 The interplay of comorbidities compounds the clinical burden. For example, in patients with both hypertension and diabetes, poor adherence simultaneously increases cardiovascular and renal risk, creating a synergistic deterioration in health status.13
Increased healthcare and economic burden
Non-adherence results in a measurable increase in healthcare burden. Patients with low adherence are more likely to require emergency interventions, hospital admissions, and longer inpatient stays.100 In a seminal study, Sokol et al. demonstrated that patients with poor adherence had significantly higher hospitalization rates and incurred substantially greater healthcare costs compared to adherent patients.8 From an economic perspective, non-adherence represents a major inefficiency in healthcare delivery. In the USA, annual costs attributable to poor adherence are estimated to be between $100 billion and $300 billion, with a substantial proportion resulting from avoidable disease complications.101 Similar trends have been reported in European healthcare systems, where the economic impact extends beyond direct medical costs to include lost productivity, disability benefits, and caregiver burden.102
Mortality and morbidity
Poor adherence is strongly associated with higher mortality and morbidity across chronic diseases. A meta-analysis involving over 27 million patients with hypertension demonstrated a significant link between low adherence and increased cardiovascular mortality.11 In diabetes, reduced adherence predicts not only earlier mortality but also a greater frequency of acute complications, such as diabetic ketoacidosis and hyperosmolar hyperglycemic states.103 In heart failure, suboptimal adherence to guideline-directed therapy is a leading predictor of preventable hospital readmissions and premature death.104 These patterns are consistent across other chronic conditions, underscoring the universality of adherence as a determinant of long-term outcomes.
Qualitative impacts: quality of life and psychosocial burden
While clinical and economic metrics are crucial, qualitative outcomes – particularly health-related quality of life (HRQoL) – are equally important. Poor adherence often leads to symptom exacerbation, reduced physical functioning, and a diminished ability to perform daily activities.105 In hypertension, e.g., low adherence is independently associated with lower HRQoL scores, even after adjusting for blood pressure levels.9 Psychosocial consequences are also substantial. Patients experiencing worsening symptoms due to non-adherence frequently report increased anxiety, depression, and social isolation. In chronic pain syndromes, irregular medication use leads to heightened pain intensity and reduced participation in social and occupational activities.106 Non-adherence also has ripple effects on family members and caregivers, who may experience increased emotional strain, financial burden, and disruption to their daily lives. These indirect impacts contribute to the overall societal cost of poor adherence, although they are less frequently quantified in research.107
System-level implications
At the healthcare system level, poor adherence undermines disease prevention strategies and the cost-effectiveness of treatment protocols. It erodes the return on investment in public health interventions and pharmaceutical innovations, as the full benefits of therapy are not realized without sustained patient engagement.108 Addressing this challenge requires a multifaceted approach that includes patient education, behavioral support, regimen simplification, and the integration of adherence monitoring into routine care.33
Additional factors influencing psychology of adherence
Psychological and behavioral factors influencing adherence
Adherence is a multifactorial phenomenon influenced by a complex interplay of patient-, therapy-, and healthcare system-related factors. Among these, internal psychological factors are particularly decisive, forming the foundation of motivation for long-term disease management. Qualitative studies reveal that initial motivation is driven by 2 key components: “alertness” and “willingness.” Alertness is the realization of the disease’s severity and potential consequences, often described as an urgent need to seek help. Willingness is the conscious decision to continue treatment after understanding its necessity. Patients with this internal readiness are more likely to engage in the therapeutic process and perceive it as a way to regain control.
The Health Belief Model (HBM) provides a useful framework for understanding these internal beliefs.109 The model posits that a patient’s decision to adhere is influenced by their perceptions of:
– Perceived susceptibility: The perceived risk of developing the disease or its negative outcomes.
– Perceived severity: The perceived seriousness of the disease.
– Perceived benefits: The belief that the prescribed therapy will be effective.
– Perceived barriers: The obstacles to taking the medication, such as cost or side effects. It is a powerful predictor of non-adherence.
– Self-efficacy: The belief in one’s own ability to successfully perform the task of taking medication. It is a modifiable factor and one of the strongest predictors of adherence.
Evidence supports the utility of the HBM; interventions based on this model, such as educational programs, have successfully improved adherence by enhancing patients’ self-efficacy and their perception of benefits.110
Personality also plays a significant role in health behaviors. The Five-Factor Model of Personality (the Big Five) provides a framework for analyzing this relationship. The strongest and most consistent predictor of good adherence is conscientiousness, characterized by discipline, organization, and a sense of duty. Conversely, neuroticism is a strong negative predictor, as emotional instability and anxiety can lead to a focus on potential side effects and deplete the motivation needed for systematic treatment. Understanding a patient’s personality profile enables the delivery of personalized interventions. For example, a patient with low conscientiousness may benefit from practical tools like pill organizers, while a highly neurotic patient may require more support in managing their anxiety.111
Depression is one of the most serious and common risk factors for non-adherence. A systematic review has shown that the odds of non-adherence are 1.76 times higher in patients with depression.112 The impact of depression is multidimensional, affecting both cognitive and motivational functions. Cognitive deficits, particularly in executive functions (such as planning and organizing) and prospective memory (remembering to take medication), directly hinder adherence. Motivational symptoms such as apathy, anhedonia, and hopelessness undermine the very drive to engage in self-care. This highlights that adherence is not merely a matter of willpower but a process dependent on intact cognitive and motivational abilities.112
Shifting from information-based to patient-centered interventions
Traditional psychoeducation, which operates on the “knowledge deficit” paradigm, has proven largely ineffective in producing lasting behavioral change. While it may increase a patient’s knowledge, it often fails to address the underlying psychological barriers, such as ambivalence, low motivation, or feelings of hopelessness. Patients may know what they should do but lack the internal drive to translate that knowledge into action.113
In response, Motivational Interviewing (MI) has emerged as a patient-centered, evidence-based standard for communication. It is a collaborative, goal-oriented style of communication designed to strengthen a person’s own motivation for change. Instead of telling the patient what to do, the clinician helps them explore their own reasons for change. Motivational Interviewing’s philosophy is rooted in partnership, acceptance, and compassion. Meta-analyses confirm the effectiveness of MI in improving adherence across various chronic diseases.114 Its effectiveness is based on specific communication skills (OARS): open-ended questions, affirmations, reflections, and summaries. By shifting the focus from “how to do it” to “why I want to do it”, MI builds a lasting foundation for behavior change.115
Strategies to improve adherence
Effective interventions to enhance medication adherence should address the distinct challenges posed by each phase of the adherence process – initiation, implementation, and discontinuation. In fact, each stage is characterized by unique psychological, behavioral, and structural obstacles that warrant phase-specific strategies.116 In chronic diseases, where long-term pharmacotherapy is often essential for symptom control and the prevention of disease progression, poor adherence can significantly undermine clinical outcomes. Therefore, improving adherence is not only a matter of individual behavior change but also of optimizing healthcare communication, system-level support, and multidisciplinary collaboration.
Supporting the initiation phase
During the initiation phase, patients often grapple with doubts about the necessity of the medication, fear of side effects, or a limited understanding of the disease and its progression.117 Interventions at this stage aim to foster acceptance of the treatment plan, address perceptual barriers through shared decision-making, and enhance motivation using techniques such as motivational interviewing, which has shown promise in facilitating the uptake of the first dose. Evidence suggests that non-initiation is frequently driven not by forgetfulness or logistical constraints but by intentional decisions rooted in ambivalence, low perceived necessity, or concerns about long-term dependency or adverse effects.31 Therefore, clinicians must prioritize open, empathetic communication early in the treatment pathway. Shared decision-making (SDM) encourages patients to express their preferences and concerns, fostering a sense of partnership and autonomy that enhances engagement.118 Moreover, SDM has been shown to reduce decisional conflict and increase initial medication acceptance, particularly when patients are supported in understanding the rationale, expected benefits, and safety profile of the prescribed treatment.119
Motivational Interviewing, when applied during early consultations, helps patients explore and resolve ambivalence, drawing on their intrinsic motivations for behavior change. Studies demonstrate that MI not only improves first-dose uptake but also reinforces the patient’s sense of self-efficacy and commitment to the therapeutic regimen.120 Integrating MI principles with brief educational components tailored to the patient’s literacy and readiness to change can be particularly effective.121 Additionally, involving other members of the healthcare team, such as nurses and pharmacists, can provide multiple touchpoints for reinforcing the importance of treatment initiation and addressing remaining doubts.
Additional strategies in the initiation phase include reducing financial barriers – such as waiving copayments and providing starter packs – which have been shown to significantly reduce prescription abandonment and improve initiation rates.122 Electronic prescribing with integrated “first-fill” reminders can increase initial prescription pick-up, streamlining the transition from prescription to action.123 Finally, social and caregiver support – such as inviting a family member to the first consultation or setting up shared reminders – can significantly increase the odds of adherence by reinforcing the patient’s routine and confidence.124, 125
Overall, the initiation phase represents a critical window of opportunity to lay the foundation for long-term adherence by establishing trust, clarifying misconceptions, and aligning treatment with patient values and goals.
Improving the implementation phase
Once the first dose has been taken, the focus shifts to sustaining day-to-day execution of the treatment plan – ensuring each subsequent dose is taken at the right time, in the right way, and for as long as clinically indicated. In the implementation phase, where patients are expected to take medications consistently and correctly over time, challenges are typically related to forgetfulness, regimen complexity, declining motivation, or life disruptions.125 To address these barriers, various evidence-based strategies have been proposed. Aligning refill dates (medication synchronization) and supplying medicines in calendar blister packs together provides a straightforward way to reduce forgetfulness and can increase adherence by approx. 4–21 percentage points.126, 127 Digital interventions – such as mobile health apps, SMS reminders, wearable devices, and interactive voice response systems – offer scalable tools for prompting medication-taking, tracking adherence patterns, and facilitating real-time feedback between patients and providers. When integrated into the care plan, these tools have been shown to significantly improve implementation adherence, especially when tailored to patient preferences and literacy levels.128, 129, 130
Simplification of therapeutic regimens also plays a critical role. Fixed-dose combinations (e.g., polypills) reduce pill burden and dosing frequency, while long-acting formulations (e.g., injectables, depot medications, extended-release tablets) minimize the need for daily adherence. Both strategies have demonstrated positive effects on adherence and clinical outcomes, particularly in cardiovascular and psychiatric conditions.131, 132
In parallel, behavioral and habit-forming interventions – such as implementation intentions, routine linking (e.g., taking medication with a daily task), and adherence contracts – have been shown to improve consistency by embedding medication use into existing behavioral patterns.133, 134 These can be further supported by motivational reinforcement strategies, such as digital feedback or gamification, to enhance the effectiveness of the approach.
Ultimately, multidisciplinary care teams, comprising pharmacists, nurses, and case managers, are crucial in supporting the implementation phase. Their roles include conducting medication reviews, providing personalized counseling, identifying barriers to adherence, and coordinating follow-up. Regular check-ins enable the early identification of non-adherence, allowing for timely intervention before clinical deterioration occurs. For example, pharmacist-led telephone follow-ups in a population of non-adherent hypertensive patients with diabetes significantly increased adherence and reduced discontinuation rates during the subsequent 6 months.135 When paired with shared decision-making and patient empowerment approaches, this collaborative model fosters sustained engagement and better long-term outcomes.136
Addressing the challenges of treatment discontinuation
Beyond consistent daily use, long-term therapeutic success depends on preventing premature or unsupervised discontinuation of therapy and, when appropriate, guiding patients through safe, planned discontinuation. Finally, the discontinuation phase – often overlooked in both clinical practice and adherence research – requires systematic attention, as it may encompass the risks of unsupervised discontinuation (e.g., rebound symptoms, withdrawal syndromes), as well as clinical deterioration and relapse due to the loss of therapeutic benefit.
To address these challenges, long-term support is crucial. Interventions in the discontinuation phase should include periodic treatment reviews, enabling clinicians to assess the ongoing necessity, tolerability, and medication adherence. Such reviews are also essential for identifying early signs of disengagement, side effects, or declining motivation.137 Open communication is a key aspect: patients should be encouraged to express concerns about burden, doubts about long-term benefit, or adverse experiences. Clinicians, in turn, must validate these concerns and collaboratively explore solutions, including dose adjustments, alternate formulations, or temporary pauses with follow-up.138, 139
For patients at risk of stopping therapy on their own, long-term motivational support – delivered through structured follow-up, digital tools, or team-based care – can help sustain engagement.140 Peer support, caregiver involvement, and patient education about the consequences of unmonitored discontinuation may also reinforce treatment persistence.
In cases where discontinuation is clinically appropriate, the process should be managed with structured tapering plans, clear instructions, and ongoing monitoring for withdrawal symptoms, recurrence, or rebound effects. However, when discontinuation occurs outside of clinical supervision – due to missed refills, treatment fatigue, or disengagement – re-engagement strategies become crucial. One such approach is the use of “Data to Care” programs, which leverage routinely collected data from electronic health records or pharmacy claims to identify patients who have silently discontinued therapy. These systems trigger outreach – via phone calls, SMS, or case manager follow-up – to reestablish contact, assess barriers, and reinitiate or adjust treatment as needed. Such programs have proven effective in HIV care and are increasingly adapted for chronic disease management, offering a scalable solution to mitigate the risks associated with unmonitored discontinuation.141 Pharmacovigilance during and after cessation is essential to ensure patient safety and to reinitiate treatment if necessary.142 Ultimately, by actively managing the discontinuation phase, clinicians can reduce unintended harm, optimize treatment trajectories, and maintain trust in the therapeutic alliance.143
Cross-phase financial and policy levers
Financial policies – such as insurance plans that waive copayments for high-value drugs and offer 90-day mail-order supplies – support every step of adherence across the entire ABC continuum. By lowering the financial burden at initiation, simplifying refills during implementation, and encouraging sustained therapy in the persistence phase, these measures reinforce each patient-level intervention and add a system-level boost.144
Moreover, aligning reimbursement models with adherence goals, such as value-based care incentives or medication therapy management programs, can further integrate adherence promotion into routine practice. By reinforcing patient-level interventions with supportive financial and systemic structures, these levers provide a sustainable and scalable foundation for improving adherence outcomes in chronic disease management.
Patient-centered communication and health literacy
Patient-centered communication, which tailors information and dialogue to individual values, preferences, and comprehension levels, is fundamental for improving medication adherence in chronic diseases. A recent mixed-methods review demonstrated that tailored information, active patient engagement, and collaborative provider communication significantly enhance self-management and adherence in chronic illness.145 Health literacy – the ability to access, understand, and apply health information – remains a strong predictor of adherence. A systematic review published in 2020 confirmed a robust association between low health literacy and poor medication adherence among adults with chronic diseases, noting that health literacy interventions can improve adherence across diverse populations.146 Furthermore, communication strategies that explicitly address patient values and motivational drivers (e.g., family wellbeing, emotional concerns, financial stressors) can deepen engagement and adherence, particularly in preventive cardiology contexts.147
Adherence in special populations: focus on elderly
Older adults with chronic diseases often face unique barriers to medication adherence due to polypharmacy, cognitive decline, sensory impairments, and complex dosing regimens. These challenges can lead to confusion, missed doses, and an increased risk of adverse drug events. Tailored strategies are therefore essential to support adherence in this vulnerable population. Comprehensive geriatric assessment (CGA) can help identify adherence-related risks, including depression, mobility issues, and medication burden. Comprehensive geriatric assessment-guided interventions that incorporate pharmacy reviews and multidisciplinary input have been shown to optimize medication use and improve health outcomes in older populations.148
One of the most effective approaches is medication regimen simplification – such as de-prescribing unnecessary drugs, switching to fixed-dose combinations, and reducing dosing frequency – shown to improve adherence without compromising clinical outcomes.149 Caregiver involvement plays a crucial role in adherence support for elderly patients. Involving family members or professional caregivers in the medication routine has been associated with increased adherence to the medication regimen and reduced unintentional discontinuation.150
Key phase-specific interventions, supporting evidence, and outcomes are summarized in Table 1.
Strength of evidence and interpretation
The evidence supporting adherence interventions varies in methodological strength. While meta-analyses and RCTs provide relatively robust support for interventions such as motivational interviewing, fixed-dose combinations, and pharmacist-led follow-up, many digital health interventions are supported primarily by short-term or observational studies. Therefore, conclusions regarding technological solutions should be interpreted cautiously, particularly with regard to long-term effectiveness and cost-effectiveness in real-world settings.
Adherence and health inequities
Medication adherence is strongly influenced by socioeconomic inequalities. Limited access to healthcare, financial barriers, digital exclusion, and low health literacy disproportionately affect vulnerable populations. While digital and long-acting technologies offer innovative solutions, they may inadvertently widen disparities if access remains uneven. Future adherence strategies must incorporate equity-sensitive design and ensure that technological advancements do not exacerbate existing healthcare inequalities.
Future perspectives and ongoing challenges
The landscape of medication adherence continues to evolve rapidly, presenting both unprecedented opportunities and significant challenges that will shape the future of chronic disease management.
Development of long-acting therapies
One of the most promising frontiers lies in ultra-long-acting therapeutic formulations requiring administration only once every 3–6 months, which could virtually eliminate daily adherence concerns for certain chronic diseases. This approach builds upon the established success of existing long-acting formulations. Long-acting injectable antipsychotics have demonstrated superior adherence and clinical outcomes compared to oral formulations, with meta-analyses showing significant improvements in treatment persistence and reduced relapse rates.132 The therapeutic potential extends across cardiovascular medicine, diabetes management, and psychiatric care; however, implementation challenges include patient acceptance, adaptation of healthcare infrastructure, and consideration of pharmacoeconomic factors, such as higher upfront costs.
Real-world challenges with new technologies
Digital health interventions offer promising solutions but face substantial implementation barriers. Mobile health applications and electronic monitoring devices have demonstrated efficacy in controlled settings15, 129; however, their real-world adoption encounters significant obstacles. Digital literacy represents a significant barrier, particularly among older adults, who comprise a substantial proportion of patients with chronic diseases. Systematic reviews demonstrate that while digital interventions can improve adherence, their effectiveness is moderated by user engagement and technological accessibility.128, 140
Access disparities in underserved communities limit the reach of technology-based solutions, while concerns about data privacy and security create additional barriers to adoption. Emerging technologies, including ingestible biosensors and AI-driven platforms, hold promise but require careful attention to ethical and practical implementation challenges.16, 17
While digital monitoring systems and long-acting therapies hold promise, ethical concerns must be addressed. Continuous digital monitoring raises questions about patient autonomy, privacy, and informed consent. Additionally, the cost-effectiveness of long-acting formulations and advanced digital systems remains uncertain, particularly in publicly funded healthcare systems. Sustainable implementation requires careful evaluation of economic impact alongside clinical effectiveness.
Need for high-quality randomized trials in real-life settings
Despite the multiplication of adherence interventions, the evidence base remains limited by methodological constraints and artificial study conditions. Most research has been conducted in highly controlled environments, which may not accurately reflect routine clinical practice. Digital intervention studies, while showing promise in meta-analyses, often suffer from short follow-up periods and homogeneous study populations.130
Pragmatic RCTs embedded within existing healthcare systems are needed to evaluate not only adherence outcomes but also clinical effectiveness, cost-effectiveness, and implementation feasibility. Extended evaluation timeframes are crucial, as chronic disease management requires sustained adherence over years rather than the weeks or months typically studied.
Integrating adherence into routine care
The greatest challenge lies in integrating adherence assessment and support into routine clinical practice. Despite overwhelming evidence of the importance of adherence, systematic attention to this issue remains inconsistent across healthcare settings. The conceptualization of adherence as a clinical vital sign requires fundamental changes in clinical workflows, electronic health record systems, and provider training programs.
Healthcare organizations must develop standardized protocols for adherence assessment that are efficient and actionable within typical clinical encounters. Current reimbursement structures often fail to adequately compensate providers for time-intensive adherence support activities adequately. Value-based payment models and multidisciplinary team-based approaches show promise for supporting comprehensive adherence interventions.144
Success requires sustained commitment from multiple stakeholders and systematic transformation of healthcare delivery systems to prioritize optimal medication adherence as a fundamental component of chronic disease care. The integration must extend beyond individual encounters to encompass care coordination across multiple providers, ensuring continuity of adherence support across all points of care.
Limitations of the study
This review has several limitations. First, as a narrative review, it does not follow a systematic methodology with formal quality grading or risk-of-bias assessment. Although a structured search strategy was applied, the absence of quantitative synthesis may introduce selection bias. Second, adherence definitions and measurement approaches vary considerably across studies, limiting direct comparability. Third, many digital and technological interventions lack long-term real-world outcome data. Finally, the rapid evolution of adherence technologies means that some emerging solutions may not yet be supported by high-quality randomized evidence.
Conclusions
Medication adherence is a key determinant of successful chronic disease management, strongly influencing clinical outcomes, healthcare utilization, and mortality. Evidence shows that adherence is shaped by interacting patient-, therapy-, and system-level factors, requiring individualized rather than uniform interventions. Effective strategies center on patient empowerment, tailored education, and simplification of treatment regimens. Multidisciplinary collaboration, particularly involving physicians, pharmacists, nurses, and behavioral health specialists, enhances adherence support. Emerging digital tools and long-acting formulations offer additional opportunities but require attention to accessibility and privacy. Integrating adherence assessment into routine care is essential for improving long-term outcomes and reducing the burden of chronic disease.
Use of AI and AI-assisted technologies
Not applicable.