Abstract
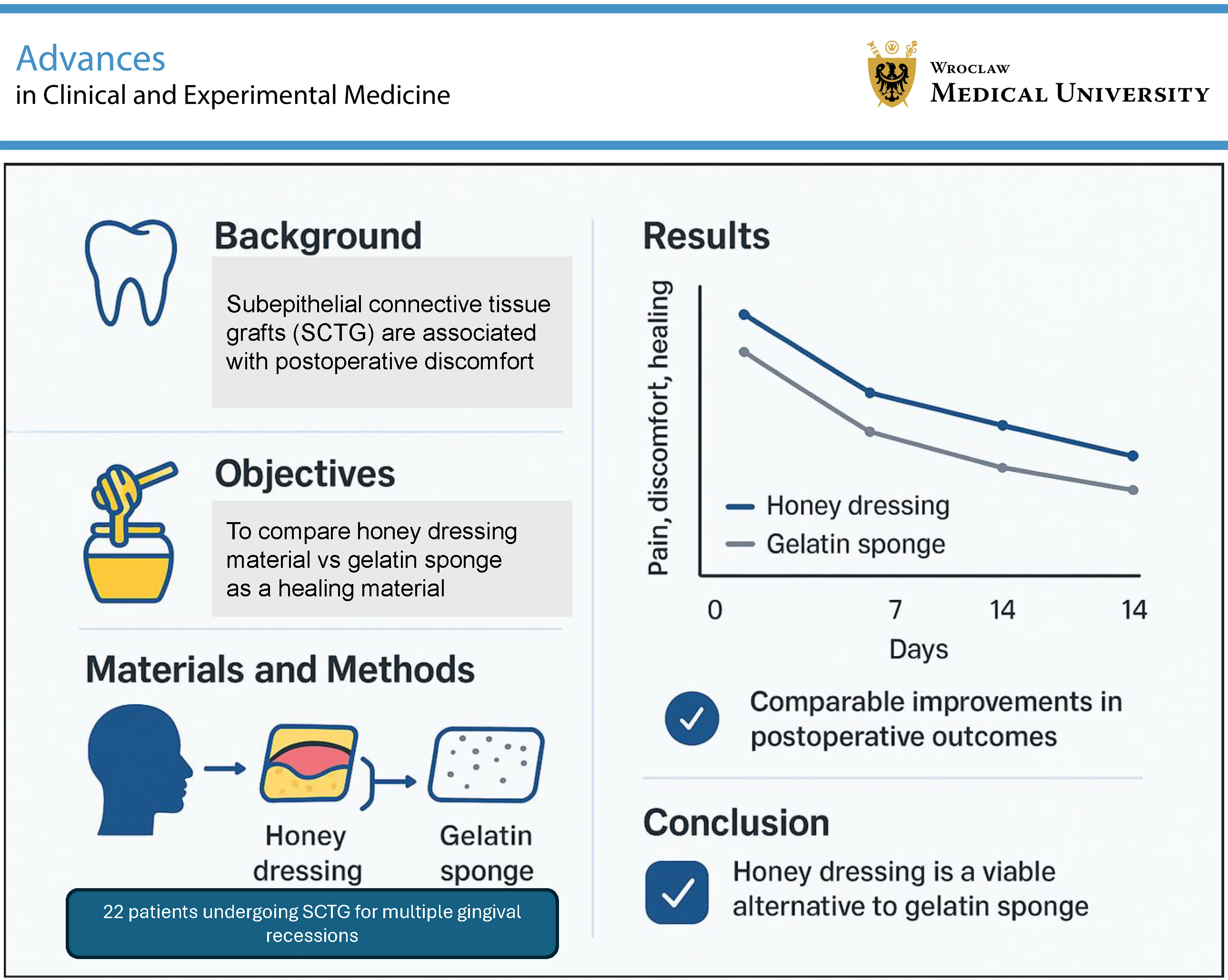
Background. Subepithelial connective tissue graft (SCTG) is commonly used in dental procedures and is associated with postoperative discomfort at the palatal donor site. The question is whether the use of a honey-based dressing may improve patients’ postoperative experience and promote wound healing.
Objectives. The aim of this study was to compare the effects of a non-adherent viscose net dressing coated with 99% Manuka honey and 1% Manuka oil (Actilite; Advancis Medical, Kirkby-in-Ashfield, UK) and an absorbable hemostatic porcine gelatin sponge (Aegis Lifesciences, Sanand, India) on the healing of the palatal donor site and patient morbidity after free gingival graft (FGG) preparation.
Materials and methods. A total of 21 patients (16 females and 5 males) with multiple gingival recessions (GR) were treated using the modified coronally advanced tunnel technique (MCAT) and subepithelial connective tissue graft (SCTG) following FGG de-epithelialization. Two grafts were harvested from both sides of the palate in each patient. Using a split-mouth design, donor sites were randomly assigned to the test group (honey dressing) or the control group (gelatin sponge). The palatal donor sites were evaluated at 1, 2, 4, 7, and 14 days postoperatively for pain, patient discomfort, changes in dietary habits, and burning sensation. Wound healing and delayed bleeding were assessed 2 weeks after surgery.
Results. In both the honey group and the gelatin sponge group, no significant differences were observed in postoperative pain, patient discomfort, burning sensation, or changes in dietary habits at 14 days postoperatively (p > 0.05). No prolonged bleeding was observed during the 2-week follow-up, and wound healing was assessed as “very good” after 14 days.
Conclusions. Both dressing materials can be successfully used at the palatal donor site after periodontal surgery and result in comparable outcomes in wound healing. Honey dressing may be considered an alternative to traditional dressing methods.
Key words: free gingival graft, palatal wound healing, honey-based dressings, periodontal surgery, postoperative pain management
Background
In periodontal plastic surgery, subepithelial connective tissue grafts (SCTGs) are widely regarded as the gold standard for the treatment of gingival recession (GR), soft tissue augmentation around implants, and gingival thickening in patients with a thin periodontal phenotype.1 The palate is the most common donor site.2, 3 Subepithelial connective tissue grafts provide predictable short- and long-term outcomes, improve aesthetics, and protect exposed roots against hypersensitivity, caries, and further recession progression. In addition, these procedures typically increase the width of keratinized tissue by approx. 1–3 mm, depending on the surgical technique, patient-related factors, and treatment site.4, 5, 6
Several techniques for harvesting SCTGs from the palate have been described.7, 8, 9, 10, 11, 12, 13 A commonly used approach is the deepithelialized gingival graft (DGG) technique, which involves harvesting a free gingival graft (FGG) followed by extraoral deepithelialization. As the palatal epithelium is removed, the donor site heals by secondary intention.3 In contrast, single-incision techniques11, 12 use a single incision to obtain the graft, are considered less traumatic than DGG harvesting, and may reduce patient morbidity by enabling primary wound healing.
Palatal harvesting may be associated with postoperative complications, including discomfort or severe pain, bleeding, infection, and, rarely, tissue necrosis at the donor site.14, 15, 16, 17 Free gingival graft harvesting is generally associated with greater early postoperative pain and bleeding than SCTG harvesting.14 Various adjunctive measures have been proposed to reduce postoperative morbidity, including hemostatic dressings,18 collagen membranes,19 low-level laser therapy,20 platelet-rich plasma,21 chemotherapeutic agents,22 and cyanoacrylate tissue adhesives.23, 24, 25 However, current evidence is insufficient to identify a single optimal approach for reducing postoperative pain and promoting early wound healing after palatal harvesting. Recently, interest in natural products for wound care has increased. Studies evaluating herbal extracts,26 keratin biomaterials,27 and ozonated oil28 have reported limited pain reduction and no clear acceleration of palatal epithelialization. In a comparative study of palatal wound management, platelet-rich fibrin, low-level laser therapy, cyanoacrylate tissue adhesives (CTA), and ozone therapy were associated with improved healing, with CTA additionally reducing pain and analgesic use.29
Species of the genus Leptospermum, native to Australia and New Zealand, are a well-known source of antibacterial honey. In the USA, these products are classified as medical-grade products and are used to maintain a moist wound environment and support the removal of infected or devitalized tissue.30 Commercially available products include Manuka honey and Medihoney, which share similar clinical applications. The dressing evaluated in this study is a non-adherent viscose mesh impregnated with 99% Manuka honey and 1% Manuka oil (Actilite; Advancis Medical, Kirkby-in-Ashfield, UK). The medical use of honey has expanded significantly, and many products have received U.S. Food and Drug Administration (FDA) clearance. Manuka-based dressings demonstrate broad antibacterial activity (including against Staphylococcus aureus, Pseudomonas aeruginosa, Stenotrophomonas, Acinetobacter, and Escherichia coli)31 and have also been reported to possess antioxidant properties.32, 33
Despite these potential benefits, evidence regarding the use of honey dressings in oral wound healing remains limited.34
Objectives
We hypothesized that the application of a Manuka honey dressing to the palatal donor site would reduce patient-reported discomfort and overall postoperative morbidity. Therefore, this study aimed to compare a Manuka honey dressing with a gelatin sponge in terms of patient discomfort and early healing at the palatal donor site following FGG harvesting.
Materials and methods
Study design and ethical considerations
This split-mouth, randomized controlled clinical trial was conducted in accordance with current standards of clinical research and is reported in line with the Consolidated Standards of Reporting Trials (CONSORT) statement. The trial was registered at ClinicalTrials.gov (NCT06366022).
Twenty-one patients (16 women and 5 men; mean age: 39.7 years) undergoing treatment for multiple gingival recessions with the modified coronally advanced tunnel technique (MCAT) were recruited from the Department of Periodontology and Oral Mucosa Diseases, Medical University of Warsaw (Poland) between May 2023 and July 2024. All participants provided written informed consent.
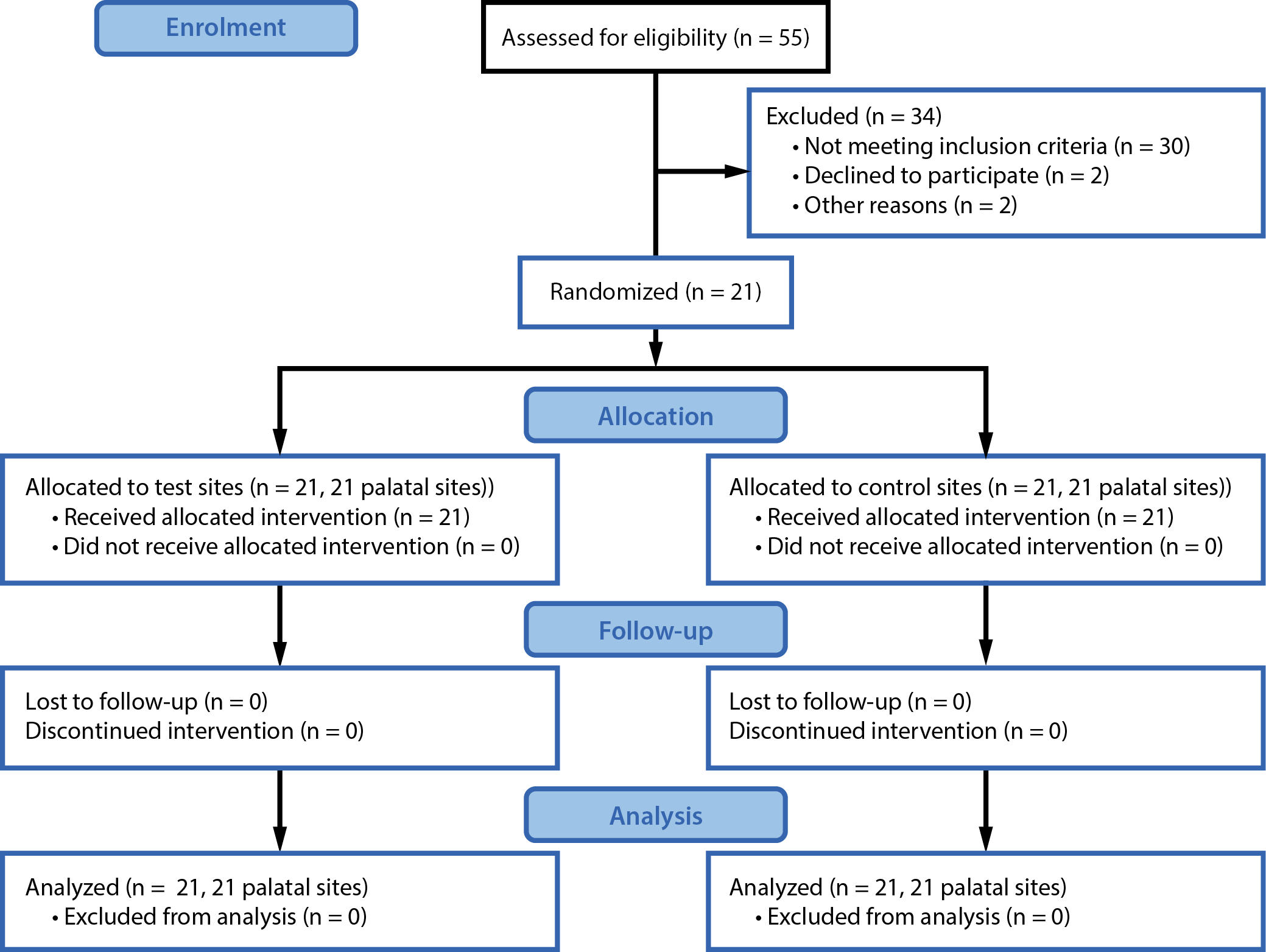
The study protocol was approved by the Bioethics Committee of the Medical University of Warsaw (approval No. KB/56/2023) and complied with the Declaration of Helsinki (1975, as revised in 2013). The study flowchart is shown in Figure 1.
Inclusion and exclusion criteria
Participants were eligible if they: 1) were aged 18–65 years; 2) had no history of periodontal surgery at the study sites; 3) had no systemic conditions that could impair wound healing; 4) were non-smokers; 5) were not pregnant or breastfeeding; and 6) had full-mouth bleeding on probing (FMBOP) and full-mouth plaque score (FMPS) below 15%.
The exclusion criteria were as follows: 1) systemic disorders (e.g., immunologic diseases, coagulation disorders, chemotherapy or radiotherapy, uncontrolled diabetes mellitus); and 2) a history of allergy to Manuka honey or gelatin sponge.
Study endpoints
The primary endpoint was patient-reported morbidity, including postoperative pain, burning sensation, discomfort, and dietary changes, assessed at 1, 2, 4, 7, and 14 days postoperatively using a visual analogue scale (VAS). Secondary outcomes included palatal wound healing at 14 days, assessed using the Landry Wound Healing Index (WHI)35 (Supplementary Fig. 1), and the occurrence of delayed bleeding (DB) at 14 days.
Sample size calculation
A power analysis was performed based on postoperative pain measured using a VAS as the primary outcome. Assuming an α level of 0.05 and a statistical power of 80%, the sample size was calculated to detect a difference of 8.92 percentage points between groups, with a common standard deviation (SD) of 7.39%, based on data from a registered clinical trial.36 On this basis, 11 patients per group were required.
Randomization and allocation concealment
Randomization was performed prior to surgery by an independent statistician not involved in patient treatment, using a computer-generated allocation list. Given the split-mouth design, each participant received both interventions: a Manuka honey dressing (test) and a gelatin sponge (control), applied to contralateral palatal donor sites during the same surgical session. Allocation concealment was maintained using sealed, opaque envelopes with coded labels; envelopes were opened immediately before graft placement. Participants were not informed of the treatment allocation.
Surgical procedures and intraoperative assessments
All participants received oral hygiene instructions (the roll technique with a soft toothbrush) and underwent professional prophylaxis and polishing before surgery. Patients with a FMPS and FMBOP below 20% were scheduled for surgery. All clinical measurements were recorded by a blinded examiner (N.M.C.) using a calibrated periodontal probe (UNC 15; Hu-Friedy, Chicago, USA). Examiner calibration was considered complete when at least 90% of measurements were reproducible and exact agreement was achieved for 75% of measurements.
All surgical procedures were performed by a single periodontist (B.G.) at the Medical University of Warsaw. Both sites (test and control) were treated during the same surgical session. Local anesthesia was administered in the palatal area using 4% articaine hydrochloride with 1:100,000 epinephrine (Ubistesin Forte 1.7 mL; 3M ESPE, Saint Paul, USA). A full-thickness flap was elevated to the mucogingival junction (MGJ) using a small periosteal elevator, followed by split-thickness dissection beyond the MGJ using tunneling instruments. Adjacent papillae were prepared to allow coronal advancement. Root planing was performed using Gracey curettes (Hu-Friedy).
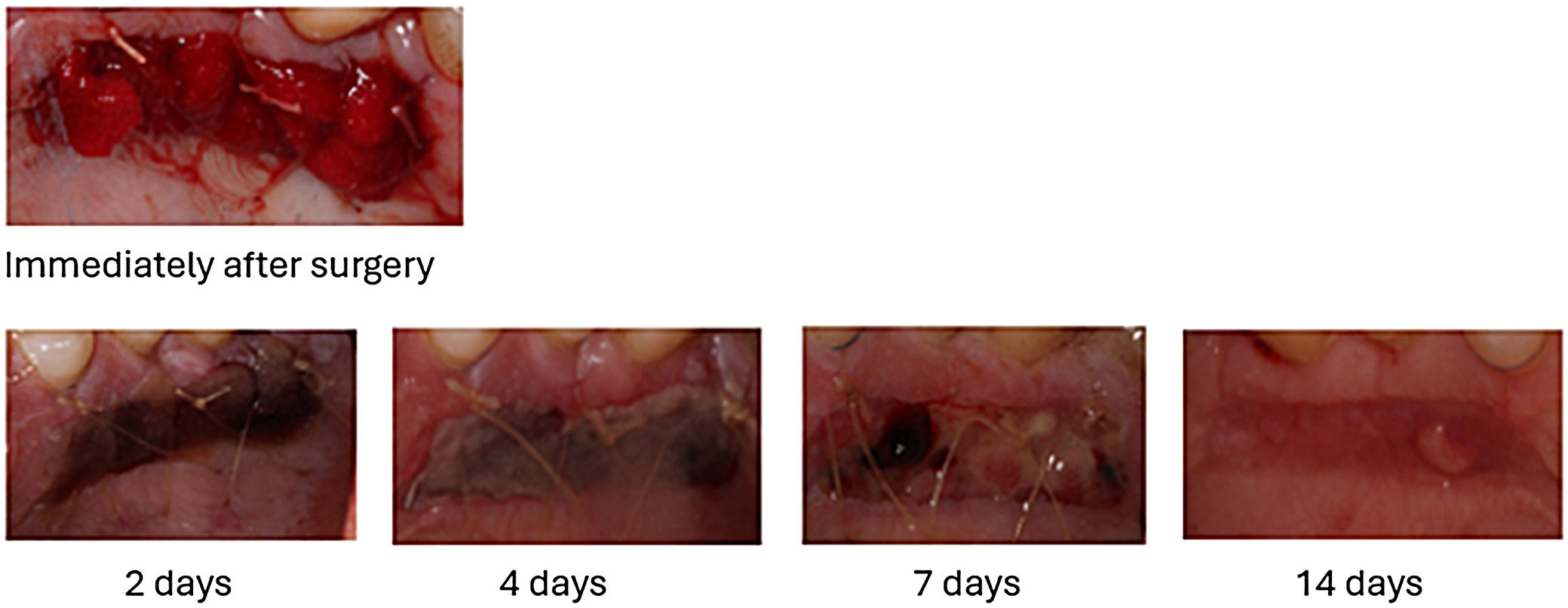
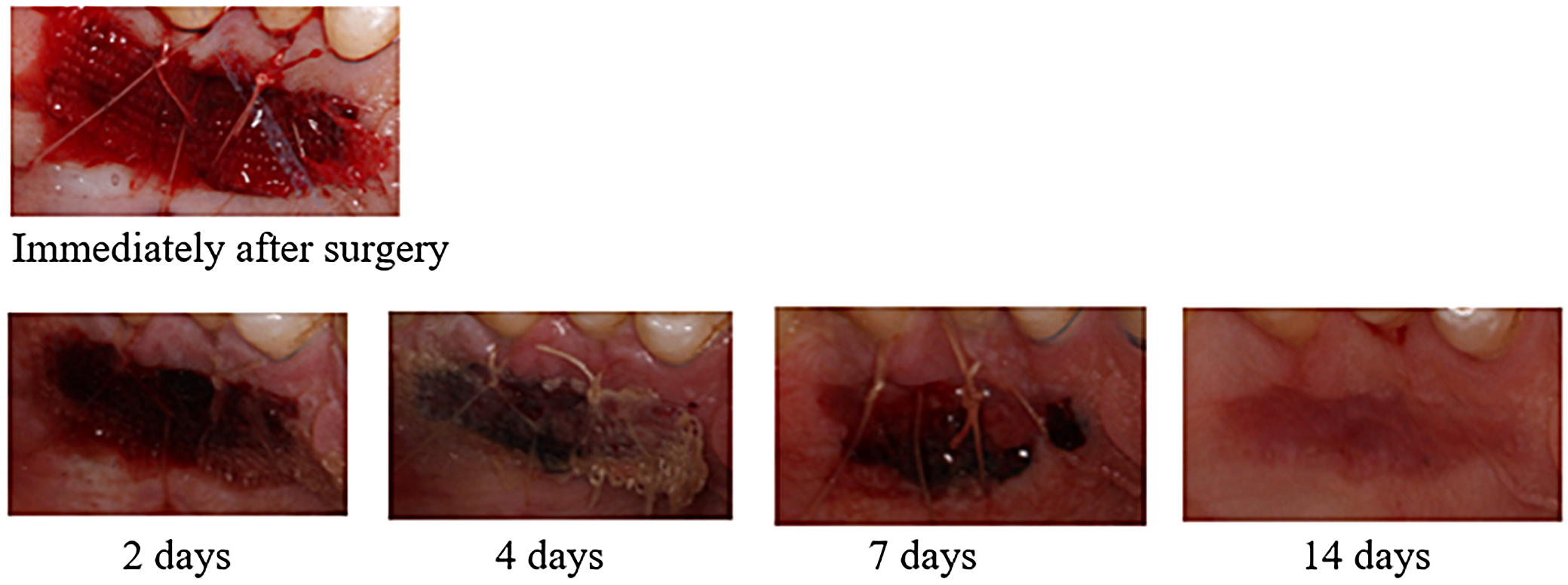
The FGG was harvested from the palatal premolar–molar region as an epithelialized graft, followed by extraoral de-epithelialization.37 The incision was made perpendicularly (90°) to the palatal surface, approx. 3 mm apically to the gingival margin of the maxillary teeth. As postoperative pain may be associated with graft dimensions, these were measured before de-epithelialization. After extraoral de-epithelialization, the connective tissue graft thickness was approx. 1 mm, with a width of about 4 mm; graft length corresponded to the prepared tunnel length. Graft thickness (GT), graft width (GW), and graft length (GL) were recorded in the mesiodistal and apicocoronal dimensions. After graft harvesting, the palatal donor sites were covered and stabilized with cross-mattress non-resorbable sutures (Seralon 4/0, 3/8; Serag-Wiessner GmbH & Co. KG, Naila, Germany). The control sites received an absorbable porcine gelatin sponge, whereas the test sites received the Manuka honey dressing, using the same suturing approach (Figure 2, Figure 3). At the recipient site, the graft was secured at the cemento-enamel junction level with resorbable sutures (PGA Resorba 6/0, 11 mm, 3/8; RESORBA Medical GmbH, Nuremberg, Germany). The flap and graft were stabilized with non-resorbable monofilament sutures (Seralon 6/0, 12 mm, 3/8; Serag-Wiessner GmbH & Co. KG). Both sides were treated with the same surgical technique.33
Postoperative care and morbidity assessment
At the end of surgery, all participants received 400 mg of ibuprofen and were instructed to take a 2nd dose 6 h later. Additional doses were permitted as needed for pain control. Written postoperative instructions included avoiding brushing, flossing, and chewing at the surgical sites for 2 weeks.
Participants were instructed to rinse twice daily with 0.12% chlorhexidine digluconate for the first 2 weeks. Sutures were removed after 14 days. Follow-up visits were scheduled at 1, 2, 4, 7, and 14 days postoperatively. Each visit included professional plaque removal and reinforcement of oral hygiene instructions, including the use of a postsurgical soft toothbrush with the roll technique for 3 weeks. Participants completed the morbidity questionnaires at each visit.
Postoperative outcome measures
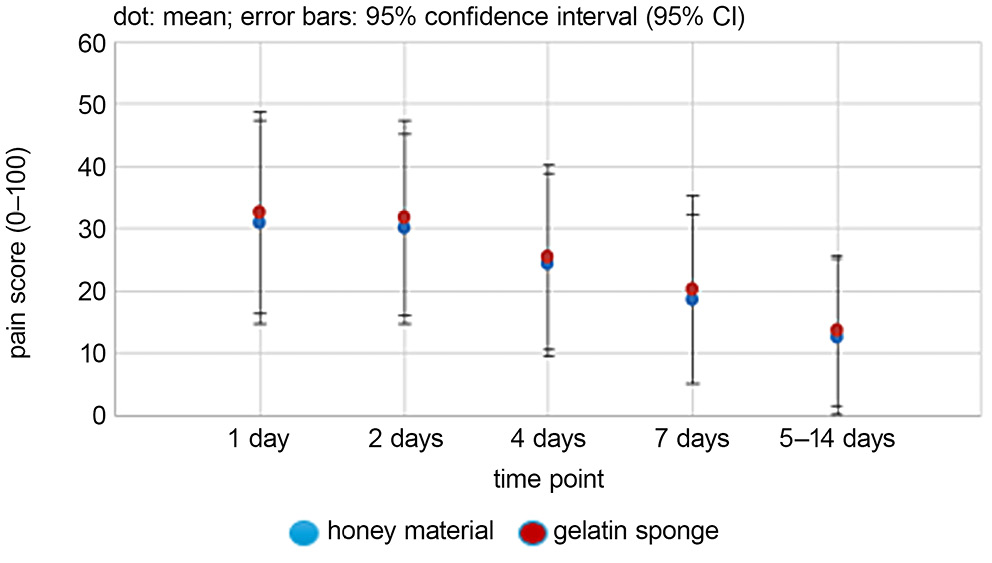
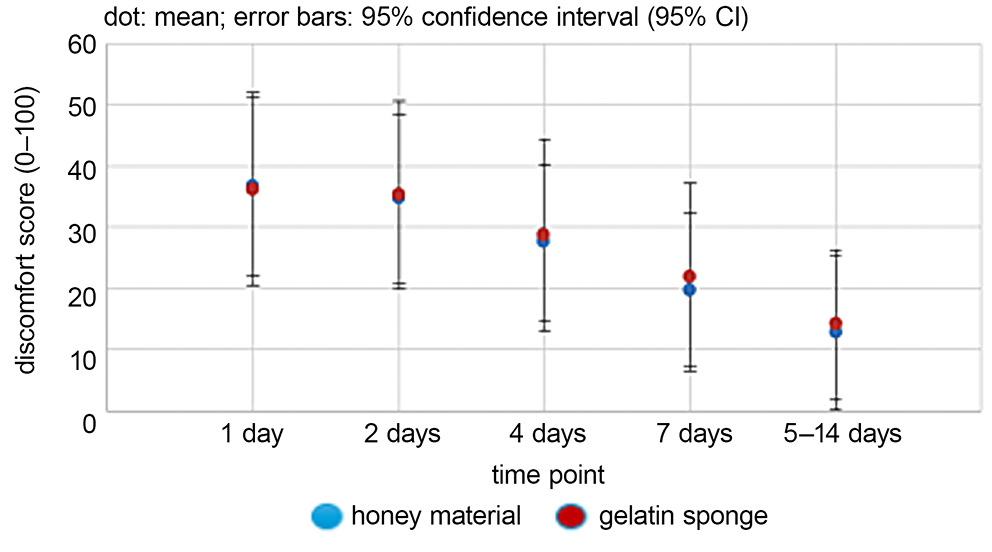
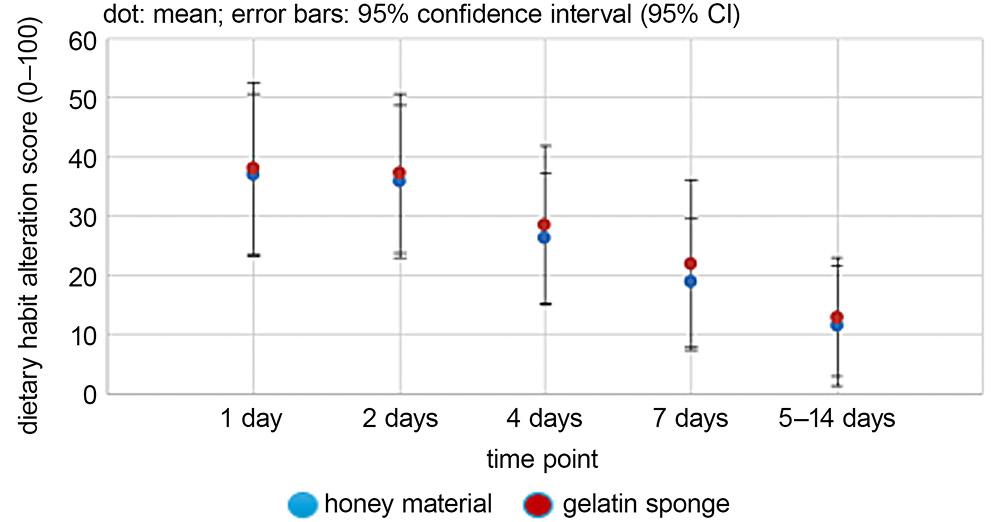
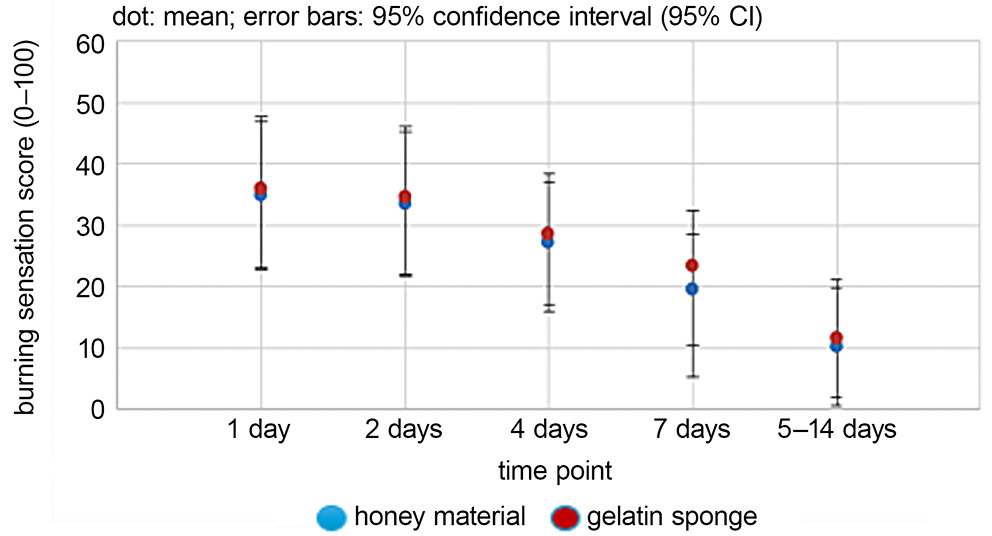
All postoperative assessments were performed by a blinded examiner (N.M.C.). Patient-reported outcomes, including discomfort, postoperative pain, burning sensation, and changes in dietary habits, were recorded at 1, 2, 4, 7, and 14 days postoperatively using a VAS (Figure 4).
− Discomfort: assessed after applying an air spray for 3 s to the palatal area (VAS categories: 0–4: no discomfort; 5–44: mild; 45–74: moderate; 75–100: extreme);
− Postoperative pain: self-reported pain at the palatal wound site (VAS categories: 0–4: no pain; 5–44: mild; 45–74: moderate; 75–100: severe);
− Burning sensation: perceived burning at the palatal wound (VAS categories: 0–4: absent; 5–44: mild; 45–74: moderate; 75–100: severe);
− Changes in dietary habits: difficulty chewing due to the palatal wound (VAS categories: 0–4: no change; 5–44: mild; 45–74: moderate; 75–100: extreme).
At 14 days postoperatively, palatal wound healing was evaluated using the Landry WHI.35 Delayed bleeding, defined as prolonged bleeding from the palatal wound, was assessed at 2 weeks and recorded as a binary outcome (yes/no).
Statistical analyses
Data are presented as means, SDs, frequencies, and percentages. Gender distribution was evaluated using a χ2 goodness-of-fit test. Differences in WHI categories and delayed bleeding were assessed using a χ2 test of independence; when expected cell counts were below 5, a Monte Carlo simulation approach (2,000 replicates) was used. Paired Student’s t-tests were applied to compare continuous outcomes between the honey dressing and gelatin sponge sites; normality was assessed using the Shapiro–Wilk test (n = 21 paired observations).
Visual analogue scale outcomes across time points were analyzed using repeated-measures analysis of variance (ANOVA), followed by multiple paired t-tests with Bonferroni correction. Assumptions were evaluated using the Shapiro–Wilk test (normality), Mauchly’s test (sphericity), and Levene’s test (homogeneity of variances). A two-sided α level of 0.05 was used. Analyses were performed using R v. 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Twenty-one patients with multiple, symmetrical gingival recession defects were enrolled: 15 women (71.4%) and 6 men (28.6%), with a mean age of 39.67 ±8.70 years. All participants completed the 2-week follow-up. No allergic reactions or clinically relevant complications were observed, and healing was uneventful. Baseline characteristics of the harvested grafts (GT, GW, and GH) were comparable between the honey dressing (test) and gelatin sponge (control) sites (paired Student’s t-test, all p > 0.05; Table 1). A statistically significant imbalance in sex distribution was observed (χ2 = 6.10, degrees of freedom (df) = 1, p = 0.014).
At 14 days, wound healing was rated as “very good” in 20 participants (95.2%) and “good” in 1 participant (4.8%) in both groups (Table 2). No delayed bleeding was reported. Visual analogue scale outcomes showed no statistically significant differences between treatments at any follow-up time point for postoperative pain, discomfort, burning sensation, or changes in dietary habits (Figure 5, Figure 6, Figure 7, Figure 8; repeated-measures ANOVA, all p > 0.05). Mean scores decreased over time in both groups. One participant reported higher pain scores during the 1st week, which decreased during the 2nd week.
Discussion
The palate is a well-established donor site for soft-tissue graft harvesting. Depending on the technique, the graft may be used as a SCTG after extraoral de-epithelialization or as a FGG. Following graft harvesting, palatal wounds typically heal by secondary intention within 2–4 weeks.3, 11, 15, 38 Postoperative pain at the palatal donor site is a common reason for reluctance to undergo periodontal plastic surgery.31, 35, 39 Consequently, many studies have evaluated topical agents and physical barriers intended to protect the donor site and reduce patient morbidity. Although honey has well-documented antibacterial properties, evidence regarding its direct effects on oral wound healing remains limited. To our knowledge, this is the first randomized controlled trial to compare a Manuka honey dressing with a gelatin sponge for the management of the palatal donor site after FGG harvesting.
In this split-mouth trial, the Manuka honey dressing did not significantly reduce postoperative pain, discomfort, burning sensation, or diet-related limitations compared with a gelatin sponge at 1–14 days postoperatively. These findings align with previous reports that donor-site morbidity is influenced by harvesting technique and wound protection.36 In a study comparing platelet-rich fibrin with a gelatin sponge for palatal wound management, Feminella et al. similarly reported comparable patient-reported outcomes between interventions.21 No participant reported delayed bleeding, and healing at 14 days was rated as good or very good in all cases. This is consistent with previous studies reporting low rates of postoperative complications after palatal SCTG harvesting.3
Medical-grade honey has been investigated in a variety of wound types, including surgical incisions,38 burns,39 and chronic ulcers such as diabetic foot ulcers.40 Its proposed mechanisms include moisture retention, reduced inflammation, and supporting tissue regeneration, which may create a favorable environment for healing.41 Based on the present findings, Manuka honey dressing appears to be a feasible alternative to a gelatin sponge for protecting palatal donor sites, but did not demonstrate superiority in short-term patient-reported outcomes or early clinical healing in this sample. Larger studies with longer follow-up are needed to confirm these findings and to determine whether specific patient subgroups may benefit.
Limitations of the study
One limitation of this study is the increased risk of type I error due to multiple statistical tests. Although the analyses were exploratory and no overall correction for multiple comparisons was applied, the results should be interpreted cautiously and confirmed in future studies.
Additional limitations include the use of a single honey product, which may limit the generalizability of the findings. Patient-related factors such as sex and age may influence pain perception and reported morbidity.37, 42, 43 In addition, because the donor and recipient sites are anatomically close, some participants may have had difficulty distinguishing the source of discomfort.
Finally, physical barriers have been suggested to provide superior protection of palatal wounds compared with some alternative approaches,15, 41 and the present study compared only a gelatin sponge and the honey dressing. Despite these limitations, the study followed CONSORT recommendations, included calibration and blinding of outcome assessment, and all surgeries were performed by an experienced clinician.
Conclusions
Within the limitations of this randomized controlled trial, a Manuka honey dressing and a gelatin sponge provided comparable early healing and patient-reported outcomes when used to manage palatal donor sites after FGG harvesting. Manuka honey dressing may be considered a natural alternative to conventional dressings for donor-site protection; however, it did not demonstrate clear clinical superiority in the early postoperative period.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.18335051. The package contains the following files:
Supplementary Table 1. Results of the normality and homogeneity of variance tests for GT, GW, and GH.
Supplementary Table 2. Results of the normality of the distribution, sphericity and homogeneity of variance.
Supplementary Table 3. Observed and expected frequencies for χ2 goodness-of-fit test.
Supplementary Fig. 1. Palatal wound healing at 14 days using the Landry WHI.
Data Availability Statement
The datasets supporting the current study’s findings are openly available at https://doi.org/10.5281/zenodo.18014753.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.