Abstract
Background. Sarcopenia, characterized by the loss of skeletal muscle mass, strength, and function, is a prevalent and severe complication of liver cirrhosis, irrespective of its etiology. Despite its early onset in cirrhosis, the impact of sarcopenia on liver transplantation (LT) outcomes is often underestimated.
Objectives. This study evaluates the role of both static and dynamic assessments of sarcopenia in LT recipients, focusing on cardiopulmonary performance and the likelihood of prolonged ICU stays.
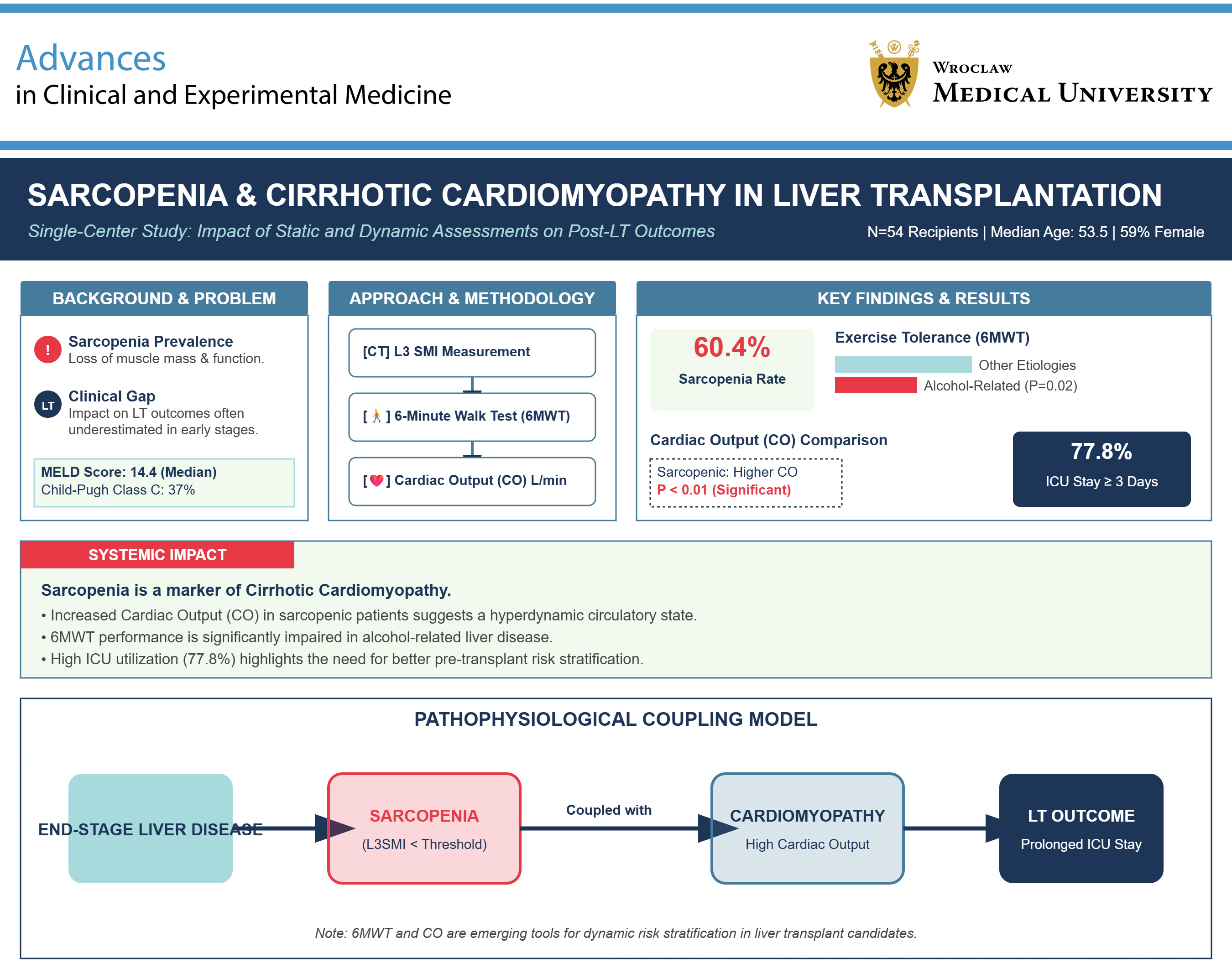
Materials and methods. We studied 54 LT recipients (median age: 53.5 years, 59% female patients) at a single center. The L3 skeletal muscle index (L3SMI) was measured using computed tomography (CT) scans, while exercise tolerance was evaluated with the 6-minute walk test (6MWT). Cardiac output (CO) was recorded in liters per minute.
Results. The median Model for End-Stage Liver Disease (MELD) score was 14.4, with 37% of patients classified as Child–Pugh class C. Major LT indications included autoimmune liver diseases (46.3%) and alcohol-related liver disease (ALD; 31.5%). Sarcopenia was present in 60.4% of patients. No significant differences in L3SMI were found related to underlying liver disease, gender, body mass index (BMI), or ammonia levels. However, patients with ALD covered significantly shorter distances in the 6MWT (p = 0.02). Sarcopenic patients had significantly higher CO than non-sarcopenic patients (p < 0.01). Intensive care unit (ICU) stay ≥3 days was observed in 77.8% of recipients, with no clear risk factors identified.
Conclusions. Sarcopenia linked to end-stage liver disease (ESLD) correlates with cirrhotic cardiomyopathy, as evidenced by increased CO. Further studies are required to clarify the role of 6MWT and CO in post-LT risk stratification.
Key words: liver transplantation, cardiopulmonary exercise test, sarcopenia, cardiac output, 6-minute walk test
Background
Sarcopenia is a widely recognized, highly prevalent, and life-threatening complication in patients with liver cirrhosis, regardless of the disease’s etiology. It is defined by a combination of generalized loss of skeletal muscle mass, strength, and function,1 and it tends to develop earlier and more rapidly in liver cirrhosis compared with other chronic conditions. Alongside physical inactivity and frailty, sarcopenia is an independent predictor of morbidity and mortality in cirrhotic patients. Factors such as aging, malnutrition, decreased hepatic protein synthesis, catabolism, hyperammonemia, elevated pro-inflammatory cytokines, and low testosterone levels contribute to both cardiac and skeletal muscle deconditioning. This leads to diminished cardiac function and reserve, resulting in physical frailty and a reduction in skeletal muscle mass and strength.2 As such, sarcopenia can be an indicator of poor general health when predicting outcomes in patients undergoing general surgery3 and renal transplantation.4 Male sex and liver function decompensation, as indicated by Child–Pugh class C cirrhosis, have been identified as independent predictors of sarcopenia, which in turn is an independent predictor of mortality.5 Among liver transplant (LT) candidates, sarcopenia is linked to increased waitlist mortality5, 6, 7, 8 and sepsis-related deaths while on the waitlist.8 Furthermore, sarcopenia tends to progress during the transplantation process and can persist up to 1 year post-surgery.9 A recent meta-analysis highlighted the negative impact of sarcopenia on LT outcomes.10 Post-transplant complications associated with sarcopenia include extended hospital and intensive care unit (ICU) stays, a higher risk of infections,11 and increased mortality following transplantation.12, 13, 14, 15, 16, 17
Computed tomography has been established as the gold standard for identifying low muscle mass, as recognized by the European Working Group on Sarcopenia in Older People, using measurements at the L3 vertebral level. However, the same Working Group also recommends dynamic evaluations of muscle function, which may provide a more objective assessment of tissue aging and natural remodeling. Recent data suggest that sarcopenia may impact the left heart chamber, contributing to occult heart failure with preserved ejection fraction under baseline conditions,18 as well as leading to respiratory muscle and diaphragmatic sarcopenia and associated weakness.19, 20
While outcomes following LT are influenced by recipient, donor, and procedural factors, the scarcity of donor livers necessitates optimizing the life-saving potential of procured livers, particularly in older candidates with more advanced end-stage liver disease (ESLD) and additional comorbidities (e.g., metabolic syndrome). Moreover, cardiovascular events are a significant contributor to serious complications and non-liver-related deaths after LT.21 Pre-transplant cardiovascular assessments aim to detect severe cardiopulmonary diseases that could render LT futile. Typically, cardiological evaluations focus on ischemic heart disease and its complications. However, there is a noticeable lack of routine dynamic assessments of cardiopulmonary performance in ESLD candidates under conditions of increased oxygen demand or hemodynamic instability.
Exercise intolerance is widely regarded as an indicator of reduced functional capacity and disability. In ESLD, there is a complex interplay of factors such as malnutrition, sarcopenia, and frailty.22 The 6-minute walk test (6MWT) is commonly employed to assess exercise capacity. It is an inexpensive, well-tolerated, noninvasive test that correlates with daily activity levels. Numerous studies have shown that 6MWT results correlate with the Model for End-Stage Liver Disease (MELD) and Child–Pugh scores as well as with mortality rates.23, 24 The 6MWT assesses overall exercise capacity and may correlate with maximal oxygen consumption (VO2), predicting survival in cirrhotic patients and the risk of death while on the LT waiting list.24 Poor performance during the 6MWT indicates abnormal exercise capacity in cirrhotic patients, with shorter distances covered correlating with more severe liver disease as assessed with the Child–Pugh score24 and with short-term survival.25 A peak oxygen uptake (VO2 peak) below 60% of the predicted value has been identified as a prognostic factor for 100-day LT-related mortality.26
Conversely, liver cirrhosis is associated with increased resting cardiac output (CO), decreased systemic vascular resistance, systolic incompetence under stress, diastolic dysfunction, increased left ventricular thickness, and electrocardiography (ECG) abnormalities, collectively referred to as hyperdynamic circulation and cirrhotic cardiomyopathy.27, 28 The increase in CO is linearly related to the progression of portal hypertension.29 Notably, elevated CO is disproportionate to oxygen consumption, indicating a decreased arteriovenous oxygen difference.30
To date, the influence of sarcopenia on cardiopulmonary efficiency before LT and on subsequent morbidity and mortality after LT, particularly in terms of prioritizing patients by transplant survival benefit, has not been thoroughly investigated. However, it is rational to prioritize patients to avoid short-term futility, defined as post-transplant 3-month mortality, and to ensure long-term survival exceeding 50% at 5 years post-LT.
Objectives
This study evaluates the role of both static (Skeletal Muscle Index at the 3rd lumbar vertebra (L3SMI)) and dynamic (6MWT) assessments of sarcopenia in LT recipients, focusing on cardiopulmonary performance, body composition differences across liver disease etiologies, and their impact on the likelihood of prolonged ICU stays. Additionally, this study aims to assess the relationship between sarcopenia, functional performance, and body composition, highlighting the significance of 6MWT as a functional marker and the influence of liver disease etiology on body mass index (BMI) and muscle mass.
Materials and methods
Participants
The study group consisted of 54 well-characterized liver graft recipients (22 men and 32 women), with a median age of 53.5 years. The liver disease etiology included alcohol-related liver disease (ALD; 31.5% of patients), autoimmune liver diseases (46.3%), viral hepatitis (13%), and other causes (9%). The median MELD score for the entire cohort was 14.4 points, with 37% of patients classified as Child–Pugh class C. Median BMI was 23.95 kg/m2 for women and 27.65 kg/m2 for male patients. L3SMI was measured using computed tomography (CT) scans, with a median value of 46.1 cm2/m2 for women and 44.55 cm2/m2 for men. The 6MWT was performed indoors along a flat, straight, 30-m corridor, with the median distance covered being 431 m. Cardiac output was measured using a noninvasive CNAP device during the 6MWT. Intensive care unit stay duration was recorded, with 77.8% of recipients staying more than 3 days in ICU and 9.5% staying more than 6 days. Two patients died within 1 year after transplantation. The characteristics of the study group are summarized in Table 1.
The study did not require an informed consent form to be signed. All the described tests are routinely performed in LT candidates. The scheme of data gathering and evaluation is presented in Figure 1.
Definition of sarcopenia
Computed tomography scanning at the L3 vertebral level has been validated as the gold standard for recognizing low muscle mass, according to the European Working Group on Sarcopenia in Older People.1 Following the method proposed by Carey et al.,31 the cross-sectional area of muscles at L3 was measured and normalized to the individual’s height, resulting in the skeletal muscle index (L3SMI). Cutoff values of 50 cm2/m2 for men and 39 cm2/m2 for women were used to define sarcopenia.31 Although the L3SMI score was used to define sarcopenia, we acknowledge that current consensus definitions recommend incorporating both low muscle mass and reduced muscle strength or physical performance. In our cohort, direct measures of muscle strength, such as handgrip dynamometry, were not available due to logistical constraints. However, we employed the 6MWT as a surrogate marker of functional capacity (see below).
6-minute walk test and hemodynamic measurements
The 6MWT was conducted according to guidelines provided by the Polish Respiratory Society,32 under the supervision of a qualified physician. The test was performed indoors, on a flat, straight, 30-m-long corridor with a hard surface and free of any type of obstacles. Patients were instructed to walk as fast as possible for 6 min, with the distance covered recorded at the end. Cardiac output was continuously measured during the test using a continuous noninvasive arterial pressure (CNAP) device for noninvasive, continuous measurement of hemodynamic parameters (CNSystems Medizintechnik AG, Graz, Austria) during the 6MWT.
Statistical analyses
Statistical analyses were performed using IBM SPSS v. 26.0 (IBM Corp., Armonk, USA), GraphPad Prism v. 8.0 (GraphPad Software, San Diego, USA), and Python (StatsModels package) for logistic regression modeling. A two-sided p-value of less than 0.05 was considered statistically significant.
The distribution of continuous variables was assessed using the Shapiro–Wilk test. Variables with normal distribution were compared between 2 groups using the Student’s t-test. For non-normally distributed variables, the Mann–Whitney U test was applied. Comparisons involving more than 2 groups were conducted using the Kruskal–Wallis test. Homogeneity of variances was evaluated with Levene’s test, and results are presented in Supplementary Table 1.
Correlations between continuous variables were assessed using Spearman’s rank correlation coefficient. Univariate logistic regression was used to evaluate associations between clinical and functional parameters and prolonged ICU stay (>3 days and >6 days). Results are reported as odds ratios (OR) with 95% confidence intervals (95% CIs), p-values, and model performance indices. Model fit was assessed using the Nagelkerke R2 statistic, which is reported in Table 2, Table 3.
To verify the assumption of linearity between continuous predictors and the logit of the binary outcome in logistic regression, the Box–Tidwell test was employed. This method introduces interaction terms between each predictor and its natural logarithm. Nonsignificant interaction terms (p > 0.33 for all tested variables) confirmed that the linearity assumption was met for all continuous predictors included in the model.
Results
A total of 54 patients undergoing LT were included in the study. Of these, 32 (60.4%) met the criteria for sarcopenia based on L3SMI thresholds. Sarcopenia was more common among male recipients, with 26 out of 32 male patients (81.3%) classified as sarcopenic (L3SMI < 50 cm2/m2), compared to 6 out of 22 women (27.3%) with L3SMI < 39 cm2/m2. The lowest recorded L3SMI in the male group was 24.8 cm2/m2 (Table 1).
No statistically significant associations were found between sarcopenia and age (≤50 vs >50 years, p = 0.95), gender (p = 0.62), BMI (p = 0.16), liver disease etiology (p = 0.84), ammonia levels (p = 0.69), or liver function as measured using the MELD score (p = 0.73). Similar patterns were observed for 6MWT performance and CO. Detailed comparisons are presented in Table 4.
Etiology-specific analysis revealed significant differences in BMI (p = 0.004, Kruskal–Wallis test). Post hoc Bonferroni-adjusted Mann–Whitney U tests showed that ALD patients had significantly higher BMI compared to autoimmune (p = 0.007) and viral (p = 0.004) subgroups. Median BMI was 27.1 kg/m2 (ALD), 21.75 kg/m2 (autoimmune), and 22.58 kg/m2 (viral). The MELD scores were numerically highest among viral hepatitis patients (median: 19.5), but this did not reach statistical significance (p = 0.07).
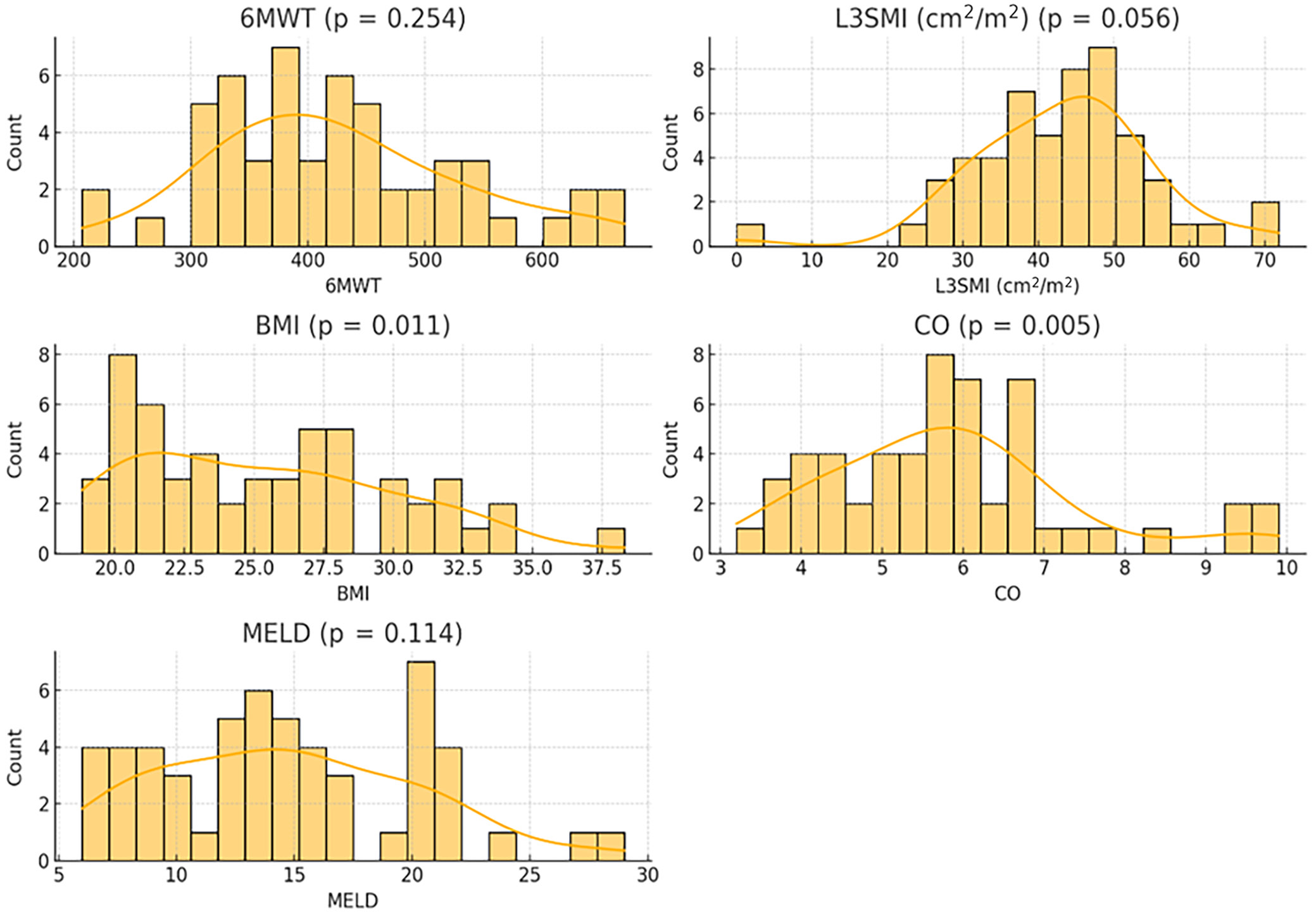
No significant differences in L3SMI (p = 0.84) or CO (p = 0.29) were observed across liver disease etiologies. The 6MWT performance was lowest in ALD patients (median: 375.0 m), and highest in other etiologies (up to 467.5 m), with borderline significance (p = 0.06). As shown in Figure 2, histograms with kernel density estimates were used to assess the distribution of continuous variables. This evaluation informed the selection of appropriate statistical methods (parametric vs nonparametric) for further analyses. Levene’s test results for homogeneity of variance are provided in Supplementary Table 1.
Table 5 summarizes descriptive statistics for clinical and functional measures. Spearman correlations between parameters are presented in Table 6. L3SMI was significantly associated with BMI (p < 0.05), and 6MWT correlated positively with both L3SMI and CO (p < 0.01).
Univariate logistic regression models evaluating risk factors for ICU stay >3 days are summarized in Table 2. None of the predictors reached statistical significance. However, for ICU stay >6 days (Table 6), lower values of 6MWT (p = 0.025), L3SMI (p = 0.048), BMI (p = 0.046), and CO (p = 0.003), as well as higher MELD scores (p = 0.048), were associated with prolonged ICU stay. Nagelkerke R2 values ranged from 0.005 to 0.157.
To formally assess the assumption of linearity between continuous predictors and the logit of the binary outcome (prolonged ICU stay >6 days), the Box–Tidwell test was conducted for the following variables: age, L3SMI, total cross-sectional muscle area at L3, and 6MWT distance. Each predictor was tested by including an interaction term between the variable and its natural logarithm in a logistic regression model.
None of the interaction terms reached statistical significance (all p > 0.33), indicating that the assumption of linearity was met for all included continuous variables. Specifically, p-values for the interaction terms were as follows: age (p = 0.359), L3SMI (p = 0.333), total muscle area (p = 0.351), and 6MWT (p = 0.351). These results confirm that the logit-linear relationship required for logistic regression holds in this dataset.
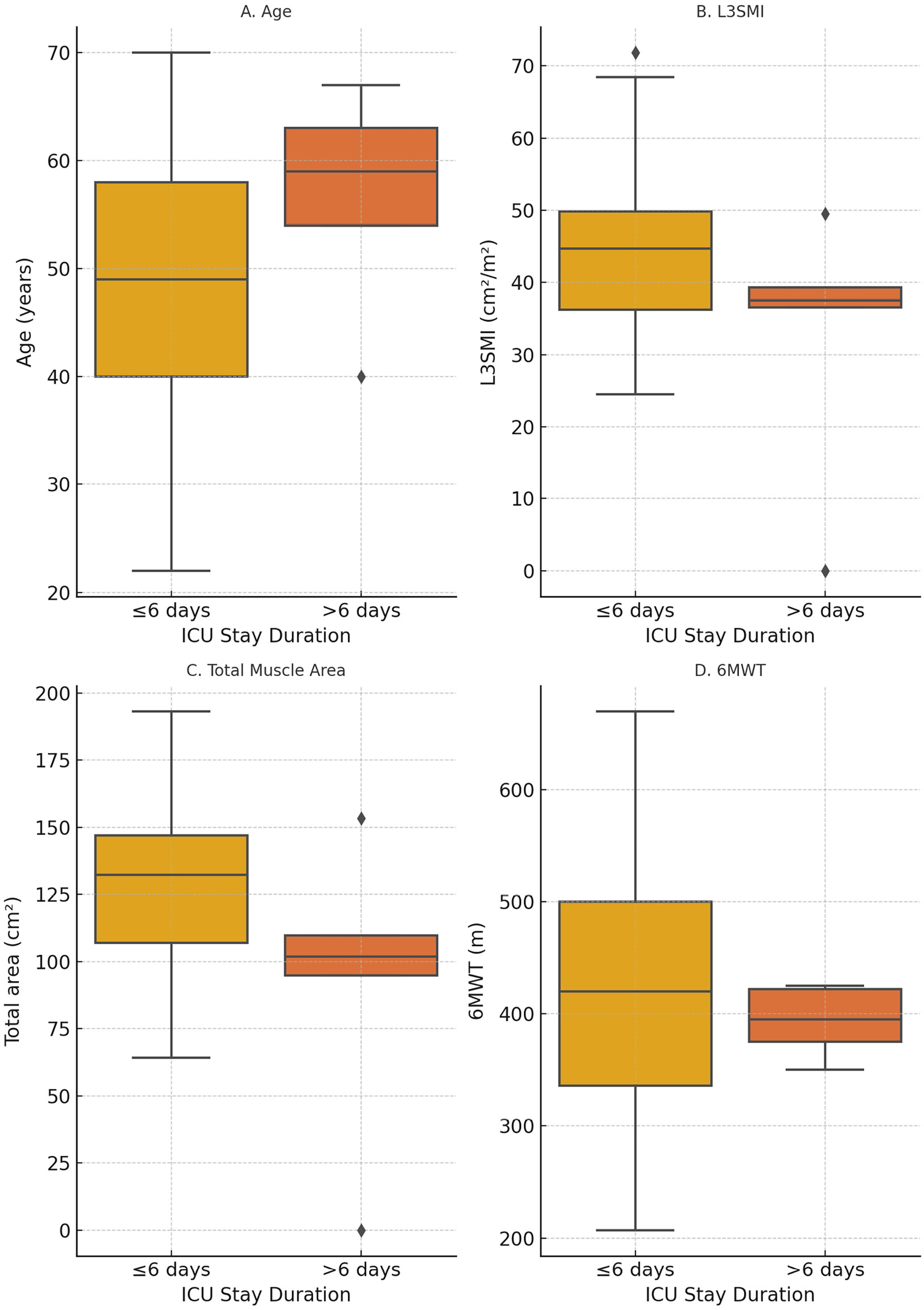
Figure 3 presents boxplots of continuous clinical predictors stratified by ICU stay duration (≤6 days vs >6 days), with individual data points overlaid to illustrate intergroup variability. This visual representation complements the Box–Tidwell test results and provides an intuitive summary of the association between predictor variables and ICU outcome. Notably, patients with ICU stays longer than 6 days exhibited lower values of L3SMI, 6MWT distance, and CO, supporting the hypothesis that reduced muscle mass and impaired functional capacity may contribute to prolonged postoperative recovery.
Discussion
Current cardiological assessment protocols for LT candidates primarily focus on detecting coronary artery disease and its associated complications. However, these protocols often fall short in evaluating patients who cannot undergo cardiopulmonary exercise testing, particularly in the context of cirrhosis-related hemodynamic disturbances. Changes in lean muscle mass are closely linked to the pathophysiology of cardiovascular disease, perpetuating a cycle of functional decline.33 This highlights a significant gap in assessing cardiac function during surgery, especially under conditions of increased oxygen demand and hemodynamic instability in LT recipients.
This study aimed to compare static (L3SMI) and dynamic (6MWT) sarcopenia assessments in LT recipients, while also evaluating CO as a potential indicator of cardiovascular fitness. Our prior research identified sarcopenia as a potential risk factor for prolonged ICU stays in LT candidates.34 However, the current findings suggest that L3SMI alone does not adequately predict liver function, morbidity, or mortality post-transplantation. No significant correlation was observed between L3SMI-defined sarcopenia and liver disease etiology, BMI, ammonia levels, or functional capacity as measured with the 6MWT. This suggests that sarcopenia is highly prevalent among LT recipients, particularly men, but may not serve as a standalone risk marker for postoperative outcomes.
The visual comparison presented in Figure 3 illustrates that patients with reduced 6MWT distances, lower L3SMI values, and diminished CO were more likely to experience prolonged ICU stays. Although no single variable independently predicted ICU duration, this consistent pattern suggests a multifactorial interplay between impaired muscular status, limited functional reserve, and reduced cardiovascular adaptability. Prolonged ICU stay is a clinically meaningful postoperative outcome, often associated with increased morbidity, resource utilization, and delayed recovery. These findings reinforce the importance of incorporating dynamic functional assessments into preoperative risk stratification, particularly in the context of post-transplant recovery, rather than relying solely on static anatomical metrics. Similar conclusions have been drawn in other transplant and surgical populations. For example, Singer et al. demonstrated that physical frailty phenotypes were strongly predictive of mortality after lung transplantation, highlighting the prognostic value of functional status.35 In a broader perioperative context, Gillis et al. emphasized the role of prehabilitation in improving surgical outcomes and reducing postoperative complications.36 In LT specifically, reduced 6MWT performance has been associated with mortality and adverse outcomes,24 and physical frailty has been linked to prolonged ICU and hospital stays.37 These data support integrating functional capacity testing, such as the 6MWT, into standard pretransplant evaluation protocols.
A novel aspect of this study was the analysis of BMI variations across different liver disease etiologies. Alcohol-related liver disease patients exhibited significantly higher BMI values compared to autoimmune and viral liver disease groups (p = 0.004), yet they also demonstrated the poorest 6MWT performance. This aligns with prior research indicating that ALD is often associated with sarcopenic obesity, a condition characterized by higher fat deposition despite significant muscle wasting. In contrast, patients with autoimmune and viral liver diseases tended to have lower BMI values, potentially reflecting chronic inflammation, malabsorption, or metabolic deficiencies. These findings reinforce the need for individualized nutritional and metabolic assessments in LT candidates, as BMI alone does not fully capture muscle function or frailty risk.
From a pathophysiological perspective, advanced cirrhosis leads to compensatory cardiovascular adaptations, including a reduction in effective circulating blood volume, splanchnic vasodilation, and hyperdynamic circulation. This can manifest as increased resting CO and, in some cases, the development of cirrhotic cardiomyopathy (CCM). Typically, CCM remains subclinical, as compensatory mechanisms maintain myocardial function despite reduced preload and afterload. However, when exposed to stressors such as exercise or surgical interventions, patients with cirrhosis may exhibit impaired cardiovascular responses due to an inadequate increase in CO during exertion.38, 39 Despite this well-documented phenomenon, our findings did not reveal a significant association between sarcopenia status and CO. At the same time, CO was significantly associated with age, sex, and BMI, and positively correlated with L3SMI, indicating that its determinants may be multifactorial.
In healthy individuals, CO is expected to rise during exercise, driven by an increase in stroke volume and heart rate. However, in cirrhotic patients, dysautonomia, neurohormonal imbalances, and structural myocardial changes may blunt this response, leading to an inability to meet the metabolic demands of exercise.40, 41, 42 This may partially explain why ALD patients, despite having a higher BMI, exhibited the poorest 6MWT results. Notably, patients with ALD covered significantly shorter distances than other etiological groups (p = 0.02), reinforcing the role of functional capacity assessments in this population.
While prolonged ICU stays in sarcopenic individuals have been linked to reduced respiratory efficiency and muscle dysfunction,43 the present study did not identify specific predictors of postoperative ICU length of stay. Recent research suggests that sarcopenia may be associated with cardiac dysfunction, including left ventricular impairment and heart failure with preserved ejection fraction, even under baseline conditions.18 Additionally, respiratory muscle weakness and diaphragmatic dysfunction may exacerbate frailty and functional decline in cirrhotic patients.19, 20 A related condition, cardiac cachexia, has also been described in LT candidates, characterized by chronic inflammation, endotoxemia, and proteolytic activation, which accelerate muscle depletion and metabolic inefficiency.43 This process is exacerbated by hyperammonemia, proteasomal overactivation, mitochondrial dysfunction, and increased oxidative stress, all of which contribute to skeletal muscle atrophy and exercise intolerance.44, 45
Despite prior evidence suggesting an interplay between ammonia levels, sarcopenia, and cardiovascular dysfunction, this study did not find a direct correlation between ammonia and CO, 6MWT performance, or prolonged ICU stay. Additionally, L3SMI did not correlate with muscle function or transplant outcomes, reinforcing the limitations of static muscle assessments in cirrhotic patients. Notably, ALD patients had the lowest 6MWT results (median: 380 m), aligning closely with the mortality threshold of 387 m identified by Pimentel et al.24 These findings underscore the clinical significance of exercise prehabilitation programs, which may improve functional capacity and post-transplant recovery.
Given that 6MWT performance provided more relevant functional insights than L3SMI, our findings suggest that functional rather than static muscle assessments may be more valuable in LT candidates. The lack of correlation between L3SMI and post-transplant outcomes raises important questions about whether alternative markers of sarcopenia, such as direct muscle strength measurements, should be prioritized in future studies. Moreover, BMI variations among liver disease etiologies suggest that body composition, rather than weight alone, may play a critical role in sarcopenia risk stratification. Future research should explore comprehensive body composition analyses, functional testing protocols, and prehabilitation interventions to optimize transplant candidate selection and postoperative outcomes.
Limitations of the study
A major limitation of this study is the relatively small sample size, which may reduce statistical power and limit the generalizability of the findings. However, the cohort reflects a real-world population undergoing a complex and infrequently performed procedure at a single tertiary center, which inherently limits recruitment capacity. Despite this, the prospective design, in-depth patient characterization, and combined functional and morphological assessment of sarcopenia provide meaningful preliminary insights and emphasize the need for future multicenter validation.
A key limitation of our study is the lack of detailed data on comorbidities such as cardiovascular disease, diabetes, and other metabolic disorders. In addition, renal function markers and hemoglobin levels were not included in the analysis, despite their potential influence on exercise tolerance and 6MWT performance. However, it is important to note that sarcopenia in the context of liver cirrhosis often develops earlier and progresses more rapidly than in other chronic conditions such as heart or lung diseases, particularly in subgroups such as those with ALD. In this population, sarcopenia is primarily driven by liver dysfunction itself, which may partially mitigate the impact of unmeasured comorbidities. Moreover, all patients in our cohort were functionally independent and able to complete the 6MWT, suggesting a relatively preserved baseline physical capacity across the group.
Although ammonia levels were evaluated, no significant associations were found with muscle strength, 6MWT results, or ICU length of stay. This may indicate that functional consequences of hyperammonemia-induced sarcopenia develop over longer timeframes, or that other mechanisms, such as chronic inflammation or neurohormonal dysregulation, play a more prominent role in sarcopenia related to liver cirrhosis.
Furthermore, the study did not identify clear predictors of prolonged ICU stay or early post-transplant complications, especially in relation to CO and pulmonary function. The elevated CO observed in sarcopenic patients raises important questions: Is this a compensatory response, a marker of advanced liver dysfunction, or an indication of cirrhotic cardiomyopathy? The current data are insufficient to resolve this issue and underscore the complex interplay between hepatic, muscular, and cardiovascular systems in this population.
Lastly, the lack of standardized pre-transplant functional evaluations remains a broader challenge in transplant candidate assessment. The significant differences in 6MWT performance between etiological subgroups, particularly the lower performance in ALD patients, highlight the potential value of incorporating objective cardiopulmonary fitness measures into routine transplant evaluations. Future research should prioritize multicenter, prospective studies with larger sample sizes and a broader clinical scope, including comorbidities, renal function, and inflammatory markers, to enhance risk stratification and improve outcomes in LT.
Conclusions
Our findings confirm that severe chronic liver insufficiency accompanied by sarcopenia is associated with cirrhotic cardiomyopathy, as evidenced by increased CO. However, rather than a simple linear relationship, these results suggest a complex, multifactorial interplay between sarcopenia, functional capacity, and hemodynamic adaptation in cirrhosis.
Importantly, ALD patients exhibited the lowest 6MWT performance despite having higher BMI, reinforcing the need for body composition analysis beyond traditional anthropometric measures. The lack of a significant correlation between L3SMI and transplant outcomes raises questions about whether static muscle mass assessment alone is sufficient for risk stratification in LT candidates. Instead, dynamic functional tests such as the 6MWT may provide more clinically relevant insights.
Further large-scale, multicenter studies are warranted to determine the precise impact of sarcopenia on cardiopulmonary performance in LT candidates, as well as to evaluate the role of early exercise prehabilitation programs in improving functional outcomes, reducing post-transplant complications, and optimizing long-term survival.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.17494303. The package contains the following files:
Supplementary Table 1. Results of Levene’s test for homogeneity of variances for key continuous variables.
Data Availability Statement
The datasets supporting the findings of the current study are openly available in Zenodo at https://doi.org/10.5281/zenodo.13851662.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.