Abstract
Background. Knee osteoarthritis (KOA) is a common condition characterized by pain, stiffness, and reduced function, significantly impacting quality of life.
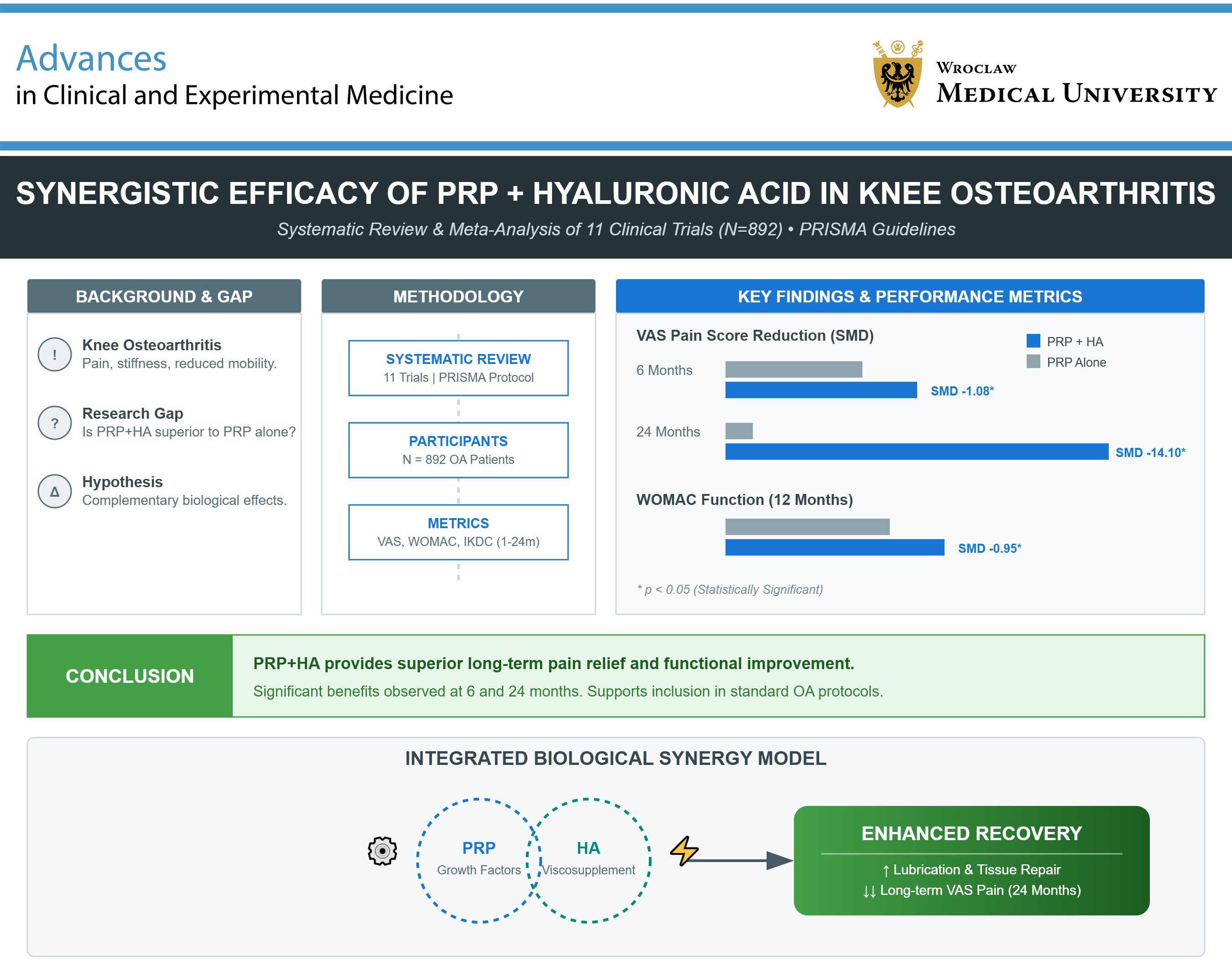
Objectives. This study aimed to evaluate the combined use of platelet-rich plasma (PRP) and hyaluronic acid (HA) compared to PRP alone in treating KOA. The hypothesis was that PRP + HA would provide superior outcomes in pain relief and functional improvement due to their complementary biological effects.
Materials and methods. A systematic review and meta-analysis were conducted according to PRISMA guidelines. The analysis included 11 trials with a total of 892 participants. The studies compared the efficacy of PRP + HA compared to PRP alone. Key outcomes evaluated were changes in the visual analogue scale (VAS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Inter-national Knee Documentation Committee (IKDC) scores at 1, 3, 6, 12, and 24 months post-treatment.
Results. At baseline, no significant differences in VAS scores were observed between the 2 groups (5.82 ±2.71 for PRP + HA vs 5.66 ±2.96 for PRP). By the 6-month follow-up, PRP + HA showed a more substantial reduction in VAS scores (−2.83 ±1.60 vs −2.56 ±1.66; standardized mean difference (SMD) = −1.08, 95% confidence interval (95% CI): −2.22 to 0.05; p < 0.001), with the largest improvement seen at 24 months (−2.7 ±0.2 for PRP + HA vs 0.4 ±0.23 for PRP; SMD = −14.10, 95% CI: −17.41 to −10.79; p < 0.001). WOMAC scores at 12 months also favored the PRP + HA group (−25.26 ±15.24 vs −19.6 ±14.20; SMD = −0.95; p = 0.01). IKDC scores showed no significant differences between groups.
Conclusions. The combination of PRP and HA provides superior pain relief and functional improvement compared to PRP alone, particularly at 6 and 24 months. These findings support the inclusion of PRP + HA in KOA treatment protocols and warrant further investigation into its long-term benefits.
Key words: meta-analysis, knee, hyaluronic acid (HA), platelet-rich plasma (PRP), knee osteoarthritis (KOA)
Introduction
Osteoarthritis (OA) of the knee joint (KOA) is one of the most common causes of impaired joint function and reduced quality of life in older adults; it is 4 times more common in women than in men.1, 2, 3 As people age and the prevalence of overweight increases, joints are subjected to greater stress. This, along with ongoing biomechanical and biochemical processes, leads to damage of the joint cartilage and subchondral bone in a manner that cannot be reversed. Other risk factors for OA include anatomical factors, obesity, and a previous history of trauma. This condition negatively impacts quality of life, contributing to poor overall health.1, 4, 5
To help relieve the symptoms of OA, patients suffering from joint pain, swelling, stiffness, and a decline in mobility, resulting in partial disability and requiring assistance with daily activities, need medications. These are difficult to formulate, as in addition to managing pain, slowing disease progression and improving knee function are the main goals.1, 5, 6, 7 Treatment options include surgical and non-surgical interventions. Non-surgical treatment is recommended for patients with early stages of KOA (Kellgren–Lawrence (KL) grade I–III), while surgery is performed in patients with advanced KOA, in whom conservative treatment has not been effective. Surgery provides definitive treatment for KOA (KL grade IV).3, 8 The most common methods of treating KOA include chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs), intra-articular injections, limb offloading, rehabilitation, and physical therapy.6, 7 These methods relieve symptoms but do not stop disease progression or repair damaged tissues.
The field of orthobiological treatments for osteoarthritis is broad, with several therapies demonstrating potential in decreasing inflammation, supporting tissue regeneration, and enhancing joint functionality.9 Blaga et al. highlight numerous clinical benefits of platelet-rich plasma (PRP), including its minimally invasive nature, favorable safety profile, and the fact that most adverse events are related to the injection procedure itself rather than the substance. Additionally, PRP promotes faster recovery and does not trigger an immune response.10 Soufan et al. also pointed out that both intra-articularly administered PRP and hyaluronic acid (HA) did not exhibit systemic side effects, unlike anti-inflammatory drugs.11 It is crucial to recognize that the efficacy of treatment outcomes is likely affected by variables such as the composition of the product, the dosage administered, and the method of application, with these factors varying according to the specific classification of the disease being addressed.12 Finally, it is essential to consider that therapies such as PRP may encounter challenges related to regulatory compliance under Good Manufacturing Practice (GMP) standards, which can hinder the integration of these solutions into routine clinical practice.
Among the intra-articular injections, HA and PRP obtained from the patient’s blood are widely used. Both HA, which is a natural component of synovial fluid and influences the synthesis of proteoglycans and glycosaminoglycans, and PRP,13, 14 rich in platelets, leukocytes, growth factors, cytokines and other plasma proteins,15 have anti-inflammatory and chondroprotective effects, contributing to pain reduction and improved joint function.16, 17 Hyaluronic acid improves viscoelasticity, increasing shock absorption, reduces synovial inflammation and protects cartilage. Hyaluronic acid can bind to the CD44 receptor of chondrocytes and reduce interleukin (IL)-1β expression, which decreases activity of matrix metalloproteinases (MMPs): 1, 2, 3, 9 and 13. Platelet-rich plasma, rich in growth factors, modulates the inflammatory response, regulate sangiogenesis and cell differentiation, and stimulates endogenous HA synthesis.3 Platelet-rich plasma and HA have shown effectiveness in reducing KOA symptoms and improving joint function in many randomized controlled trials (RCTs) and systematic reviews.
Hyaluronic acid predominantly reinstates the viscoelastic characteristics of synovial fluid, alleviating pain via mechanical support for cartilage, whereas PRP promotes chondrocyte proliferation, cartilage formation, and endogenous HA synthesis; postinjection adverse effects are generally minimal, encompassing transient pain, swelling, or minor joint limitations that subside within days.1
Despite numerous studies supporting the effectiveness and safety of HA and PRP individually, research on the simultaneous use of both treatment methods remains scarce. Investigating this combination is essential for elucidating the potential synergistic benefits and guiding clinical practice. The combined action of PRP and HA, through distinct yet complementary mechanisms, could have a synergistic effect: PRP promotes tissue repair and regeneration, while HA improves joint lubrication and protects cartilage.18 This study seeks to provide a robust evidence base for the use of PRP + HA in the treatment of KOA, potentially offering a more effective alternative to current management strategies. By advancing our understanding of the role of biological therapies in treating degenerative joint diseases, this study could significantly impact patient care and quality of life for those suffering from KOA.
Objectives
The aim of this study was to evaluate the efficacy of combined PRP and HA treatment in treating KOA, focusing on pain relief, functional improvement, and inflammation reduction compared to PRP alone. We hypothesized that the synergistic action of PRP and HA, through their distinct biological mechanisms, would result in enhanced therapeutic effects in alleviating KOA symptoms and improving joint function.
Materials und methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines19 and followed the recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions.20 The protocol for this review was registered with the International Prospective Register of Systematic Reviews (Registration ID: CRD42024510649).
Search strategy and study selection
We searched electronic databases including PubMed, CENTRAL (Cochrane Controlled Trials Register), Web of Science, and Embase for relevant studies published between the databases’ inception and 24 July 2024. The following search strategy was used to optimize both search specificity and sensitivity, with the following keywords and phrases: “Platelet Rich Plasma” OR “Plasma, Platelet-Rich” OR “PRP” AND “Hyaluronic Acid” OR “HA” OR “Hyaluronate, Sodium” OR “Hyaluronate Sodium” AND “knee” AND “osteoarthritis” OR “osteoarthritides” OR “osteoarthr*” OR “arthrosis” OR “degenerative arthr*” OR “knee OA”.
The search was limited to studies published in English. Additional studies were identified by manually searching the reference lists of all eligible studies and relevant review articles. Where necessary, authors were contacted via email to request additional information or clarifications. Two researchers (M.T. and M.A-J.) conducted the literature search separately, and any discrepancies were resolved through consensus, with the senior author (Ł.S.) facilitating discussions.
All search records were independently screened for eligibility by 2 authors (M.T. and M.P.). Each author independently documented their findings, providing justifications and comments for each decision. When there was a difference of opinion, the senior author (Ł.S.) facilitated reaching an agreement by engaging in a discussion.
The results were subsequently transferred to the web platform Rayyan (https://www.rayyan.ai), which serves as a repository to simplify the process of eliminating duplicates and independently screening potential records.21 The initial screening process involved reviewing titles and abstracts and removing repeated studies. Subsequently, the full texts of potentially relevant articles were carefully assessed to determine whether they met the inclusion criteria.
Inclusion and exclusion criteria
We included all studies that met the following evidence-based PICOS criteria: 1) Patients: adult patients with KOA; 2) Intervention: PRP + HA; 3) Comparator: PRP alone; 4) Outcomes: contained complete original data, including at least 1 of the following: visual analogue scale (VAS) score, International Knee Documentation Committee (IKDC) score,22 and Knee Injury and Osteoarthritis Outcome Score (KOOS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score,23 or adverse events related to the treatment method; 5) Study design: RCTs and non-RCTs. We considered all published literature in addition to selected gray literature and preprints that provided full-length reports.
We used the following exclusion criteria: 1) unpublished data; 2) review studies, congress abstracts, letters to the editor, and clinical trial abstracts; 3) research lacking patient outcome scores; 4) non-human model studies; and 5) basic science studies.
Outcome and data extraction
Relevant data from the included articles were extracted by a pair of independent authors (M.T. and M.P. or B.M. and M.A-J.) into a structured template to ensure consistency and accuracy. If necessary, we communicated with the corresponding authors to clarify details or request raw data on specific endpoints. Any discrepancies were resolved through discussion with all the authors until a consensus was reached. The following data points were extracted from the included publications: 1) study characteristics (i.e., authors, article title, country, study design, length of follow-up), 2) demographic data of participants (i.e., number of participants, age, sex, body mass index (BMI), severity of KOA); and 3) outcome scores (i.e., VAS, KOOS, IKDC, WOMAC, and adverse events).
For data synthesis across studies, primary outcome measures were documented, including WOMAC and KOOS scores, as well as the VAS at 6 months post-intervention.
Secondary outcomes included the number of patients reporting adverse events.
Outcomes at 1, 3, 6, 12, 18, and 24 months post-intervention were assessed where available. In addition, changes in scores relative to baseline measurements were calculated for each time point.
Risk of bias and quality of evidence assessment
Two reviewers (M.T. and M.A-J.; blinded for review purposes) assessed the quality of the eligible studies independently, and the senior author (Ł.S.) resolved any discrepancies. The Cochrane Risk of Bias tool (ROB 2) was used to assess the following domains: 1) random sequence generation, 2) allocation concealment, 3) blinding of participants and personnel, 4) blinding of outcome assessment, 5) completeness of outcome data, 6) selective outcome reporting, and 7) other potential sources of bias.24 For non-RCTs, the ROBINS-I tool was used, and the following domains were assessed: 1) confounding, 2) selection of participants, 3) classification of interventions, 4) deviations from the intended interventions, 5) missing data, 6) measurement of outcomes, and 7) selection of the reported results.25 Each domain was categorized as unclear, low, or high risk. These assessments, both individual and overall, were based on the criteria outlined in the ROB 2 tool.24
Data analysis and statistical methods
For data analysis and statistical evaluation, we used RevMan 5.4 software (The Cochrane Collaboration, Oxford, UK) and Stata v. 18 (StataCorp, College Station, USA). The threshold for statistical significance across all study outcomes was set at a p-value of 0.05 (two-sided). We calculated standardized mean differences (SMDs) with 95% confidence intervals (95% CIs) for continuous outcomes and odds ratios (ORs) or risk ratios (RRs) with 95% CIs for dichotomous outcomes, allowing the inclusion of zero-event studies to estimate the pooled effects. In cases where studies presented continuous outcomes via medians and ranges, means and standard deviations (SDs) were calculated using the approach proposed by Hozo et al.26 Our analysis was based on a random-effects model to account for variations across studies. The Q-value statistical test and I2 index were used to evaluate heterogeneity. Statistical heterogeneity was classified into 3 categories: high (I2 > 80%), moderate (I2 = 25–79%), and low (I2 < 25%).27 To detect publication bias, we applied Egger’s test and generated funnel plots, focusing on asymmetry in analyses involving more than 10 studies. Sensitivity analysis was conducted using a leave-one-out approach.
Results
Literature search
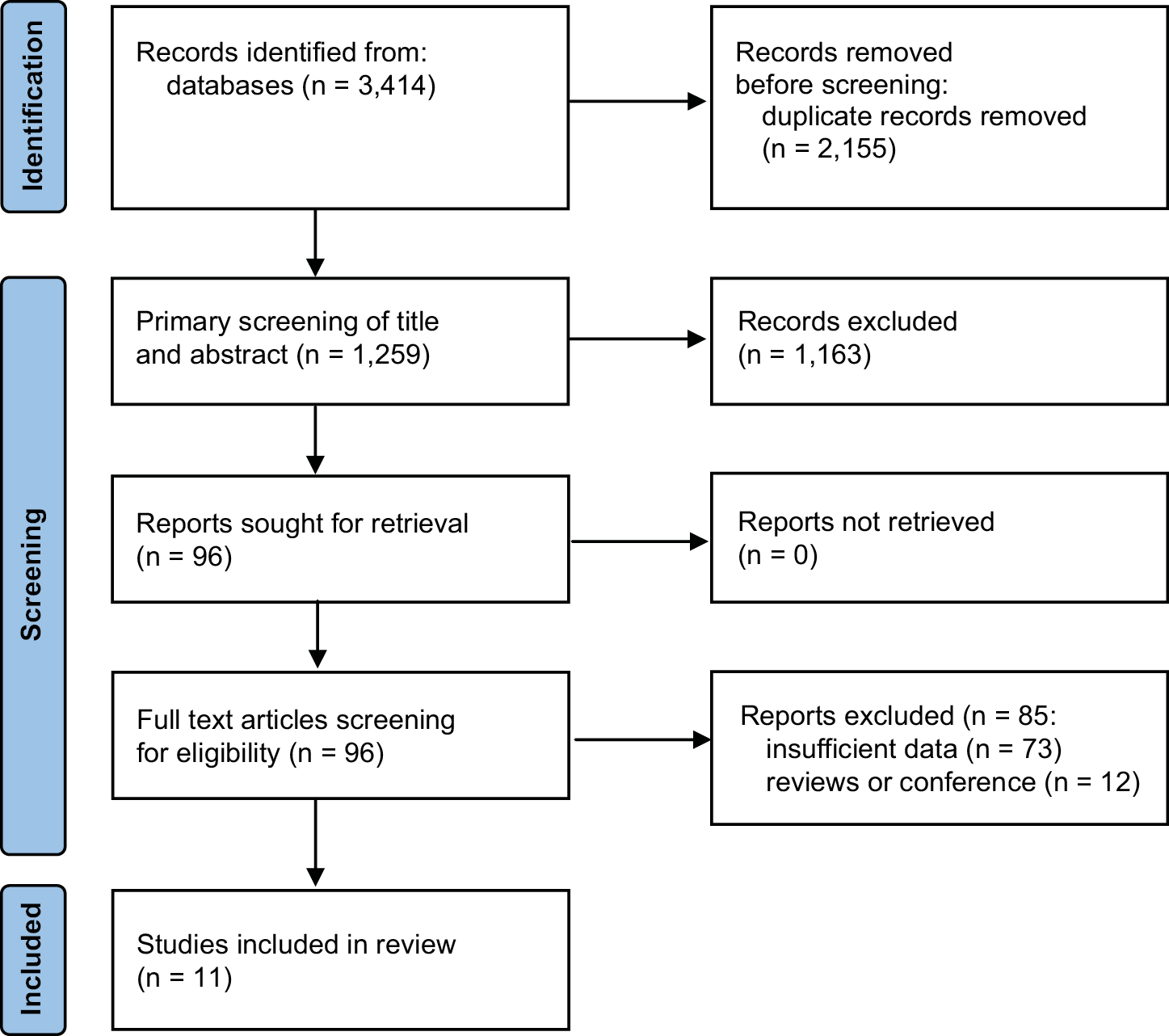
The search process yielded a total of 3,414 articles (Figure 1). After removing 2,155 duplicates, 1,163 articles were further excluded after a preliminary review of titles and abstracts, resulting in 96 studies. Among these articles, 85 were excluded based on full-text screening. Finally, 11 publications were selected for meta-analysis.1, 3, 6, 18, 28, 29, 30, 31, 32, 33, 34
The risk of bias for all included studies was assessed as low, as determined using the RoB2 and ROBINS-I tools. A detailed breakdown of the risk of bias assessment is illustrated in Supplementary Fig. 1–4.
Study and patient characteristics
The final analysis involved 11 studies, published between 2015 and 2023, comprising 892 participants, with 452 in the PRP + HA group and 440 in the PRP group. The trials were conducted in China,28, 30, 33, 34 Italy,1, 6, 29 the USA,18 India,31 Brazil,32 and Taiwan.3 The mean age of the subjects ranged from 46.2 to 62.71 years. There were 8 RCTs and 3 retrospective studies. The follow-up period ranged from 1 day to 24 months. The characteristics of the included studies appear in Table 1.1, 3, 6, 18, 28, 29, 30, 31, 32, 33, 34
VAS score by timeframe
At baseline, there was no significant difference in VAS scores between the PRP + HA and PRP groups (5.82 ±2.71 vs 5.66 ±2.96, respectively; SMD = 0.04; 95% CI: −0.13 to 0.21; p = 0.67; Table 2).
There was also no significant difference in follow-up periods, except at 6 months (2.23 ±2.18 vs 2.51 ±2.25; SMD = −0.41; 95% CI: −0.64 to −0.17; p < 0.001) and 24 months (1.70 ±0.60 vs 4.60 ±1.00; SMD = −3.45; 95% CI: −4.46 to −2.44; p < 0.001) after treatment (Supplementary Fig. 5).
The pooled median change from baseline in the PRP + HA group was significantly higher than in the PRP group at the 24-month follow-up (−2.7 ±0.2 vs 0.4 ±0.23, respectively; SMD = −14.10; 95% CI: −17.41 to −10.79; p < 0.001; Figure 2).
Sub-analysis of RCTs showed statistically significant differences between the PRP + HA and PRP groups only at 6-month and 24-month follow-ups (2.57 ±2.38 vs 2.87 ±2.0; SMD = −0.49; 95% CI: −0.77 to −0.21; p < 0.001 and 1.70 ±0.60 vs 4.60 ±1.0; SMD = −3.45; 95% CI: −4.46 to −2.44; p < 0.001; Table 2).
Analysis of changes in values using the VAS showed statistically significant differences from baseline only after 24 months (−2.7 ±0.2 for PRP + HA vs 0.4 ±0.23 for PRP; SMD = −14.10; 95% CI: −17.41 to −10.79; p < 0.001; Supplementary Fig. 6).
WOMAC score by timeframe
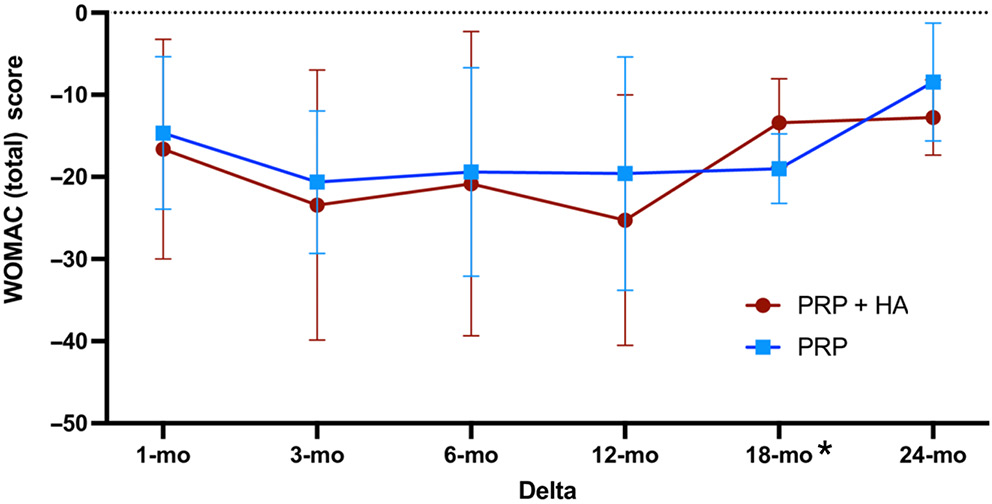
Baseline WOMAC scores were similar across both PRP + HA and PRP groups (46.11 ±26.23 vs 45.15 ±25.18; SMD = 0.14; 95% CI: −0.17 to 0.46; p = 0.36; Supplementary Fig. 7). All studies were RCTs. Statistically significant differences were noted at the 12-month follow-up, with the PRP + HA group showing a more substantial reduction in WOMAC scores (24.38 ±23.8 vs 28.33 ±24.95; SMD = −0.53; 95% CI: −1.00 to −0.05; p = 0.03). Mean changes between the 12-month follow-up and baseline revealed statistically significant differences in WOMAC score between PRP + HA and PRP groups (−25.26 ±15.24 vs −19.6 ±14.20; SMD = −0.95; 95% CI: −1.66 to −0.23; p = 0.010), as well as between the 18-month follow-up and baseline (−13.4 ±5.35 vs −19.6 ±14.2; SMD = 1.15; 95% CI: −16.04 to 5.83; p < 0.001; Figure 3).
Detailed WOMAC subscale (pain, stiffness, and function) values are shown in Table 2. A graphic representation of the differences between the measurements and baseline in each subscale is illustrated in Supplementary Fig. 8, Supplementary Fig. 9, and Supplementary Fig. 10, respectively.
KOOS scale by timeframe
Only 3 studies reported KOOS scores in PRP + HA and PRP patient groups. There were no statistically significant differences in the KOOS score either at baseline (60.07 ±16.44 vs 58.15 ±17.58; SMD = 0.14; 95% CI: −0.33 to 0.61; p = 0.57) or during individual follow-ups (1, 3, 6, 12, and 18 months after treatment; p > 0.05; Supplementary Fig. 11). Even when analyzing the differences between individual time points and baseline, no statistically significant differences were noted between the study groups (Figure 4). Only 1 RCT reported the KOOS scale in the study groups. No statistically significant differences were noted between PRP + HA and PRP at any of the time points (p > 0.05). A similar situation occurred when analyzing the differences in values between individual time points and baseline (Supplementary Fig. 12).
IKDC scale by timeframe
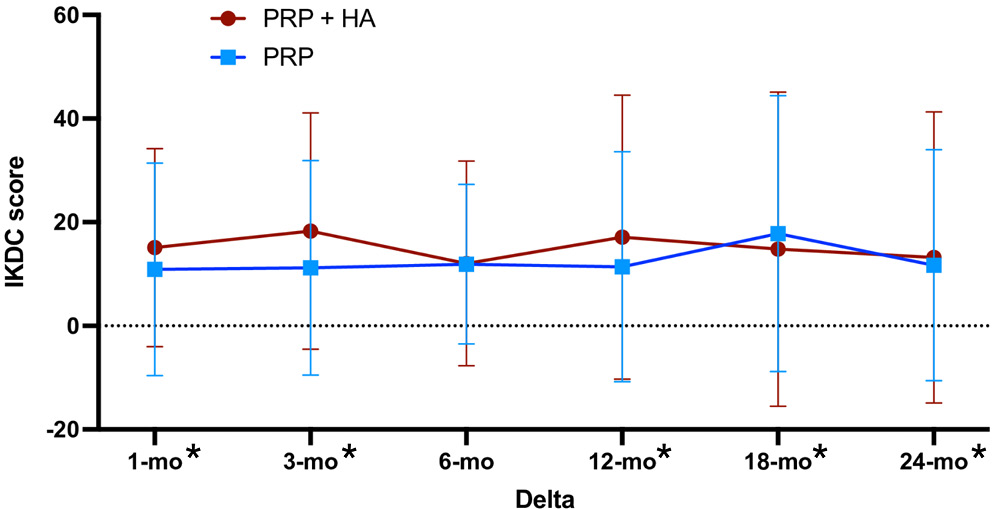
Two studies reported IKDC scores in the PRP + HA and PRP groups, and both studies were RCTs. Pooled analysis showed no significant difference between these groups at baseline (37.42 ±15.03 vs 37.47 ±10.42; SMD = 0.02; 95% CI: −0.35 to 0.39; p = 0.92), as well as across all follow-up periods (1, 3, 6, 12, 18, and 24 months; Supplementary Fig. 13). Changes in IKDC scores across different follow-up time points and baseline showed no statistically significant differences between the study groups in any of the outcome measures (Figure 5).
Discussion
The presented meta-analysis offers an in-depth exploration into the effectiveness of PRP therapy, both as a standalone treatment and in combination with HA, in the management of KOA. This discussion integrates findings from the meta-analysis with a comprehensive review of existing literature to contextualize the impact of PRP and HA on patient outcomes, specifically focusing on pain reduction, functional improvement, and improvement in patients’ overall quality of life.
The meta-analysis meticulously selected data from a broad spectrum of studies, narrowing down to 11 publications deemed suitable for rigorous scrutiny. This careful selection and synthesis process, which mirrored the comprehensive approach of Ciapini et al., not only underscores the current evidence but also reveals the nuanced benefits of PRP, with or without the addition of HA, in the management of KOA.29
When combined, PRP and HA jointly stimulate local angiogenesis, though PRP plays a more prominent role in this process by encouraging healthy surrounding cells to produce additional growth factors. Furthermore, PRP has demonstrated anti-nociceptive effects.35, 36, 37 Research by Lana et al. suggests that HA serves as a supportive matrix for cartilage repair and improves the mechanical properties of cartilage.32
The observed improvements, as noted in the WOMAC Pain Assessment (WOMAC PA) scores, typically manifest between 30 and 90 days post-treatment, aligning with the timeframe for these molecular and cellular modifications to take effect. This combination therapy may result in better rehabilitation and earlier return to activities of daily living.
This meta-analysis unveils a notable variation in the efficacy of PRP across different timeframes and outcome measures. This observation resonates with the findings of Guo et al.,30 who reported no significant disparities in functional outcomes between groups treated with PRP in combination with HA and those treated with PRP alone. However, they hinted at a potential for improved functional scores with the combination therapy. This trend suggests that while PRP alone can impart beneficial effects, its combination with HA might enhance or extend these outcomes, warranting further investigation, as suggested by Ciapini et al.29 Furthermore, the meta-analysis highlights a critical period of enhanced efficacy specifically at the 6-month and 24-month follow-ups, particularly notable in PRP + HA treatments. This timeframe-dependent effectiveness aligns with observations made by Yu et al.28 and Wu et al.,3 who observed significant improvements in pain relief and functional scores at similar intervals. These findings suggest the potential for PRP and HA therapies to induce lasting therapeutic benefits, offering a robust alternative to the transient nature of symptomatic treatments currently used in KOA management paradigms.
Notably, the sub-analysis of RCTs within the meta-analysis revealed statistically significant differences in outcomes favoring PRP + HA combinations at specific follow-up intervals. This echoes the systematic approach of Lana et al.32 and Jacob et al.,31 which emphasized the value of RCTs in establishing the efficacy of PRP treatments. The consistent observation across these studies of improved outcomes with PRP + HA interventions reinforces the potential of combinatory therapies for improving KOA care.
The analysis extends to the nuanced roles of WOMAC and KOOS scores as outcome measures, reflecting patient-reported assessments of pain, stiffness, and functional capacity. The meta-analysis, through its elaborate examination of these scores, highlights the complex nature of KOA symptoms and how distinct treatments uniquely address these issues. Such an approach mirrors the detailed analyses conducted by Palco et al.6 and Sun et al.,34 which also utilized these scales to discern the therapeutic value of PRP and HA interventions. The consistency between these studies highlights the critical role of patient-centered outcomes in evaluating the success of KOA treatments.
Recent meta-analyses highlight the significant clinical utility of PRP and HA, underscoring the relevance of the topic explored in this meta-analysis. Bensa et al. demonstrated that corticosteroid injections for KOA yield results comparable to HA and PRP only in the short term, whereas PRP shows clear superiority in longer-term follow-ups.38 Moreover, Qiao et al. found that PRP and HA, including when used in combination therapy, do not present a higher risk of treatment-related adverse events compared to placebo. It is important to note that the absence of elevated safety risks also applies to corticosteroid use.39 Regarding the most effective intervention strategy, a meta-analysis by Tao et al. revealed that repeated PRP treatments are more effective than a single administration.40
Moreover, this study critically examines the risk of bias in the included studies, utilizing established tools such as the RoB2 and ROBINS-I. This thorough scrutiny of study quality ensures that conclusions drawn are based on evidence of the highest integrity, a principle that is paramount in the realm of evidence-based medicine. This commitment to maintaining strict methodological standards is reflected in the studies included in this review, all of which strive to contribute to a more reliable and comprehensive understanding of PRP and HA therapies in osteoarthritis management.
The assessment of pain and functional outcomes in most studies relied heavily on subjective scales such as the VAS and the WOMAC, which could potentially limit the objectivity of the results. The selection of the IKDC and WOMAC scores as endpoints (surrogate measures) was made due to their broad application in clinical studies in this field. The WOMAC score is a self-reported tool used by patients to evaluate their pain, stiffness, and physical function in relation to osteoarthritis. Patients rate each item based on their experience, typically using a Likert scale (0–4) or a VAS.41 In contrast, the IKDC score combines physician assessments with patient-reported outcomes and assesses knee function, particularly after injuries such as ligament tears. This score integrates clinical evaluations with patients’ subjective assessment of knee symptoms, functionality, and activity levels.42 The use of objective assessment methods such as the single-leg stance (SLS) test, which was used in Sun et al.,34 or the Biodex Balance System SD, used in Wu et al.,3 may contribute to greater objectivity in research and a better comparison of both treatment methods. Furthermore, advanced imaging tests such as magnetic resonance imaging (MRI), despite their costs and time requirements, could also contribute to improving the quality of research. Adding a control group receiving saline injections, which is often used as a placebo in intra-articular research, could also set a clear baseline for judging how well the treatment works.
The selection of appropriate patients for the studies is critical. As indicated by Jacob et al., patient weight plays a crucial role due to its significant impact on articular cartilage damage.31 Long-term studies should consider changes in patient body weight, as weight reduction alone can stop disease progression irrespective of the treatment. Palco et al. highlighted the importance of disease stage in analyzing treatment outcomes: most studies on the conservative treatment of KOA mainly include patients in the early stages, while stages III and IV are less represented. It is hypothesized that the use of combined PRP + HA may benefit individuals with advanced stages of the condition.6 The selection and administration methods of treatments also present a significant consideration. The study by Wu et al. was probably the first study in which a different drug administration protocol was used, as PRP was administered 1 week prior to HA, diverging from the concurrent administration seen in prior studies.3 This approach yielded comparable or superior results, highlighting the need for further optimization of administration protocols.
Future scientific research should focus, among other things, on deepening the understanding of the biological mechanisms underlying the effects of PRP and HA, both individually and in synergy. Gaining insight into these mechanisms may lead to the discovery of substances with similar potential applications in intra-articular injections. From a clinical standpoint, further investigation is needed into the optimal injection protocols, including timing intervals. For instance, it would be important to determine whether more intensive treatment could significantly reduce the risk of KOA progression, which holds critical clinical relevance. Additionally, there is a need for a more comprehensive analysis of the endpoints used in clinical trials. It seems essential to implement 2 types of measurement scales in such studies: one that is self-reported by patients, and another completed by clinicians, preferably independent raters not directly involved in the care of trial participants. Lastly, the use of radiologically based endpoints should be encouraged and combined with these measurement scales. Furthermore, the reliance on highly experienced physicians for performing high-frequency color Doppler imaging, without a standardized practitioner for all examinations, may introduce variability in the measurement outcomes. Coupled with the lack of long-term follow-up data to evaluate the enduring effects of the treatments and the possible unaccounted use of concurrent analgesic or anti-inflammatory medications, these factors support a cautious interpretation of the findings. They also highlight the need for further research with more rigorous methodologies and involving larger, more homogeneous study populations.
Limitations of the study
We acknowledge several limitations of this research that may impact the breadth of its applicability and the interpretation of its outcomes. First, the variability in pre-treatment inflammation levels and synovial conditions, potentially influenced by patients’ NSAID or steroid use, introduces a degree of heterogeneity within the study cohorts, complicating direct comparisons. Additionally, the inclusion of patients receiving bilateral injections might increase population heterogeneity, though it reflects real-life clinical scenarios. The observed differences in the effectiveness of PRP combined with HA in treating different knee compartments, attributed to varying stress distributions, highlight the complexity of osteoarthritis treatment and underscore the necessity for individualized therapeutic approaches. Furthermore, some outcomes were reported by only 1 study; while these results were included for thoroughness, they do not constitute aggregated estimates. These instances were distinctly categorized and should be regarded as single-study results rather than meta-analytic compilations.
Conclusions
This meta-analysis underscores the efficacy of PRP, either independently or in conjunction with HA, as a viable treatment for KOA, especially in alleviating pain and enhancing functionality over time. Notable advantages were evident at 6 and 24 months, indicating a synergistic effect. Nonetheless, clinical implications must be evaluated with caution due to variability across the studies. To improve evidence-based treatment methods, future research should focus on large, high-quality trials that investigate the underlying biological mechanisms of this therapy.
Use of AI and AI-assisted technologies
Not applicable.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.16979738. The package contains the following files:
Supplementary Fig. 1. A summary table of review authors’ judgements for each risk of bias item for RCT.
Supplementary Fig. 2. A summary table of review authors’ judgements for each risk of bias item for non-RCT.
Supplementary Fig. 3. A plot of the distribution of review authors’ judgements across RCTs for each risk of bias item.
Supplementary Fig. 4. A plot of the distribution of review authors’ judgements across non-RCTs for each risk of bias item.
Supplementary Fig. 5. Forest plot of VAS scores among PRP + HA and PRP patients (results derived from single studies do not constitute a pooled analysis and should be interpreted with caution due to the limited generalizability of such findings).
Supplementary Fig. 6. The evolution of the mean VAS scores changes from baseline in the research groups in RCTs sub-analysis.
Supplementary Fig. 7. Forest plot of WOMAC (total) scores among PRP + HA and PRP patients (results derived from single studies do not constitute a pooled analysis and should be interpreted with caution due to the limited generalizability of such findings).
Supplementary Fig. 8. The evolution of the mean WOMAC pains subscale changes from baseline in the research groups.
Supplementary Fig. 9. The evolution of the mean WOMAC stiffness subscale changes from baseline in the research groups.
Supplementary Fig. 10. The evolution of the mean WOMAC function subscale changes from baseline in the research groups.
Supplementary Fig. 11. Forest plot of KOOS scores among PRP + HA and PRP patients (results derived from single studies do not constitute a pooled analysis and should be interpreted with caution due to the limited generalizability of such findings).
Supplementary Fig. 12. The evolution of the mean KOOS scores changes from baseline in the research groups in RCTs sub-analysis.
Supplementary Fig. 13. Forest plot of IKDC scores among PRP + HA and PRP patients.
Supplementary Table 1. Pooled results of different scales among PRP + HA and PRP in subgroup of RCT trials.
.jpg)
.jpg)