Abstract
Background. No comprehensive comparative research has been conducted to evaluate open Bankart (OB), arthroscopic Bankart (AB), open Latarjet (OL), and arthroscopic Latarjet (AL) simultaneously across all relevant clinical outcomes and parameters.
Objectives. To compare the efficacy of OB, AB, OL, and AL procedures in the treatment of shoulder dislocation.
Materials and methods. The databases PubMed, Embase, the Cochrane Library, and Web of Science were utilized for the literature search. The study evaluated recurrent instability, re-dislocation, apprehension, functional outcomes, and postoperative pain. The results were visually represented through network diagrams, forest plots, league tables, and rank probability plots to provide a comprehensive understanding of each outcome.
Results. Overall, 37 studies were included in the analysis. Individuals who underwent OL experienced a notably reduced risk of recurrent instability compared with those who underwent AB (random-effects model pooled relative risk (RR) = 0.34, 95% credible interval (95% CrI): 0.24–0.48) and OB (random-effects model pooled RR = 0.51, 95% CrI: 0.31–0.85). The risk of re-dislocation was also significantly lower for patients treated with OL compared with AB (pooled RR = 0.15, 95% CrI: 0.04–0.45). While not statistically significant, the OL procedure tended to have the lowest risk of apprehension and the highest Subjective Shoulder Value (SSV) score. Regarding postoperative pain, patients who underwent OB had the highest likelihood of attaining the lowest scores on the visual analogue scale (VAS). In addition, OL was associated with the highest probability of complications.
Conclusions. The open Latarjet procedure appears to offer superior shoulder stability; however, while functional outcomes for patients undergoing OL are likely to be non-inferior, the procedure is not significantly associated with reduced postoperative pain as measured with the VAS score. Additionally, the OL procedure is associated with an increased likelihood of complications. Consequently, it is essential to implement preventive measures to manage postoperative pain and address potential complications following OL procedure.
Key words: network meta-analysis, shoulder dislocation, Bankart, Open Latarjet, arthroscopic treatment
Introduction
The shoulder joint is the most frequently dislocated joint in the human body, with an incidence of approx. 23.96 per 100,000 individuals annually.1 Its high mobility and relatively shallow glenoid cavity make it particularly susceptible to instability, especially following traumatic events.1 Injuries to the static (e.g., labrum, ligaments) and dynamic (e.g., muscles) stabilizers of the shoulder can lead to instability, with anterior shoulder instability being the most common form, typically resulting from traumatic events.2, 3 Conservative management is frequently selected for patients who are not candidates for surgery, despite the higher risk of recurrence.4 Surgical stabilization represents an effective treatment option when conservative management fails, providing durable fixation and a more definitive resolution of instability.5
Traditional open Bankart (OB) repair was historically regarded as the standard surgical treatment for shoulder stabilization.6, 7 This technique has been shown to improve joint stability and is associated with low recurrence rates.8, 9, 10, 11 However, despite its effectiveness, the open approach has certain disadvantages, including restricted external rotation and an increased risk of secondary osteoarthritis.12
Arthroscopic Bankart (AB) repair, first described in 1993, has gained increasing acceptance over the past decades owing to advances in arthroscopic techniques and improved surgical expertise.13, 14, 15 Compared with open procedures, arthroscopic repair offers several advantages, including smaller incisions, shorter operative time, reduced postoperative pain, and potentially fewer complications.16, 17, 18 However, some studies have reported higher recurrence rates of shoulder instability following AB repair compared with open repair.19, 20
The open Latarjet (OL) procedure is widely used for the management of anterior shoulder instability and is recognized for its effectiveness and reliability; however, it is associated with potential complications such as nonunion and infection.21, 22 Arthroscopic Latarjet (AL) has subsequently been introduced as a minimally invasive alternative. Emerging evidence indicates that AL achieves clinical outcomes comparable to OL, while potentially offering smaller incisions, fewer complications, faster graft healing, earlier rehabilitation, and the ability to address concomitant intra-articular pathologies.23, 24
Numerous studies have directly compared pairs of the 4 surgical techniques – OB, AB, OL, and AL – for the management of shoulder instability.25, 26, 27 Furthermore, several meta-analyses have evaluated the comparative effectiveness of OL compared with AL in recurrent anterior shoulder instability, as well as OB vs AB in the management of Bankart lesions.28, 29
Currently, multiple surgical interventions are available for managing shoulder dislocations; however, no single treatment has been proven superior. Additionally, there is a scarcity of studies evaluating OB, AB, OL, and AL across all relevant clinical outcomes and parameters.
Objectives
The current network meta-analysis aimed to compare the OB, AB, OL, and AL procedures for the treatment of shoulder dislocation.
Materials and methods
Search strategy
To ensure a thorough examination of the available literature, 2 independent investigators (Q.H. and W.Q.) conducted a comprehensive search across multiple databases, including PubMed, Embase, the Cochrane Library, and Web of Science. The search was completed on August 17, 2023, to gather the most recent and relevant studies for the network meta-analysis. English search terms included “Shoulder Dislocation” OR “Dislocation, Shoulder” OR “Dislocations, Shoulder” OR “Shoulder Dislocations” OR “Glenohumeral Dislocation” OR “Dislocation, Glenohumeral” OR “Dislocations, Glenohumeral” OR “Glenohumeral Dislocations” OR “Glenohumeral Subluxation” OR “Glenohumeral Subluxations” OR “Subluxation, Glenohumeral” OR “Subluxations, Glenohumeral” AND “Bristow” OR “Latarjet” OR “Bankart” OR “iliac bone graft” OR “Repair” OR “Putti-Platt” OR “Arthroscopies” OR “arthroscopic surgery” OR “Surgery” OR “Conservative” OR “nonoperative” OR “nonsurgical” OR “Physiotherapy” OR “Immobilization”. Disagreements concerning eligibility were resolved by another investigator (J.S.). Primary study selection was based on the titles and abstracts of the retrieved studies, followed by full-text screening. The present study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines, ensuring a transparent and methodologically rigorous approach to the systematic review and meta-analysis process.30
Eligibility criteria
The inclusion criteria for the study were as follows: 1) studies involving patients diagnosed with shoulder instability or dislocation; 2) studies in which patients underwent treatment with one of the 4 specified surgical procedures: OB, AB, OL, or AL; 3) evaluation of outcomes related to shoulder stability, functional outcomes, or postoperative pain; 4) study designs limited to randomized controlled trials (RCTs) and cohort studies.
The exclusion criteria were defined to ensure the relevance and quality of the included literature and included: 1) animal studies; 2) case reports; 3) studies with sample sizes of fewer than 10 participants; 4) studies not directly related to the topic, such as those involving patients without shoulder dislocation or instability, or those focusing on non-surgical treatments or procedures other than Bankart and Latarjet repairs; 5) editorial materials, conference abstracts, protocols, letters, guidelines, expert consensus documents, reviews, and meta-analyses, as these formats typically do not contain the level of detail or original data required for a systematic review and meta-analysis; 6) studies not published in English.
Outcome measures
In this analysis, the primary outcome of interest was shoulder stability, with specific measures including the incidence of recurrent instability, re-dislocation, and apprehension. The secondary outcomes encompassed functional outcomes and postoperative pain. Functional outcomes were measured using several standardized scales, including the Subjective Shoulder Value (SSV) score, reflecting the patient’s assessment of shoulder function; the American Shoulder and Elbow Surgeons (ASES) score, a comprehensive evaluation of shoulder function commonly used after shoulder surgery; the Rowe score, another scale specifically designed to assess shoulder function, with an emphasis on activities of daily living and sports; and forward flexion, a measure of range of motion indicating the extent to which the patient can raise the arm forward. Postoperative pain was quantified using the visual analogue scale (VAS).
Data extraction
The data extraction process from the included studies in the systematic review and network meta-analysis was comprehensive and included the following details: authors, year of publication, country, study design, population, intervention, sample size, male/female distribution, age (in years), body mass index (BMI, in kg/m2), glenoid bone loss, number of Hill–Sachs lesions, follow-up time (in months), and outcomes.
Quality assessment
In the systematic review and network meta-analysis, the quality assessment of the included RCTs was conducted using the modified Jadad scale.31 This scale allocates a total of 7 points, with RCT quality categorized as follows: 1–3 points indicating low quality and 4–7 points indicating high quality. For cohort studies, quality was evaluated using the modified Newcastle–Ottawa scale (NOS).32 The NOS assigns a total of 9 points, with quality ratings defined as follows: 0–3 points indicating poor quality, 4–6 points indicating fair quality, and 7–9 points indicating good quality.
Statistical analyses
A network meta-analysis was conducted using Stata v. 15.1 (StataCorp LLC, College Station, USA) and the gemtc 1.0.1 package in R v. 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria). A Bayesian framework and a Markov chain Monte Carlo (MCMC) model were employed for the analysis. To ensure model convergence, trace plots and diagnostic tools were utilized. The number of initial iterations in the Monte Carlo simulations was determined based on achieving a potential scale reduction factor (PSRF) close to 1, indicating satisfactory convergence. Additional iterations were performed if necessary.
The bandwidth value in the density plots served as a quantitative measure, with smaller values suggesting a closer fit to the preset distribution. Iterations were continued until the bandwidth stabilized near 0, ensuring robust model performance. The model consisted of 4 chains, with an initial iteration count of 20,000, followed by an additional 50,000 iterations, and a step length of 1. In the presence of network relationships, the model assessed consistency and potential discrepancies between direct and indirect treatment comparisons. When the difference between the Deviance Information Criteria (DIC) of the consistency and inconsistency models was less than 5, it indicated agreement between direct and indirect comparisons. Network plots were constructed for each outcome measure. Analyses were conducted using a random-effects model. For the Rowe score, SSV score, forward flexion, ASES score, and VAS, the weighted mean difference (WMD) and 95% credible intervals (95% CrIs) for different surgical interventions were reported. For recurrent instability, apprehension, re-dislocation, and complications, the relative risk (RR) values and 95% CrIs for different surgical interventions were reported. All direct and indirect comparisons of WMD or RR values with their corresponding 95% CrIs were presented in forest plots. The ranking of surgical interventions was predicted using a ranking plot, in which the probability of each intervention being ranked in the nth position was presented as a bar chart, with the horizontal axis indicating the corresponding rank.
Continuous variables were analyzed using the change from baseline as the final analysis outcome to reduce statistical errors arising from initial population imbalances in some cohort studies. An adjusted funnel plot was employed to evaluate potential publication bias. This approach is particularly relevant in the context of network meta-analyses, where traditional funnel plots may not adequately capture the nuances of multiple intervention comparisons. By using the adjusted funnel plot, symmetry of effect sizes across studies can be assessed more accurately, thereby providing a more robust evaluation of potential bias.
Results
Characteristics of the included studies
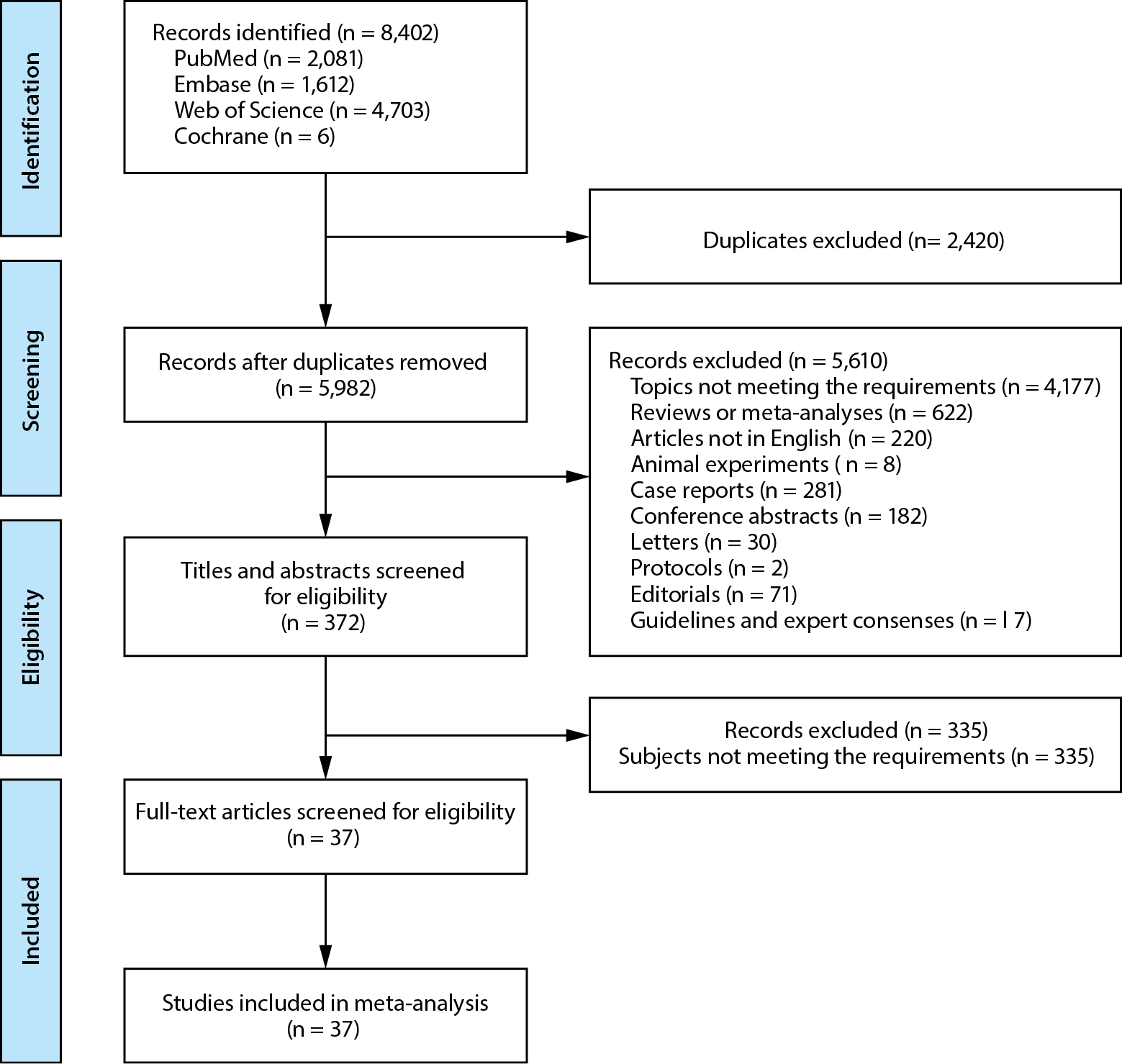
From the 4 databases, 8,402 studies were retrieved. After excluding duplicates, 5,982 studies remained for screening based on titles and abstracts, followed by full-text screening. Ultimately, 37 studies were included in this network meta-analysis, comprising 5 RCTs and 32 cohort studies.25, 26, 27, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66 Figure 1 illustrates the flow chart of the eligible study screening process. Of the included studies, 32 were of high quality and 5 were of fair quality. These studies were published between 1997 and 2023. The characteristics of the included studies are presented in Supplementary Table 1.
Shoulder stability
Recurrent instability
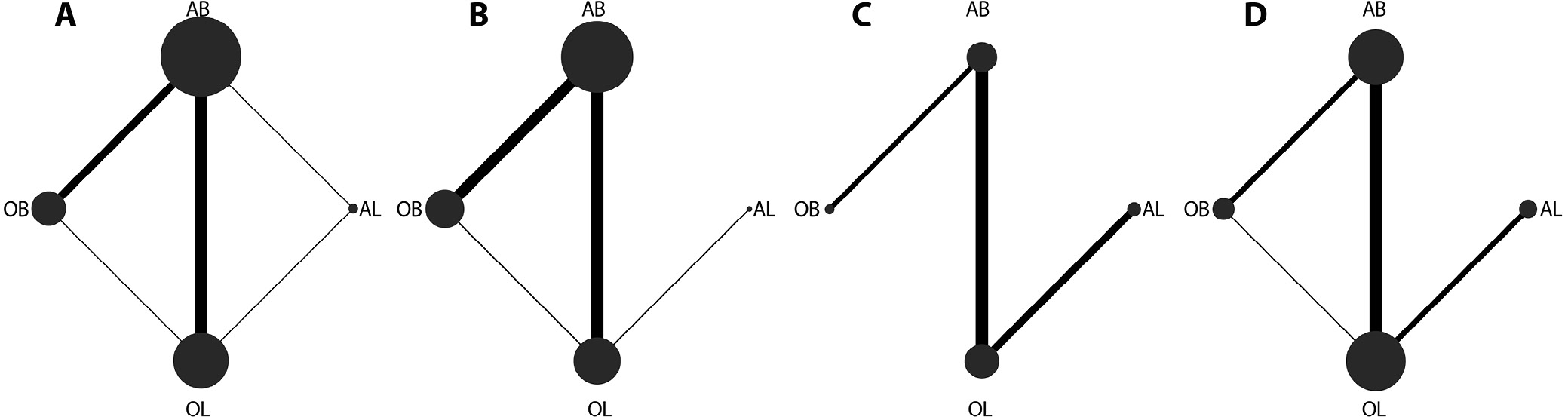
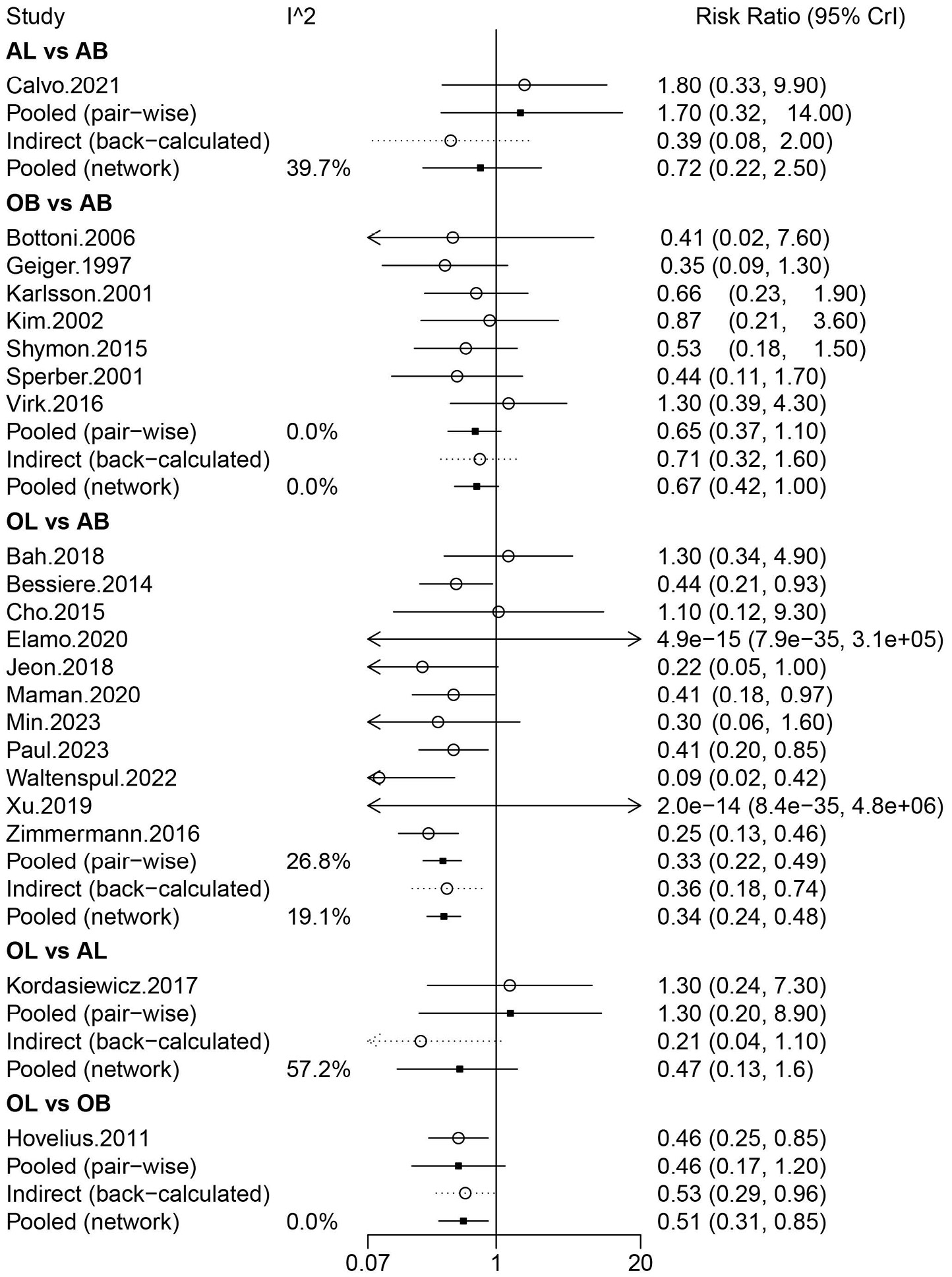
Information on recurrent instability was provided in 21 studies involving 2,300 patients, in which OB, AB, OL, and AL were compared. Arthroscopic Bankart was directly compared with OB, AL, and OL. There were more studies for the direct comparison between AB and OL (Figure 2A). The forest plot analysis using a random-effects model revealed that OL had a lower risk of recurrent instability than AB (pooled relative risk (RR) = 0.33, 95% CrI: 0.22–0.49) (Figure 3). The league table demonstrated that patients treated with OL had a significantly lower risk of recurrent instability than those treated with AB (random-effects model pooled RR = 0.34, 95% CrI: 0.24–0.48) and OB (random-effects model pooled RR = 0.51, 95% CrI: 0.31–0.85) (Table 1). The rank probabilities showed that OL was most likely to be the optimal procedure with regard to recurrent instability (Table 2). In the subgroup analysis restricted to primary surgical procedures, the pooled results analyzed using a random-effects model demonstrated that patients undergoing OL exhibited a significantly reduced risk of recurrent instability compared with those treated with arthroscopic AB (pooled RR = 0.39, 95% CrI: 0.20–0.60) (Supplementary Table 2).
Re-dislocation
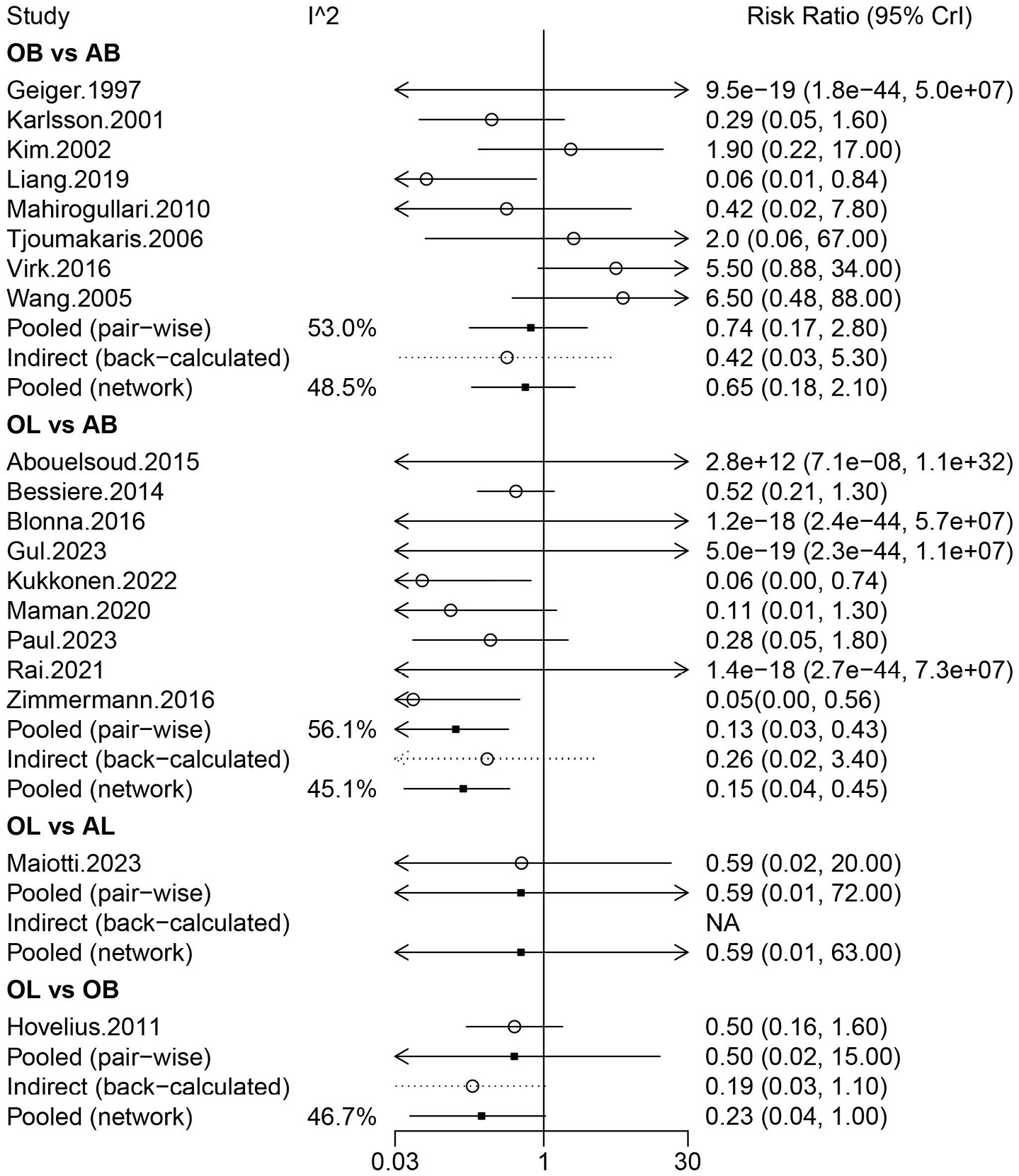
Nineteen studies involving 2,318 patients assessed the risk of re-dislocation after AB, OB, AL, and OL. Arthroscopic Bankart was directly compared with OB and OL, and OL was directly compared with OB and AL. More studies compared AB and OL (Figure 2B). Figure 4, based on the random-effects model analysis, also showed a lower risk of re-dislocation in patients treated with OL compared with AB (pooled RR = 0.13, 95% CrI: 0.03–0.43). The league table analysis using a random-effects model found that the risk of re-dislocation after OL was significantly lower than that after AB (pooled RR = 0.15, 95% CrI: 0.04–0.45) (Table 1). The rank probabilities showed that OL had the highest likelihood of being the optimal operation with regard to re-dislocation (Table 2). Based on the subgroup analysis of primary surgeries, OL was associated with a lower likelihood of re-dislocation compared with AB (random-effects model pooled RR = 0.14, 95% CrI: 0.03–0.39) and OB (random-effects model pooled RR = 0.11, 95% CrI: 0.01–0.66) (Supplementary Table 2).
Apprehension
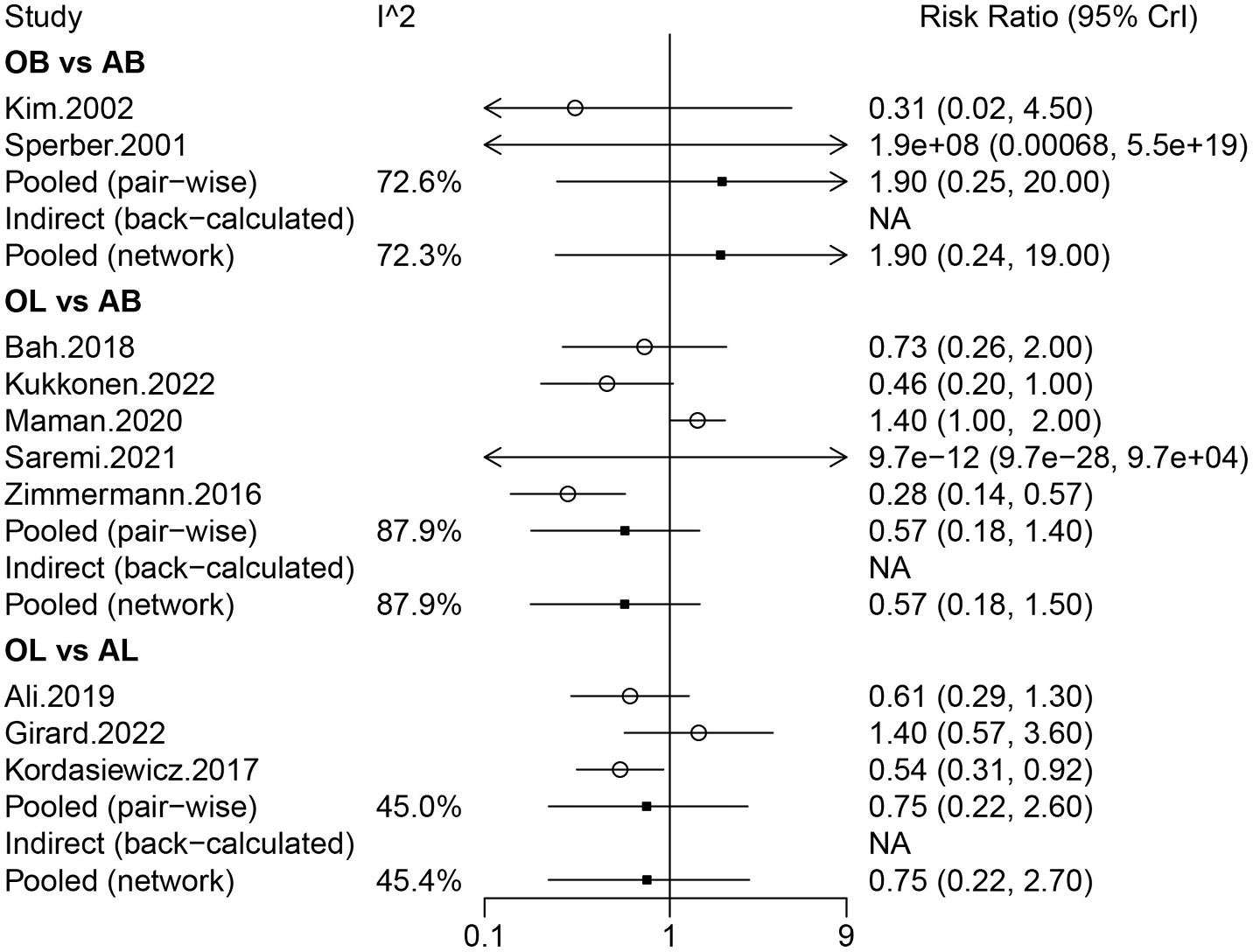
The risk of apprehension was evaluated in 10 studies including 1,195 patients. Arthroscopic Bankart was directly compared with OL and OB, and AL was directly compared with OL. More studies compared AB and OL (Figure 2C). The forest plot analysis using a random-effects model demonstrated that no significant difference was observed in the risk of apprehension among these 4 operations (Figure 5). Similarly, no significant difference was observed in the risk of apprehension among these 4 operations in the league table analysis using a random-effects model (Table 1). The rank probabilities showed that patients undergoing OL were most likely to have the lowest risk of apprehension (Table 2).
Functional outcomes
SSV score
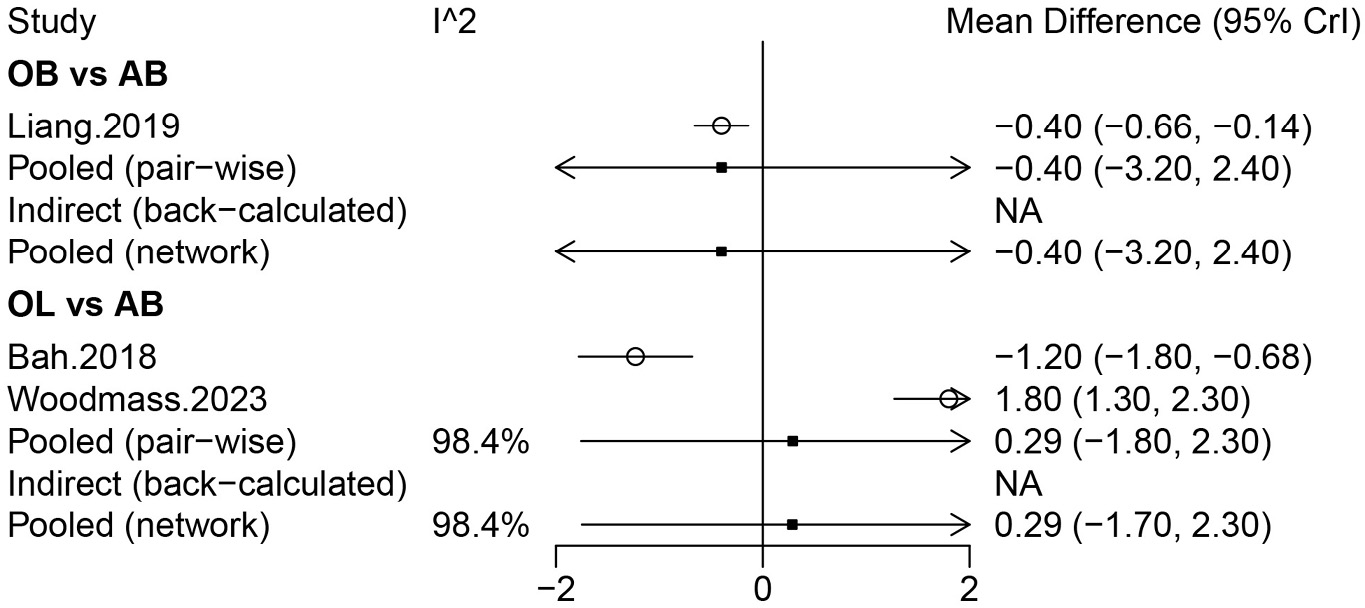
Three studies involving 500 patients investigated the SSV score, including AB, OL, and AL. No significant difference in the SSV score was found among these surgical treatments based on the forest plot and league table (Table 1). The rank probabilities suggested that OL was most likely to be associated with the highest SSV score (Table 2). Based on the subgroup analysis of primary surgeries, no significant difference in the SSV score was observed among these surgical treatments (Supplementary Table 2).
ASES score
Two studies involving 952 patients assessed the ASES score, including AB, OL, and AL. No significant difference was observed in the ASES score among these surgical treatments based on the league table analysis using a random-effects model (Table 1). The rank probabilities suggested that AB was most likely to be the best surgery with regard to the ASES score (Table 2).
Rowe score
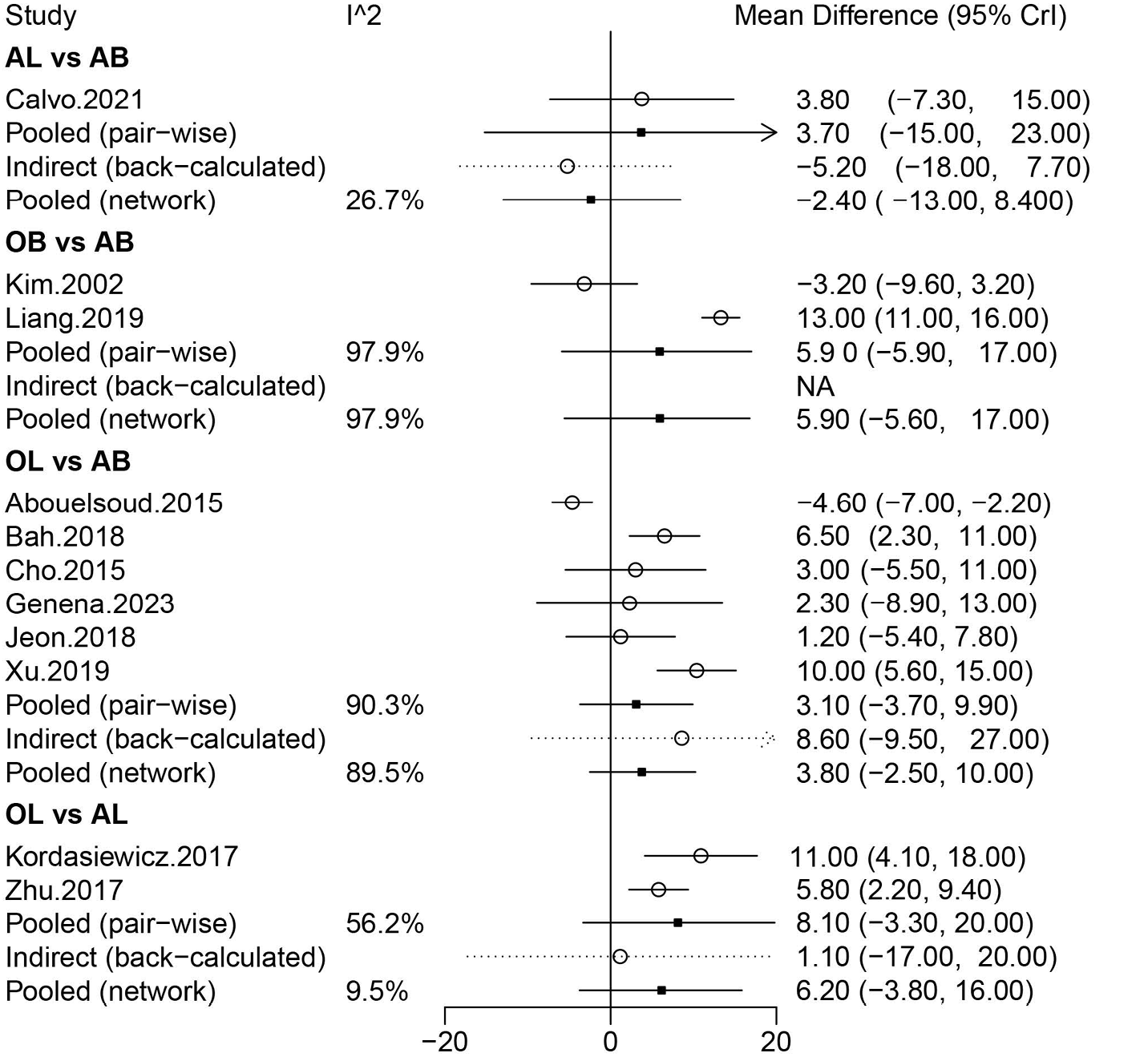
The Rowe score was evaluated in 11 studies involving 1,152 patients, and comparisons were made among OB, AB, OL, and AL. No significant difference in the Rowe score was found among these operations when the analysis was conducted using a random-effects model (Figure 6). Similarly, no significant difference in the Rowe score was observed among these operations in the league table analysis using a random-effects model (Table 1). The rank probabilities showed that OB had the highest likelihood of being the optimal procedure with regard to the Rowe score (Table 2).
Forward flexion
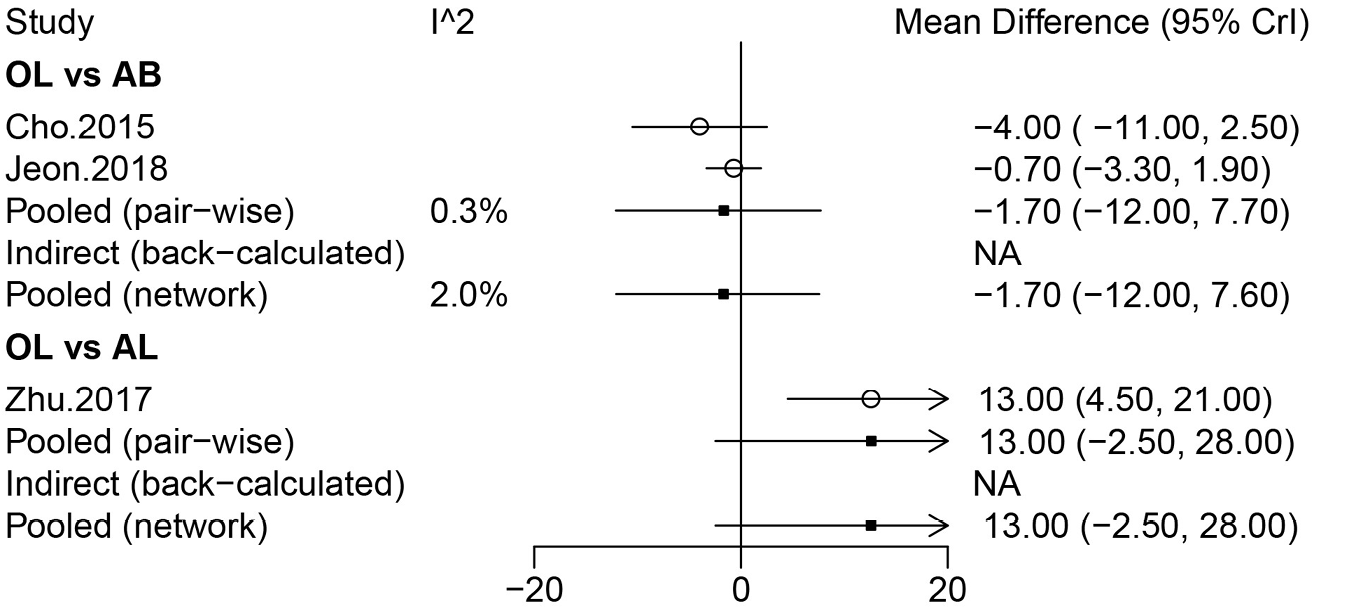
Three studies involving 311 patients provided data on forward flexion, including AB, OL, and AL. No significant difference in forward flexion was observed among the 3 operations in the forest plot analysis using a random-effects model (Figure 7). Similarly, no significant difference in forward flexion was observed among the 3 operations in the league table analysis using a random-effects model (Table 1). The rank probabilities showed that AL was most likely to be associated with the greatest forward flexion (Table 2).
Postoperative pain
Information on the VAS score was provided in 3 studies involving 1,294 patients, including AB, OL, and OB. When the analysis was conducted using a random-effects model, no significant difference was observed in the VAS score among AB, OL, and OB (Figure 8). Similarly, no significant difference in the VAS score was observed among AB, OL, and OB in the league table analysis using a random-effects model (Table 1). The rank probabilities demonstrated that OB had the highest probability of achieving the lowest VAS score (Table 2).
Complications
A total of 18 studies comprising 1,902 patients were included in the analysis. Complications were assessed across 4 surgical approaches: AB, OB, OL, and AL. Direct comparisons were made between OL and each of the other 3 surgical methods, with specific direct comparisons existing between OL and AB. The network plot indicated a larger node and a thicker connecting line between AB and OL, suggesting that more studies directly compared these 2 interventions and that the sample size for these comparisons was relatively larger (Figure 2D).
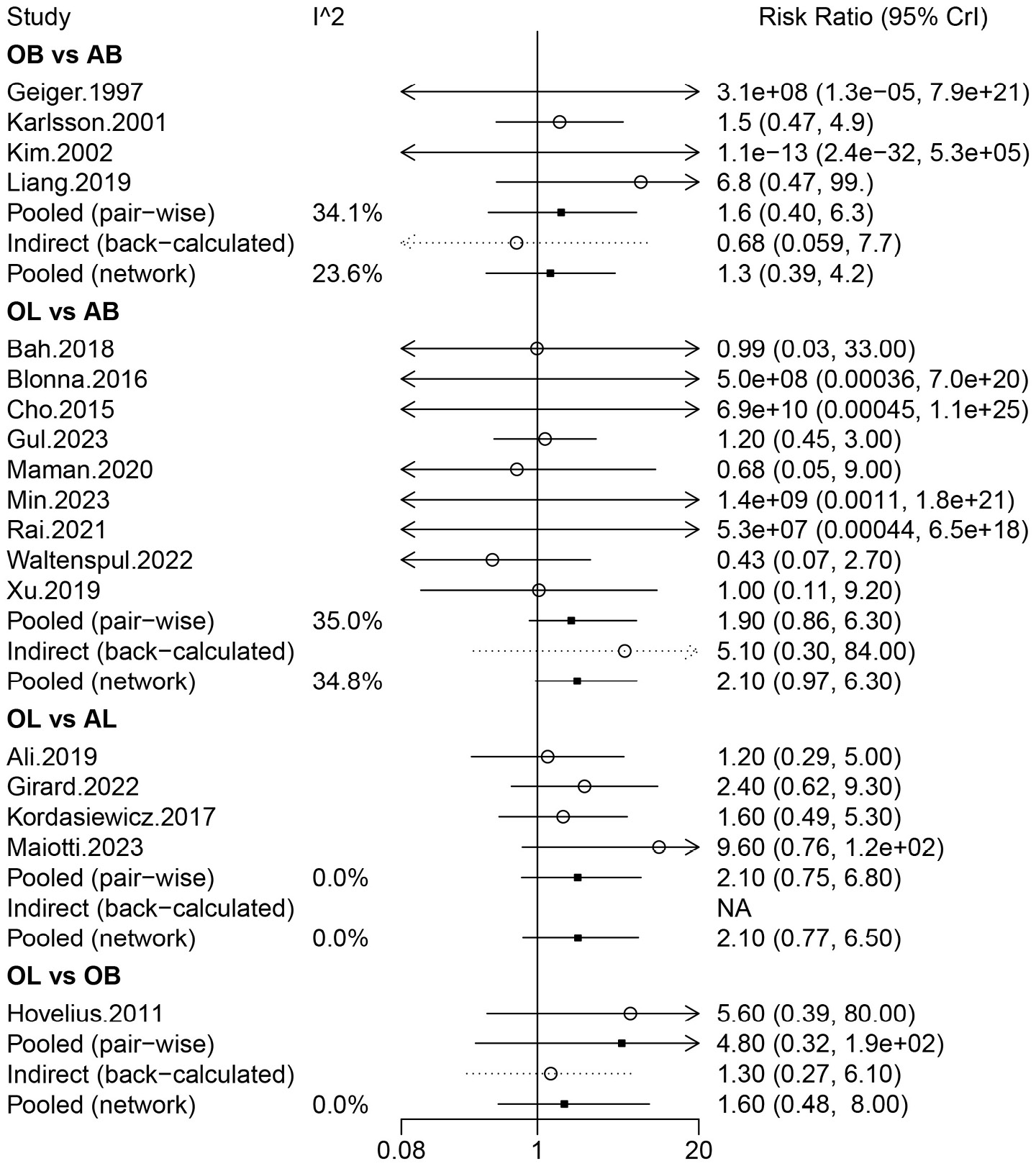
No significant difference in complications was observed among the 4 methods in the forest plot analysis using a random-effects model (Figure 9). Similarly, no significant difference in complications was observed among the 4 techniques in the league table analysis using a random-effects model (Table 1). The rank probabilities demonstrated that OL had the highest probability of complications (Table 2). The funnel plots for publication bias assessment are shown in Supplementary Fig. 1.
Discussion
In this network meta-analysis, a comparison of the pooled data regarding the clinical efficacy of the OB, AB, OL, and AL procedures for shoulder dislocation and instability was conducted. Open Latarjet was most likely to have the lowest risk of recurrent instability and re-dislocation. Although not statistically significant, OL was most likely to have the lowest risk of apprehension and the highest SSV score. However, OL had the highest probability of complications. In addition, with regard to postoperative pain, the OL procedure was not necessarily associated with a significantly lower VAS score, indicating that it might not be the best option in terms of postoperative pain management.
The results of the network meta-analysis indicate that the OL procedure may offer superior outcomes in terms of shoulder stability and function for patients with shoulder dislocation and instability. However, the analysis also highlights a critical area for improvement: the management of postoperative pain following the OL procedure. In a meta-analysis conducted by Wang et al.,29 a comparative analysis of OB compared with AB repairs for Bankart lesions revealed that while the OB method provided superior shoulder stability, it was accompanied by limitations in shoulder mobility.
Conversely, the AB technique, although less invasive, was associated with better preservation of motion. In another meta-analysis, a comprehensive evaluation was conducted to compare the clinical efficacy, as well as the rates of postoperative revisions and complications, between OL and AL. The study found no significant differences in the majority of the assessed outcomes between the 2 procedures. However, the AL approach was associated with a lower score on the Western Ontario Shoulder Instability Index, indicating better shoulder function or less instability. Additionally, the AL procedure exhibited a higher revision rate, suggesting a greater likelihood of patients requiring additional surgeries.28
Nonetheless, the efficacy of OB, AB, OL, and AL has not been compared in patients with shoulder dislocation and instability in existing studies. To facilitate understanding and decision-making among the 4 methods when considering therapeutic options for shoulder dislocation, the present network meta-analysis focused on shoulder stability, functional outcomes, and postoperative pain following these procedures.
In terms of shoulder stability, the OL procedure was indicated to have the highest likelihood of being the most effective repair option. In a meta-analysis encompassing 795 shoulders, the OL procedure demonstrated a significantly lower risk of recurrence compared with AB repair.67 As reported by Rollick et al.,68 the estimated re-dislocation rate was notably higher at 15.1% for patients who had undergone AB, whereas it was considerably lower at 2.7% for those who had OL procedure. In terms of functional outcomes, OL may also demonstrate a relative advantage.
According to the findings by Bliven et al.,69 a higher percentage of patients who underwent the Latarjet procedure were able to successfully return to work, sports, and throwing activities compared with those who had Bankart repair. Consistently, a study has shown that the Latarjet procedure for anterior shoulder instability leads to excellent long-term functional outcomes and a high rate of return to sports.70 However, patients might experience unsatisfactory postoperative pain outcomes and complications following the OL procedure, which could be attributed to the larger incision associated with the surgery. Arthroscopic surgery generally offers the benefits of a lower nonunion rate and the potential for quicker recovery due to its minimally invasive nature. The drawbacks of the AL procedure are also evident. It requires longer operative time and a longer learning curve for surgeons.71
Analysis of the learning curve indicated that the initial cohort experienced longer operative times and higher complication rates compared with the subsequent group, potentially accounting for the increased incidence of revision surgeries required for the AL procedure.72 Only surgeons expected to perform the AL procedure at high volume should consider adopting this technique.73, 74 Additionally, it has been shown that the direct costs associated with the AL procedure are significantly higher, amounting to approximately double the cost of the OL procedure, with figures of 2,335 EUR for AL compared with 1,040 EUR for OL.75
Several factors may contribute to the effectiveness of the OL procedure. The OL procedure provides a dual stabilizing effect by increasing the anterior glenoid width and creating a sling effect with the conjoint tendon, which helps stabilize the joint.76 Correct graft positioning is critical to the success of the OL procedure. It has been suggested that OL might offer better control over graft placement, which could lead to improved long-term outcomes.77
Limitations of the study
Several limitations of this study should be acknowledged. First, there was a lack of literature on some outcomes, which may have affected the accuracy of the results. Second, this study focused on the general population, and further research was not conducted in specific populations such as athletes and males or females.51 In addition, some of the included studies were cohort studies; therefore, change scores were used for continuous data, and studies that provided only endpoint data were not included in this analysis. Third, including only English-language literature may result in language bias. Fourth, there are differences between primary operations and re-operations, and these differences could potentially influence the outcomes of interest. However, due to limitations in the included literature, such as the lack of detailed data on re-operations, we were unable to conduct a separate analysis for re-operations. This precludes definitive conclusions regarding the comparative effectiveness of the 4 surgical approaches for shoulder dislocation and instability in the context of re-operations. Fifth, we acknowledge that glenoid bone loss, a significant factor affecting shoulder joint stability and surgical outcomes, was not controlled for in our screening process. Although glenoid bone loss was included as a variable in Supplementary Table 1, the substantial amount of missing data across the reviewed studies prevented us from accounting for it in our analysis. This limitation may restrict the accuracy of our comparisons among different surgical approaches.
Conclusions
Open Latarjet was most likely to be the optimal procedure for shoulder stability, and patients undergoing OL may have non-inferior functional outcomes. Although the OL procedure may not be associated with significantly lower VAS pain scores, it was associated with a higher rate of complications. Therefore, it is imperative to implement appropriate measures to mitigate postoperative pain and manage complications following OL procedure.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.15872256. The package contains the following files:
Supplementary Table 1. Characteristics of the included studies.
Supplementary Table 2. League table of different procedures for various outcomes in patients with primary operation analyzed by the random-effect model.
Supplementary Fig. 1. A. Publication bias assessed by the funnel plot for recurrent instability; B. Publication bias assessed by the funnel plot for re-dislocation; C. Publication bias assessed by the funnel plot for apprehension; D. Publication bias assessed by the funnel plot for Rowe; E. Publication bias assessed by the funnel plot for complications.
Use of AI and AI-assisted technologies
Not applicable.