















Abstract
Background. In the contemporary era, acquiring online information has become a prevalent practice. As with any affliction, individuals are inclined to investigate the potential therapeutic avenues for erectile dysfunction (ED) on the internet.
Objectives. To evaluate the quality, comprehensibility and informative content of YouTube videos on penile prosthesis implantation, with a focus on videos produced by healthcare professionals, and to address the videos according to the class of physician producing the video.
Materials and methods. A search for “penile prosthesis” was conducted on YouTube using a censored network to ensure privacy and prevent bias. The first 100 relevant videos uploaded in the last decade were analyzed. They were categorized by source (academicians, government or private hospital physicians, and non-physicians) and assessed for quality using the modified Quality Criteria for Consumer Health Information (DISCERN) scale, Global Quality Scale (GQS) and a newly developed Total Informative Score based on the European Association of Urology Patient Information Forms. The Kruskal–Wallis H test, Kendall’s tau correlation test and Spearman’s test were used for statistical analysis.
Results. Of the videos analyzed, 87% provided informative content, with the majority (51%) uploaded by academic sources. The median duration time was 185 s (111–397). The average modified DISCERN score was low (median: 2, Q1–Q3: 2–3), indicating generally inadequate quality, with 54% rated as poor. No statistical significance occurred between GQS scores for the videos published by the upload source. Videos by government hospital physicians scored the highest in quality measures, while non-physician videos garnered more views and likes. The Patient Education Materials Assessment Tool (PEMAT) understandability and actionability scores showed that videos from healthcare professionals had higher understandability (70%) than those from other sources.
Conclusions. The overall quality of YouTube videos on penile prostheses is low, despite most being informative. Videos created by physicians are more reliable and easier to understand. Implementing stricter guidelines for content creators and promoting public awareness initiatives are recommended to improve patient access to high-quality information.
Key words: YouTube, penile prosthesis, modified DISCERN, PEMAT
Background
Erectile dysfunction (ED) is a common condition that affects approx. 52% of men aged 40–70.1 Currently, the first-line treatment for ED is oral phosphodiesterase type 5 inhibitors. Patients with refractory ED or those who do not wish to pursue medical therapy may require alternative treatment options. Intracavernous injections, vacuum erection devices and penile prostheses are commonly used alternative treatment methods. Penile prostheses provide a surgical solution that can restore erectile function in refractory cases, regardless of etiology.2 Designed to facilitate penile rigidity, these devices help users regain sexual function. There are 2 main types of prostheses: malleable (flexible) and inflatable. Overall, penile prosthesis implantation is associated with high patient satisfaction rates. Obtaining informed consent is essential to ensure that patients are aware of potential risks, which include mechanical failure, infection, pain, changes in penile size and sensation, and possible injury to nearby structures such as the urethra, bladder or intestines. Discrepancies between preoperative expectations and postoperative outcomes may also lead to psychological distress.3 For this reason, surgeons provide patients with comprehensive information about potential complications, ensuring that they are aware of the risks before surgery. However, this detailed explanation often requires further clarification or guidance for surgical candidates. Obtaining thorough guidance from every physician on such a specific topic can be challenging, and this need becomes even more difficult to meet when considering the additional factors of privacy and embarrassment.
Studies have shown that patients with sexual health concerns often prefer online sources to get information about their illness due to feelings of shame.4 The ease of resources available on the internet has enabled people to seek solutions to their health-related questions and concerns on different platforms, as in many other areas. This tendency, which has increased across all fields during the pandemic, is particularly pronounced in sexual health, even outside of a pandemic context. The underlying factor may be a sense of shame that prevents individuals from seeking medical attention, even outside the pandemic context. YouTube, a video-based social media platform accessed by approx. 30 million users per day, has become a potential source of medical information.5 Healthcare professionals, institutions and patients share health-related videos for various purposes, including education, advertising and information.
The Internet has greatly simplified access to information. However, it is concerning that anyone with an Internet connection and a suitable device can upload videos that are accessible to patients worldwide.
Many previous studies across various specialties have shown that the information presented in YouTube videos is often of poor quality and may contain inaccurate or misleading content.6, 7, 8, 9, 10 Several studies have also highlighted the risks associated with the spread of erroneous medical information across different disciplines. This includes urological conditions such as ED, premature ejaculation, Peyronie’s disease, hypospadias, urinary tract stones, bladder pain syndrome, and the use of phosphodiesterase type 5 inhibitors.11, 12, 13, 14, 15, 16, 17 The findings of these studies point to a broader issue regarding the quality of medical content available online. Specifically, the analysis of these videos demonstrates the potential to mislead patients or present incomplete information, which may influence their decision-making. While such material may be useful for general education, it becomes problematic when patients rely on it to understand surgical procedures and make treatment decisions. This is particularly important in the context of surgical treatments such as penile prosthesis implantation, where preoperative information is critical. In these cases, the need for accurate, high-quality resources becomes even more pronounced. Inadequate information may lead to misunderstandings about the procedure, its risks and expected outcomes, ultimately influencing patients’ decisions and expectations. A 2022 study of YouTube videos related to penile prostheses echoed these concerns, concluding that the quality of information was insufficient and lacked comprehensive medical guidance.18 The study also showed that many of the videos did not meet the standards required for informed decision-making.
Objectives
Given this background, our study aimed to address an existing gap in the literature by evaluating YouTube videos related to penile prosthesis implantation. Specifically, we categorized the videos based on their producers – medical professionals compared to non-professionals – and assessed the adequacy, quality and reliability of the information presented. This research seeks to provide a more nuanced analysis of the reliability of online medical content, recognizing that patient decision-making is critical to health outcomes. The findings of this study are intended to contribute to the growing body of literature on the quality of medical information available on digital platforms and to offer guidance on how patients can access more reliable resources.
Materials and methods
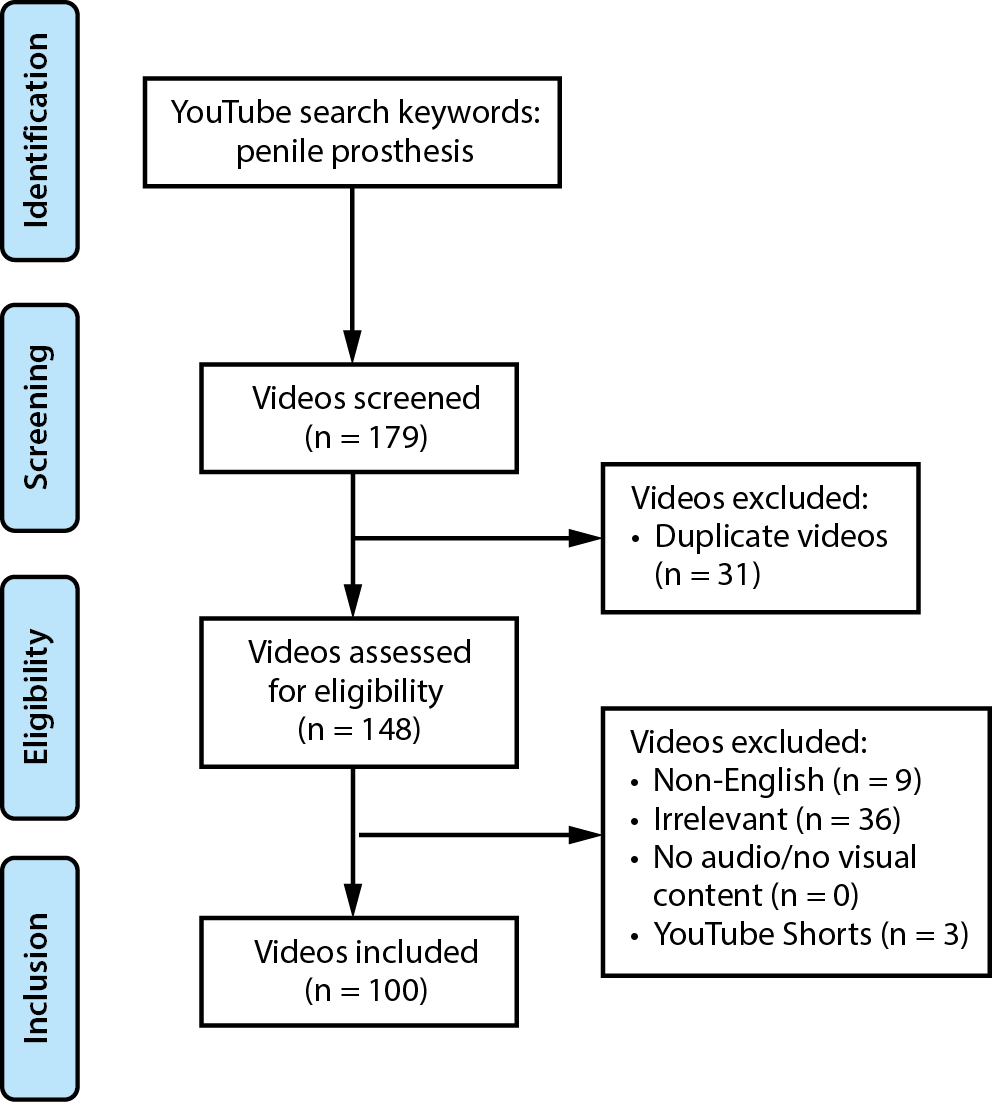
The study did not involve human or animal subjects, and access to YouTube videos is publicly available; therefore, no ethics committee approval was required. On June 1, 2024, we searched the term “penile prosthesis” on YouTube using a virtual private network (VPN)-based proxy server located in the USA. To avoid single-user bias, the search was conducted with all personal accounts logged out, in incognito mode, and repeated twice. Search history and cookies were cleared before the procedure. For relevance, only videos from the last 10 years were included in the analysis. No time restrictions were otherwise applied to the videos included in the study. Videos that were fully or partially duplicated, not in English, irrelevant, or classified as YouTube Shorts were excluded. The elimination process is illustrated in a flowchart (Figure 1). The first 100 videos meeting these criteria were included in the study. To minimize bias, 3 physicians with varying levels of experience independently evaluated the content of each video. The upload date, duration, view count, number of likes and dislikes, and number of comments were recorded. Video sources were classified according to the provider of the information or the surgical content into the following categories: academic, government hospital physicians, private hospital physicians, and non-physicians. The quality and content of the videos included in the study were evaluated using the modified Quality Criteria for Consumer Health Information (DISCERN) scale and the Global Quality Scale (GQS). The modified DISCERN scale, which assesses objectivity, reliability and understandability, consists of 5 questions. Each “yes” answer receives 1 point and each “no” answer receives 0 points, yielding a maximum score of 5 and a minimum score of 0. The GQS, which measures the overall quality of information obtained from online sources, is also scored on a scale from 1 to 5.19 The Patient Education Materials Assessment Tool (PEMAT) was developed to evaluate and compare the understandability and actionability of patient education materials. According to the PEMAT, videos are considered understandable or actionable if they achieve a score ≥70%.20
Furthermore, based on the European Association of Urology (EAU) Patient Information Forms for Penile Prosthesis, we developed a more specific tool addressing the key topics that patients should be informed about regarding penile prostheses. This tool was termed the “Total Informative Score” (TIS). The informational content of the videos was evaluated using 6 questions (Table 1) and rated on a scale of 1 (insufficient information), 2 (partially sufficient information) or 3 (sufficient information) for each item. Accordingly, the minimum score is 6, indicating that the video contains no meaningful medical information, while the maximum score is 12, indicating that the video provides comprehensive coverage of penile prosthesis surgery.
Statistical analyses
IBM SPSS v. 27 (IBM Corp., Armonk, USA) was used for statistical analysis. Continuous variables were described as median and minimum–maximum (min–max) or as median and interquartile range (IQR, Q1–Q3), as appropriate. Categorical variables were expressed as numbers and percentages. In the univariate analyses, the Kruskal–Wallis H test for nonparametric variables was used to examine whether the type of video producer was associated with video quality, as measured with PEMAT understandability and actionability, TIS, the modified DISCERN score, and the GQS score. As the p-value for the Kruskal–Wallis test was below 0.05, post hoc analysis was performed using Dunn’s test with Bonferroni adjustment. The p-values obtained from Dunn’s test, with adjusted values reported for each significant pairwise comparison, are presented. Because the data were not normally distributed, correlations were assessed using Kendall’s tau correlation test. This test was used to evaluate potential associations between video characteristics and quality scores. A p < 0.05 within a 95% confidence interval (95% CI) was considered statistically significant.
Results
These videos were posted between 2014 and 2024. A descriptive analysis revealed a median duration of 175 s (range: 44–2,154 s). The number of views showed considerable variability, with a median of 5,850 and a range from 51 to 2,600,000. Similarly, the median number of likes was 34 (range: 0–7,100), while the number of comments per video had a median of 4 (range: 0–689). The median time since upload was 25.5 months, with a minimum of 1 month and a maximum of 120 months. There were no dislikes recorded for any of the videos. The quality and content of the videos, assessed using standardized scoring tools, were as follows: the PEMAT scores showed a median understandability score of 70 (range: 60–80) and a median actionability score of 70 (range: 50–80).
The median modified DISCERN score of the videos included in the study was 2 (range: 2–3). Twenty-four videos (24%) received a score of 1, 33 videos (33%) received a score of 2, 22 videos (22%) received a score of 3, 20 videos (20%) received a score of 4, and only 1 video (1%) received the maximum score of 5. Overall, these findings indicate low to moderate quality. Similarly, the median GQS score was 2 (range: 2–3). In this evaluation, 16 videos (16%) received a score of 1, 38 (38%) received a score of 2, 23 (23%) received a score of 3, 22 (22%) received a score of 4, and only 1 video (1%) received the maximum score of 5. This distribution likewise demonstrates that the majority of the videos were of low to moderate quality.
Of the videos included in the study, 87 (87%) were informative videos based on the EAU Patient Information Form, 10 (10%) contained surgical procedures and 3 (3%) included both types of content. Most videos were uploaded by academicians (51%), while 13 (13%) were uploaded by government hospital physicians, 30 (30%) by private hospital physicians, and 6 (6%) by non-physicians. General information regarding the videos is summarized in Table 2. The median PEMAT understandability scores were 70% (60–80%), 85% (77.5–90%), 70% (50–81.25%), and 70% (62.5–81.25%) for academicians, government hospital physicians, private hospital physicians, and non-physicians, respectively.
The median PEMAT actionability scores were 65% (50–75%), 80% (75–85%), 62.5% (50–80%) and 65% (42.5–74%) for academicians, government hospital physicians, private hospital physicians, and non-physicians, respectively. The Kruskal–Wallis test showed a significant difference in PEMAT understandability scores among the groups (H(3, 100) = 10.37, p = 0.016). However, no statistically significant difference was found in PEMAT actionability scores between the groups (H(3, 100) = 7.27, p = 0.064) (Table 3, Figure 2A,B).
The median GQS scores were 2 (2–3), 3 (2.5–4), 2 (2–4), and 2 (1–2.5) for academicians, government hospital physicians, private hospital physicians, and non-physicians, respectively. The median modified DISCERN scores were 2 (2–3), 3 (3–4), 2 (1–4), and 1 (1–2.5) for these same groups. There was no statistically significant difference in GQS scores based on the source of upload (H(3, 100) = 5.66, p = 0.129) (Table 3, Figure 3A). However, a statistically significant difference was observed in modified DISCERN scores among the groups (H(3, 100) = 9.73, p = 0.021) (Table 3, Figure 3B).
The median TIS values were 13 (12–16), 13 (10–15.5), 13 (11–16.25), and 9 (8–13.25) for academicians, government hospital physicians, private hospital physicians, and non-physicians, respectively. There was no statistically significant difference in total information scores based on the source of upload (H(3, 100) = 6.09, p = 0.021) (Table 3, Figure 3C). According to Dunn’s test with Bonferroni correction, there was a statistically significant difference in PEMAT understandability scores between government hospital physicians and both academicians (p = 0.012) and private hospital physicians (p = 0.021).
Government hospital physicians had higher PEMAT understandability scores. For the modified DISCERN scores, a statistically significant difference was found between government hospital physicians and non-physicians (p = 0.026), with higher scores observed among government hospital physicians. There was a statistically significant difference in the number of video views between academicians and both government hospital physicians and non-physicians (p = 0.033 and p = 0.008, respectively), with videos uploaded by academicians receiving fewer views. In addition, the number of comments on videos uploaded by academicians was significantly lower than that on videos uploaded by government hospital physicians (p = 0.038).
There was also a statistically significant difference in the number of likes between videos uploaded by academicians and those uploaded by government hospital physicians and non-physicians (p = 0.016 and p = 0.049, respectively), with academicians’ videos receiving fewer likes). Table 4 presents only the statistically significant pairwise comparisons following Bonferroni correction (p < 0.05) for clarity; the full list of pairwise comparisons is available in Supplementary Table 1. Video duration, number of views, comments, and likes showed statistically significant correlations with TIS, GQS, modified DISCERN, and PEMAT scores. No statistically significant relationship was observed between video upload date and any of the quality measures – including GQS, modified DISCERN, PEMAT understandability, PEMAT actionability, and TIS. These findings indicate that the quality of YouTube videos on this topic has not changed appreciably over time (Table 5).
Discussion
Penile prosthesis surgery is an effective treatment option with high satisfaction rates and a low complication profile for patients with ED who do not benefit from medical therapies.21 However, complications that require revision surgery, as well as adverse outcomes such as penile shortening or decreased penile sensation, may negatively affect patients’ quality of life and overall satisfaction. In addition, the additional costs associated with revision procedures may result in financial burden for patients.
Therefore, it is essential that patients are fully and accurately informed before the procedure. The widespread use of the Internet and the integration of digital applications into daily life have led individuals to rely on platforms such as YouTube as sources of free medical information. Given the feelings of shame often experienced by patients with sexual health concerns, it is understandable that many prefer to seek information through these platforms. Numerous videos related to penile prosthesis implantation are available on YouTube.12, 22 A previous study evaluating the informational content of these videos reported more than 8,000 videos on the topic.18 In our study, the identification of an even larger number of videos during screening suggests that public interest in this subject continues to grow. Based on previous studies evaluating the quality of YouTube videos, the first 100 videos were assessed.12, 18, 23 Unlike the study conducted by Capace et al., videos published by healthcare providers were further categorized into subgroups, revealing that academicians produced the majority of the content (51%).
The quality of the videos was assessed using the GQS, which showed that 54% were of inadequate quality (GQS scores of 1 or 2). The median modified DISCERN score was 2, with more than half of the videos (57%) receiving a score of 2 or lower. These findings indicate that the videos were generally of low to moderate quality. This is concerning, as individuals without medical training may struggle to distinguish reliable information from inaccurate or misleading content. Incorrect or incomplete information can confuse patients and complicate clinical counseling. In the subgroup analysis, videos published by physicians working in government hospitals had higher GQS scores and were the most reliable, with the highest median modified DISCERN scores. In contrast, videos uploaded by non-physician users ranked highest in popularity, receiving the most likes, comments and views. These findings align with previous studies indicating that many individuals who watch health-related videos online do not consider the source of the content.24
However, it is well recognized that accurate information requires the use of appropriate and reliable sources. In this context, guideline-based search tools may help patients obtain correct information when accessing medical content online. Interestingly, and contrary to expectations, the subgroup analysis revealed that videos published by academicians had relatively low GQS and modified DISCERN scores. Although the reason for this finding is not fully clear, it may be related to the inclusion of overly detailed or highly technical information, which could lead to viewer fatigue and reduced comprehension.
This study evaluated YouTube videos on penile prosthesis implantation by categorizing them according to their source and assessing their quality using validated tools such as DISCERN, GQS and PEMAT. It also introduced the TIS for a more targeted assessment. The informational content of the videos was further evaluated using an additional tool based on the EAU Penile Prosthesis Patient Information Form, focusing on 6 key topics. The analysis showed that videos published by non-healthcare professionals had very low informational content.
Furthermore, the relatively low informational scores of videos published by healthcare professionals suggest that comprehensive, high-quality knowledge on this topic may not be readily accessible online. Although most videos were classified as informative, their overall quality remained low, with government hospital physicians producing the most reliable content. These findings underscore the need for clearer guidelines and greater public awareness regarding reliable sources of medical information. In addition to the quality and content of the videos, it is essential that the information shared is both understandable and actionable. Educational videos must strike an effective balance between content quality and usability, as well-informed patients are better equipped to make appropriate decisions about their care.
According to Shoemaker et al., PEMAT understandability and actionability scores above 70% are considered sufficiently understandable or actionable.20 In our study, PEMAT understandability scores for videos from all sources were at or above this threshold. However, videos published by physicians working in government hospitals had significantly higher understandability scores than those from other sources. The median PEMAT actionability score was 70 (60–80). Notably, only the videos published by physicians working in government hospitals achieved scores indicating that the information was easy to apply. These findings suggest that videos produced by doctors in public hospitals are generally intended to promote public awareness, and our results confirm that these videos successfully fulfill that purpose.
This study highlights the importance of high-quality online medical content for patients considering penile prosthesis implantation. The findings demonstrate that low-quality videos may lead to confusion and negatively influence patient decision-making. Government hospital physicians produced the most reliable content, which underscores the need for more patient-friendly educational materials from all sources. Enhancing the quality of online content has the potential to improve patient education, satisfaction and ultimately clinical outcomes.
Limitations
Despite the systematic evaluation of YouTube videos using validated assessment tools, this study has several limitations. First, we restricted our analysis to English-language videos, meaning that a substantial portion of content related to penile prostheses remains unexamined. The search procedure may also introduce bias, as the findings are based on a single search term. Another limitation is that only the first 100 YouTube videos identified using the selected keywords were analyzed. It is well established that most users do not look beyond the first 1 or 2 pages of search results, which may limit the representativeness of the sample. YouTube search results vary among users and are influenced by prior search behavior, geographic location and other algorithm-driven factors. To minimize these effects, we logged out of all personal accounts and used a VPN-based proxy to modify our location before conducting the search. This study also acknowledges the potential for selection bias due to the involvement of a single researcher and the influence of YouTube’s algorithm; therefore, 3 researchers independently assessed the videos, and a new YouTube account was created for the search process. Future studies should include multiple researchers or employ automated video-sorting techniques to improve the objectivity and reliability of video selection. Evidence from previous studies suggests that such methods can effectively reduce bias and enhance the quality of selected content.
Conclusions
The quality of YouTube content related to penile prostheses is generally low. Videos published by physicians in hospital settings tend to provide higher informational content and are more understandable and accessible for patients. To improve this widely used information source, implementing guidelines for content creators and ensuring the availability of accurate, reliable medical information are essential.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.17019527. The package contains the following files:
Supplementary Table 1. Pairwise comparisons of video characteristics by source (Bonferroni-adjusted p-values).
Data Availability Statement
The datasets supporting the findings of the current study are openly available in Zenodo at https://doi.org/10.5281/zenodo.14253817.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.
.jpg)
.jpg)