















Abstract
Background. Since older patients are at high risk of hypotension and hypoxia during anesthesia, it is crucial to choose safe sedatives.
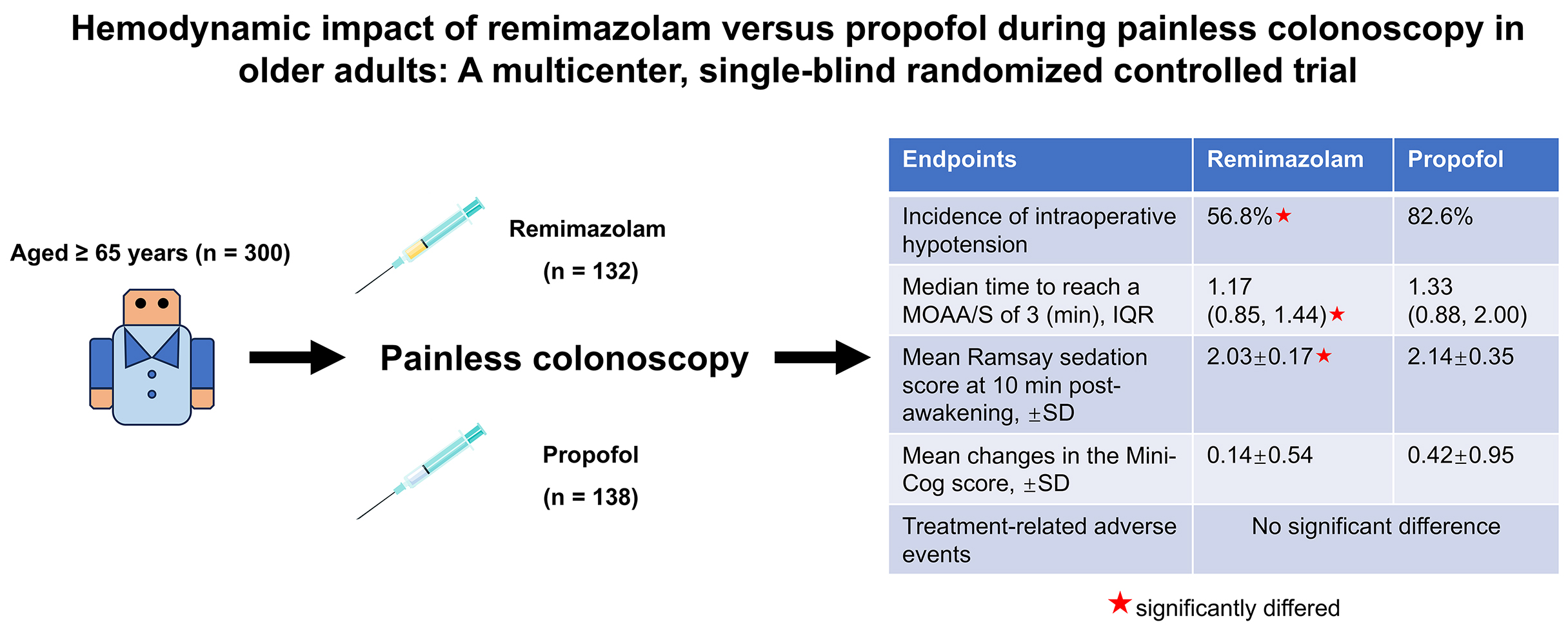
Objectives. To compare the efficacy and safety of remimazolam with propofol in elderly patients undergoing endoscopic procedures.
Materials and methods. This multicenter, single-blind, randomized study included patients aged ≥65 years (American Society of Anesthesiologists (ASA) physical status I–III) who were randomized in a 1:1 ratio to receive either remimazolam (0.1–0.2 mg/kg) or propofol (0.3–0.5 mg/kg). The primary endpoint was the rate of occurrence of hypotensive events. Secondary endpoints included time to patient unresponsiveness and time to awakening (defined as a Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score ≤3 and ≥4), time to leaving the operating room, cognitive function assessment (using the Mini-Cog test), and additional parameters.
Results. A total of 300 patients aged ≥65 years were enrolled. Patients who received remimazolam (n = 132) experienced a significantly lower incidence of intraoperative hypotension compared with those treated with propofol (n = 138) (56.8% vs 82.6%, p < 0.001). The median time to reach a MOAA/S score of 3 was shorter in the remimazolam group than in the propofol group (1.17 min [interquartile range (IQR): 0.85–1.44] vs 1.33 min [IQR: 0.88–2.00], p = 0.041). At 10 min post-awakening, the median Ramsay sedation score was lower in the remimazolam group (2.03 ±0.17 vs 2.14 ±0.35, p = 0.001). Tukey’s post hoc analysis showed a significant decline in cognitive scores before and after anesthesia in the propofol group (p = 0.002), whereas no significant change was observed in the remimazolam group (p = 0.658). There was no significant difference in treatment-related adverse events (AEs) between the 2 groups.
Conclusions. Remimazolam significantly reduced the incidence of intraoperative hypotension during colonoscopy, providing a safer sedative option for elderly patients and supporting its use as a preferred agent in this population.
Key words: anesthesia, hemodynamics, remimazolam, propofol, colonoscopy
Background
In recent years, with an aging population, the incidence of gastrointestinal diseases has risen significantly,1 and according to reports from China, 4,824,700 new cancer cases and 2,574,200 new cancer deaths occurred in 2022.2 Particularly for older people, the risk of developing peptic ulcers or cancer is increased,3 and performing regular preventive examinations is crucial for the early detection of gastrointestinal diseases and for maintaining the health of older patients.4
In older adults (aged ≥65 years) undergoing endoscopy, the use of sedatives may induce hypotension, affecting their health. Therefore, in 2006, the American Society of Gastrointestinal Endoscopy (ASGE) issued guidelines specifically addressing sedative use in older patients and recommended the use of anesthetics such as propofol, etomidate and midazolam supplemented with analgesics such as fentanyl, sufentanil and remifentanil5 during gastrointestinal endoscopy. Although propofol induces rapid sedation and quick recovery, it has a narrow therapeutic index,6 which leads to doses resulting in intraoperative hypotension rates of up to 26%, particularly in elderly patients.7, 8, 9 Additionally, propofol may induce other dose- and injection rate-dependent side effects, including respiratory depression, hypoxemia and cardiovascular events. Consequently, the U.S. Food and Drug Administration (FDA) strongly advises that propofol administration be performed exclusively by professionals trained in general anesthesia.10 Benzodiazepines are commonly used sedatives and generally have little impact on the circulatory system, but their slow clearance rate may lead to accumulation, prolonging the need for mechanical ventilation.11, 12
Remimazolam has a faster neuropsychiatric recovery compared to midazolam. It may become a new option for sedation during bronchoscopy.13 Compared with propofol, the benzodiazepine remimazolam is more hemodynamically stable for painless gastroenteroscopy in elderly patients, producing a significantly lower incidence of adverse events (AEs), such as injection pain and respiratory depression, and significantly shorter times to wake up and leave the operating room.14
In addition, remimazolam has a high clearance rate, a smaller volume of distribution at steady state, and a shorter elimination half-life.15 Remimazolam, which binds strongly to proteins in the body, is extensively metabolized by liver carboxylesterases16 and subsequently excreted through the kidneys,17 with an elimination time of 45 min. Additionally, the sedative effect of remimazolam is short-acting, making it suitable for inducing sedation in time-limited medical procedures, including upper gastrointestinal endoscopy and colonoscopy.18 Therefore, remimazolam offers the benefits of a faster recovery time from sedation and a lower risk of hypotension during maintenance anesthesia.19 The FDA approved remimazolam in July 2020 for the induction and maintenance of sedation in adults undergoing procedures lasting ≤30 min, and remimazolam is also used to ensure painless colonoscopy for patients aged ≥65 years.
Objectives
The present study aimed to compare the efficacy and safety of remimazolam and propofol for sedating older Chinese individuals undergoing endoscopic procedures in a large-scale study that particularly focused on hypotension, and to further determine the specific time period during which remimazolam affects blood pressure (BP).
Materials and methods
This article is presented in accordance with the Consolidated Standards of Reporting Trials (CONSORT) reporting checklist.
Ethics approval
The study protocol and all amendments were approved by the Ethics Committees of all participating hospitals: West China Hospital, Sichuan University (approval No. 2021-Review-No. 719, issued on August 9, 2021); Luzhou People’s Hospital (approval No. 2023002); the First Affiliated Hospital of Chengdu Medical College (approval No. 2022CYFYIRB-BA-Ju110); West China Fourth Hospital, Sichuan University (approval No. HXSY-EC-2022056); the Third Hospital of Mianyang (approval No. 2022010); the Medical Center Hospital of Qionglai City (approval No. 2022045); The Second People’s Hospital of Neijiang and Meishan People’s Hospital completed ethical review through a record-filing process based on the approval of the leading center and adopted the same ethics approval number (approval No. 2021-Review-No. 719). This study was registered with the Chinese Clinical Trial Registry (registration No. ChiCTR2200063066; date of registration: August 30, 2022) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all enrolled patients.
Study design
This was a single-blind, randomized, parallel-group study conducted in 8 medical centers across China. A random coding table was generated using the central stratified block randomization method with IBM SPSS v. 25.0 statistical software (IBM Corp., Armonk, USA), based on the planned total number of cases in each group. Patients at each center were randomly assigned to either a remimazolam group or a propofol group, with drugs being distributed sequentially by each center according to the random number assigned at the time of dispensing.
Because remimazolam is a clear or slightly yellow solution when reconstituted in saline, whereas propofol is a white emulsion, these medications can be easily distinguished. Therefore, a single-blind design was employed in this trial, with only the patients being blinded.
Patients
Between August 2022 and June 2023, 300 patients aged ≥65 years with American Society of Anesthesiologists (ASA) physical status (ASA-PS) I–III who were scheduled to undergo colonoscopy were enrolled. Inclusion criteria were body mass index (BMI) 18–30 kg/m2, respiratory rate (RR) 10–24 breaths/min and pulse oximetry (SpO2) ≥95% on room air. In addition, systolic blood pressure (SBP) ≥90 mm Hg, diastolic blood pressure (DBP) ≥60 mm Hg and a heart rate (HR) of 60–100 bpm were required during screening and at baseline.
Exclusion criteria were: contraindications to deep sedation or general anesthesia; a history of sedation/anesthesia incidents; known allergy to eggs, soy products, opioids and their antagonists, propofol, or remimazolam; contraindications to propofol, benzodiazepines, opioids, and their antagonists; a history of serious hepatic, renal, gastrointestinal, hematological, neurological, or metabolic disorders that, in the opinion of the investigator, may have increased the risk of sedation/anesthesia complications and made participation in the trial inappropriate; risk of respiratory-compromising factors identified during the screening period, including a history of asthma, wheezing or sleep apnea syndrome; a history or a family history of malignant hyperthermia; a history of failed extubation and the presence of a difficult airway assessed by the investigator, or assessed as difficult extubation (Modified Mallampati Score of grade IV).
In addition, patients who had participated in a clinical trial with any drug within 1 month prior to screening or had received opioids or sedative/anesthetic drugs in the 3 days prior to the visit were excluded. Furthermore, patients with any other factor that, in the opinion of the investigator, made participation in the clinical study inadvisable were also excluded.
After screening for eligibility criteria, patients who signed informed consent forms were randomly assigned, in the order of enrollment, to a remimazolam group or a propofol group.
Treatment procedures
Before any procedure, patients fasted for 8 h, and no drinking water was permitted for 2 h. When a patient arrived in the examination room, a monitor was connected to record their breathing circulation, and bispectral index (BIS) data. A nasal cannula or breathing mask was applied with an oxygen flow rate of 5 L/min to preoxygenate the patient for 3 min. A nasal cannula was then used to provide oxygen and maintain oxygen delivery until the end of the procedure.
Sufentanil (0.1 μg/kg over 30 s) was administered, followed by 0.1–0.2 mg/kg remimazolam (Yichang Humanwell Pharmaceutical Co., Ltd., Yichang, China) or 0.3–0.5 mg/kg propofol (AstraZeneca S.p.A., Caponago, Italy). According to clinical guidelines, which emphasize that physiological changes in older patients warrant lower initial doses of sedatives than those used in typical adults and a slower titration rate to allow full evaluation of each dose’s effects, close monitoring of patient response is essential.20 The procedure was initiated when the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score was ≤3. The depth of intraoperative sedation was maintained at MOAA/S scores ≤3 and a BIS value between 60 and 80.
Propofol (0.3 mg/kg) or remimazolam (0.05 mg/kg) was administered if patient body movements or eye opening occurred during the procedure, if the patient’s BP fluctuated significantly, or if their facial expression indicated pain, at which point 0.05 µg/kg sufentanil was administered. If the patient developed respiratory depression, measures were taken to provide mechanical ventilation. If the patient’s HR was <50 bpm, 0.5 mg of atropine was administered intravenously. Ephedrine 3 mg or 0.1 mg of metaraminol was administered intravenously to raise BP if the patient’s BP had dropped below 30% of the baseline BP or if the SBP was <80 mm Hg. After colonoscopy, patients were taken to the postanesthesia care unit (PACU), where their postanesthetic clinical signs were carefully monitored, documented and analyzed.
Observations during interventions
Vital signs, including BP, HR, end-tidal carbon dioxide partial pressure, SpO2, RR, and BIS, were monitored continuously throughout the trial. The Ramsay sedation scores of patients were recorded at several key time points: before drug administration, immediately after awakening, 5 min post-awakening, 10 min post-awakening, and upon discharge from the PACU. The Ramsay sedation scale classifies sedation into 6 levels: a score of 1 indicates anxiety, restlessness or agitation; 2 reflects a cooperative, oriented and calm state; 3 indicates a response only to verbal commands; 4 represents a response to loud auditory stimuli or a light glabellar tap; 5 signifies a response to strong physical stimuli, such as ear lobe tugging or eyebrow pressure; and 6 indicates no response, signifying deep sleep. All sedation assessments were performed by trained clinicians at these specified intervals to ensure the accuracy and consistency of the sedation level.21 Cognitive function was assessed before anesthesia and when the patient was awake using the Mini-Cog assessment.22
Primary endpoint
The incidence of intraoperative hypotension was the main outcome measure. Hypotension was defined as either an SBP ≤ 80 mm Hg or a decrease in SBP > 20% from baseline between the beginning of medication administration and the patient becoming fully alert.
Secondary endpoints
The secondary endpoints included: the time from anesthesia induction to patient unresponsiveness (defined as a MOAA/S score ≤3); total examination time; awakening time (defined as a MOAA/S score of ≥4); the time from awakening to leaving the operating room (considered as leaving the PACU when the Aldrete score was >9); whether the patient showed somatic movements and the number of these movements; the total dose of propofol or remimazolam administered; the number of times additional doses of propofol or remimazolam were administered during the procedure; and the doses of these drugs. Safety indicators included: hypotension; hypoxemia (SpO2 < 90%, with or without nasal oxygen catheter placement); airway obstruction; respiratory depression (RR < 8 breaths/min); apnea; bradycardia (HR < 60 bpm); tachycardia (HR > 100 bpm); intraoperative awareness; the number and doses of intraoperative vasopressors (ephedrine and metaraminol) administered; the number and doses of intraoperative atropine administered; satisfaction of the anesthesiologist and endoscopist (satisfaction scores measured using the visual analogue scale (VAS) method); and cognitive function assessment using a Mini-Cog before and after anesthesia. Postoperative comfort indicators were collected through telephone follow-ups with patients 24 h and 48 h after colonoscopy. These included: nausea; vomiting; vertigo (defined as a feeling of spinning, movement, or trembling of the peripheral environment or of the patient); and dizziness (defined as a feeling of lightheadedness, unsteadiness or unpleasant sensations). Furthermore, incidences of headache, drowsiness, fatigue, abdominal distension, abdominal pain, and eructation were recorded, as well as sore throat and jaw discomfort (anesthetic drugs may suppress the gag reflex, increasing reflux aspiration risk and causing throat discomfort). Sore throat and jaw discomfort may indicate airway management or positioning issues, whereas eructation relates to intestinal gas and recovery care.
Sample size calculation
For sample size calculations, the hypotension occurrence rate was used as the primary outcome measure. According to phase 3 clinical trial results, the incidence of intraoperative hypotension when remimazolam was used for colonoscopy was 10.6%, and 29.2% when propofol was used.23 Assuming that when propofol was administered to older patients, the incidence of hypotension was similar to that found in adult patients (30%), and that remimazolam reduced the incidence of hypotension by 20%, a 3% cut-off for superiority was used, assuming α = 0.025 and β = 0.2, resulting in a sample size of 82 patients per group according to the superiority test sample size formula. Considering a drop-out rate of 20%, the study required a total sample size of 206 patients, with 103 patients assigned to each drug group.
Statistical analyses
Statistical analyses were performed using SPSS v. 25.0 (IBM Corp.). All tests were two-tailed, with a significance level of p ≤ 0.05. Statistical methods were based on data characteristics: continuous variables are reported as median (1st quartile (Q1), 3rd quartile (Q3)) and were compared using the Wilcoxon test for non-normally distributed data, or as the mean ± standard deviation (SD) and analyzed using the t-test. Ordinal variables were compared using the Wilcoxon rank-sum test. Categorical variables were analyzed using the χ2 test or Fisher’s exact test, when appropriate. For repeated-measures data, repeated-measures analysis of variance was used, with degrees of freedom (ε) adjusted based on Mauchly’s sphericity test. Generalized estimating equations (GEE), with a logit link for binary outcomes, were applied to analyze differences in the incidence of hypotension between the 2 groups, along with post hoc comparisons at different time points.
Results
A total of 300 patients were enrolled, of whom 30 were excluded due to insufficient data (18 in the remimazolam group and 12 in the propofol group). Ultimately, 270 patients were included in the full analysis set, with 132 in the remimazolam group and 138 in the propofol group (Figure 1).
Most patients in the 2 groups had an ASA-PS score of II (87.7–88.6%), and there were no discernible differences in vital signs, BIS, cognitive functions, or other demographic baseline or clinical characteristics between the 2 groups (Table 1).
Primary outcome
In patients who received remimazolam, the incidence of intraoperative hypotension (75/132, 56.8%) was significantly lower compared with the propofol group (114/138, 82.6%) (p < 0.001) (Figure 2A). Additionally, from Figure 2B, it is evident that the incidence of intraoperative hypotensive events at 1, 3 and 5 min after remimazolam administration appeared to be lower than in the propofol group. There was no significant difference in the incidence of hypotensive events between the 2 groups from 10 min after sedation induction until awakening (Figure 2B).
The differences in hypotension incidence between the 2 groups were further analyzed using GEE with a logit link for binary outcomes. It was found that only the incidence of hypotension at 1 min after remimazolam administration was significantly lower than in the propofol group, while no significant differences were observed at other time points. The GEE analysis also indicated that both group and time effects were significantly different (p = 0.003 and p < 0.001, respectively). However, their interaction was not significant, suggesting no difference in the temporal trend of hypotension incidence between the 2 groups (Table 2).
Secondary outcomes
Effects of anesthesia
The median dosages of administered remimazolam and propofol were 11.6 mg (Q1–Q3: 10.0–13.1 mg) and 93.0 mg (Q1–Q3: 65.0–120.0 mg), respectively. The median time from the induction of anesthesia to patient unresponsiveness was shorter in the remimazolam group than in the propofol group (1.17 min (Q1–Q3: 0.85–1.44 min) vs 1.33 min (Q1–Q3: 0.88–2.00 min), p = 0.041). The total examination time was not significantly different between the 2 groups. Additionally, the median time to awakening and the median time from awakening to leaving the operating room were not significantly different between patients who received remimazolam and those who received propofol (1.78 min (Q1–Q3: 0.59–4.09 min) vs 1.31 min (Q1–Q3: 0.50–3.75 min), p = 0.736; 14.50 min (Q1–Q3: 10.03–29.48 min) vs 15.52 min (Q1–Q3: 12.30–26.67 min), p = 0.242, respectively). The dosages of additional drugs in the 2 groups were not significantly different (59.8% vs 62.3%, p = 0.677; Table 3).
Regarding the Ramsay sedation score, there were no significant differences at the pre-anesthetic, awake, 5 min after awakening, and PACU-departure time points. An exception was observed at 10 min after awakening (remimazolam 2.03 ±0.17 vs propofol 2.14 ±0.35, p = 0.001; Table 3).
Patient cognitive function and satisfaction of patient and physicians’ evaluation
The changes in the Mini-Cog score after sedation in the remimazolam group were significantly lower than those in the propofol group (0.14 ±0.54 and 0.42 ±0.95, p = 0.001) (Table 4). However, neither the group effect nor the interaction between group and time was statistically significant, as revealed by further GEE analysis, indicating that there was no significant difference in cognitive scores or their changes between the 2 groups. However, Tukey’s post hoc tests showed that the difference in cognitive scores before and after anesthesia was statistically significant in the propofol group (p = 0.002). No significant difference was observed in the remimazolam group (p = 0.658). The VAS scores for patient and endoscopist satisfaction were not significantly different. The VAS score for anesthesiologist satisfaction was higher in the remimazolam group than in the propofol group (9.74 ±0.66 vs 9.55 ±0.81, p = 0.033) (Table 4).
Safety and comfort indicators
Safety indicators primarily refer to treatment-related AEs (TRAEs) that occurred throughout the sedation process, including hypoxemia, airway obstruction, respiratory depression, apnea, bradycardia, tachycardia, and intraoperative awareness. Additionally, AEs included the incidence of vasopressor and atropine use during sedation. As shown in Figure 3A, there were no significant differences in the incidence of AEs between the 2 groups.
Additionally, comfort indicators related to TRAEs occurring within 24 h after the end of anesthesia in the remimazolam group included nausea, vomiting, dizziness, headache, drowsiness, fatigue, abdominal distension, abdominal pain, and eructation. In the propofol group, the TRAEs were mainly nausea, vomiting, vertigo, drowsiness, fatigue, abdominal distension, and abdominal pain. However, the comfort indicators related to the incidence of TRAEs within 48 h after the end of anesthesia were significantly lower in both groups than in the 24-h group. In the remimazolam group, the main TRAEs were drowsiness, fatigue, abdominal distension, and abdominal pain, while in the propofol group, the main TRAEs were only abdominal distension and abdominal pain (Figure 3B,C).
Discussion
The results of the present study revealed that the incidence of hypotension was lower in the remimazolam group than in the propofol group, achieving the primary endpoint. Remimazolam may be considered a suitable alternative to propofol for elderly patients,9, 24, 25 given that propofol anesthesia often causes hypotension during surgery. In addition, remimazolam had a faster onset of sedation, but the sedation scores at 10 min post-awakening were higher in the remimazolam group. Therefore, the anesthesiologists expressed greater satisfaction when using remimazolam. Previously, it had been observed that remimazolam reached its peak blood concentration within 1 min, with an average retention time in the body only 1/7 that of midazolam.26 In a phase 3 clinical trial by Rex et al., participants undergoing colonoscopy were randomly assigned to receive 5.0 mg of remimazolam. After assessing sedation effects, additional top-up injections of 2.5 mg remimazolam were administered at intervals of no more than 2 min to maintain sedation.
Remimazolam significantly improved the overall procedural success rate to 0.896 (95% confidence interval (95% CI): 0.851–0.942).27 Compared to the control group, patients treated with remimazolam showed better recovery of neuropsychiatric functions, and the incidence of hypotension was significantly reduced even in high-risk colonoscopy patients (ASA PS III/IV) after initial remimazolam doses ranging from 2.5 to 5.0 mg. If sufficient sedation was not achieved, up to 4 additional doses of 1.25 to 2.5 mg of remimazolam were administered.28 In another phase III trial by Wang et al., patients aged 18–65 years who underwent colonoscopies received an intravenous injection of 7 mg remimazolam or 1.5 mg/kg propofol to induce sedation. The time from the start of medication to an MOAA/S score ≤3 was significantly longer in the patients who received remimazolam (1.45 min) than in patients given propofol (1.24 min) (p < 0.001).23 However, in the present study, the opposite result was found. The remimazolam group reached an MOAA/S score of 3 in a significantly shorter median time than the propofol group (1.17 min (0.85–1.44 min) vs 1.33 min (0.88–2.00 min), p = 0.041). This discrepancy may be attributed to the lower propofol dosage used for older patients in our study. In addition, the incidence of hypotension in the phase III trial conducted by Wang et al. was greater than in the present study (remimazolam group: 56.8%, propofol group: 82.6%). This was likely due to greater hemodynamic fluctuations in older patients. Furthermore, hypotension was defined not only as an SBP reduction to ≤80 mm Hg but also as an SBP falling by >20% from baseline. The present study also revealed that changes in cognitive function, as measured using the Mini-Cog score, were less pronounced in the remimazolam group than in the propofol group. However, a direct comparison before and after sedation showed a significant decline in cognitive function in the propofol group but no significant change in the remimazolam group. More rigorous statistical analyses, including group effects and interaction analyses, found no significant difference in the overall pattern of cognitive changes between the 2 groups. Therefore, these results suggest that propofol may contribute to cognitive decline but do not confirm that remimazolam provides better cognitive protection. In addition, the Ramsay sedation scores at 10 min post-awakening were superior in the remimazolam group. Although the exact reasons for these findings are unclear, they indirectly demonstrate the safety of remimazolam for geriatric colonoscopy. The sedation efficacy and safety of remimazolam in elderly patients aged ≥65 years are consistent with the findings of a previously published meta-analysis,14 which had limitations due to the small sample sizes in the included studies. The present study fills that gap and further confirms the efficacy and safety of remimazolam in elderly patients. Since the use of remimazolam in elderly patients is not yet widespread, its potential as an alternative to propofol holds significant clinical relevance. In recent years, several methods have been proposed to alleviate the pain and discomfort associated with the use of local anesthesia. A systematic review has highlighted that phentolamine, as a local anesthetic reversal agent, significantly shortens the duration of anesthesia in both children and adults. By accelerating the clearance of anesthetic drugs, phentolamine helps mitigate the side effects associated with prolonged anesthesia.29 Therefore, when using remimazolam or propofol for injection-induced sedation, it may be beneficial to incorporate additional methods to shorten the anesthesia duration, reducing the risk of adverse reactions in patients.
Limitations
In summary, the current investigation and other clinical studies have verified that remimazolam is as safe and effective as propofol for colonoscopy sedation. However, these results should be interpreted with caution. There is currently a lack of studies on the quality of recovery and the effects of remimazolam on cognitive function. In addition, pharmacological data on equivalent doses of remimazolam compared to other sedatives are also missing. Notably, the doses of remimazolam and comparator drugs used in clinical trials varied. In elderly patients, the lack of antihypertensive intervention may affect blood flow fluctuations during examinations. Another limitation is the lack of pre-procedure fluid optimization, such as a detailed fluid status assessment through inferior vena cava evaluation30 or the passive leg raising test.31
Conclusion
Remimazolam sedation offers both effective sedation and a favorable safety profile, making it a valuable alternative for use in clinical practice. Due to its minimal impact on hemodynamics, remimazolam has strong potential as a sedative of choice for individuals undergoing colonoscopy, particularly elderly patients in China.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.15437576. The package contains the following files:
Supplementary Table 1. Change in hypotension incidence over time. The data are presented as numbers and percentages (p-values: post hoc GEE analysis).
Supplementary Table 2. GLM procedure – least squares mean (LSMEAN). Adjustment for multiple comparisons: Tukey–Kramer.
Supplementary Table 3. GLM procedure – least squares mean of the effect “time*group”. Pr > |t| (for H0): LSMean(i) = LSMean(j). Dependent variable: score.
Supplementary Table 4. Test of normality. Normality tests of measurement values were performed using Shapiro–Wilk tests. When p > 0.05, the data followed a normal distribution; when p < 0.05, the data did not follow a normal distribution. Parametric tests were applied when p > 0.05.
Supplementary Table 5. Homogenity of variances. Homogeneity tests of measurement values were performed with Levene’s tests. Since the p-value was above 0.05, it was considered homogeneous.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research, the supporting data are not available.
Use of AI and AI-assisted technologies
Not applicable.
Consent for publication
Not applicable.
.jpg)
.jpg)
.jpg)