Abstract
Background. Many hospitals worldwide implement nurse-led sedation protocols to prevent both under- and over-sedation and to enhance comfort and safety for mechanically ventilated patients in intensive care units (ICUs); however, definitive conclusions regarding their effectiveness remain limited.
Objectives. To assess the efficacy of nurse-led sedation protocols on clinical outcomes in mechanically ventilated adults within ICUs.
Materials and methods. A systematic search was conducted across 4 electronic databases – PubMed, Embase, Scopus, and the Cochrane Library – to identify relevant studies published in peer-reviewed journals. The standard mean difference (SMD) and risk ratio (RR), along with their corresponding 95% confidence intervals (95% CIs), were calculated. Heterogeneity among studies was assessed using the Cochran’s Q test and I2 statistic, with significance determined by the appropriate p-value. All statistical analyses were performed using Review Manager (RevMan) v. 5.4.
Results. This meta-analysis of 10 randomized controlled trials (RCTs; n = 1,151 patients) indicates that a nurse-led sedation protocol is significantly more effective than usual care in reducing ICU mortality (RR = 0.34 (95% CI: 0.25 to 0.45); I2 = 38%, p < 0.001), duration of mechanical ventilation (SMD = −1.94 (95% CI: −2.16 to −1.72); I2 = 73%, p < 0.001), length of hospital stay (SMD = −1.70 (95% CI: −1.80 to −1.59); I2 = 79%, p < 0.001), length of ICU stay (SMD = −1.58 (95% CI: −1.76 to −1.40); I2 = 66%, p < 0.001), and incidence of delirium (RR = 0.47 (95% CI: 0.39 to 0.57); I2 = 15%, p < 0.87).
Conclusions. Compared to usual care, nurse-led sedation protocol can improve ICU mortality and other clinical outcomes in mechanically ventilated ICU patients safely and effectively.
Keywords: ICU mortality, intensive care unit (ICU), meta-analysis, mechanical ventilation, nurse-led sedation protocols
Background
Critically ill patients on mechanical ventilation in intensive care units (ICUs) often require sedation to alleviate pain, anxiety, and agitation. Inadequate sedation can increase sympathetic activity, lead to cardiovascular instability, and cause respiratory complications that compromise patient outcomes.1, 2 Conversely, inadequate sedation can culminate in delirium, unplanned extubation, and prolonged mechanical ventilation, resulting in lower morbidity, mortality, and healthcare expenditures.3, 4 The Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption (PADIS) guidelines advocate for the routine utilization of analgesia and sedation in ICUs to minimize discomfort, promote patient-centered care, and diminish the risk of adverse events (AEs).5 Despite the critical importance of sedation management in ICUs, ongoing debate surrounds the most effective approach. Traditional physician-led sedation protocols may not consistently achieve optimal sedation levels, potentially resulting in AEs and extended ICU stays. Contemporary controversies in the literature encompass debates on optimal sedation strategies, including physician-led vs nurse-led protocols, ideal depth of sedation, benefits and risks of daily sedation interruptions vs continuous sedation, and concerns regarding the potential long-term effects of sedation on cognitive and psychological outcomes.
In recent years, nurse-led sedation protocols have emerged as a promising alternative, possessing the potential to enhance patient outcomes, reduce healthcare expenditures, and augment patient satisfaction.6, 7 These protocols involve the utilization of standardized sedation scales, such as the Richmond Agitation-Sedation Scale (RASS) or the Sedation-Agitation Scale (SAS), to assess patient sedation levels and adjust intravenous drip rates accordingly.8, 9 Many studies10, 11, 12, 13, 14 have indicated that nurse-led sedation management, guided by specific goals and flowcharts, surpasses traditional methods.
The implementation of a nurse-driven sedation protocol has yielded advantageous results, notably by abbreviating the duration of mechanical ventilation, reducing the length of stay in the ICU, and minimizing the period of continuous sedation. Furthermore, this approach has enhanced the frequency of spontaneous awakening trials (SATs), ultimately contributing to improved patient outcomes, including diminished morbidity, mortality, and healthcare expenditures. Magner et al. observed in their research that a nurse-led programmed sedation scheme can augment the effectiveness of sedation while concurrently decreasing the occurrence of delirium.15 In a comparable study, Qi et al. noted that the adoption of a sedation protocol by nursing staff can enhance outcomes, resulting in decreased mortality rates and a reduction in sedation-related AEs among mechanically ventilated patients in ICUs, when contrasted with standard physician-led care.16
However, Aitken et al. observed no notable disparities in hospital mortality, self-extubation rates, ICU length of stay, and duration of mechanical ventilation when comparing patients subjected to protocol-directed sedation with those undergoing non-protocol-directed sedation.17 Consequently, the evidence substantiating the efficacy of nurse-led sedation protocols remains inconclusive, as preceding systematic reviews and meta-analyses have been characterized by limited sample sizes and inconsistent results. Moreover, recent investigations have yielded divergent findings, underscoring the necessity for a thorough and contemporary examination of the existing literature.
Objectives
This study seeks to assess the impact of ICU nurse-led sedation protocols on various patient outcomes, such as mechanical ventilation duration, length of stay in the ICU, mortality rates, and AEs related to sedation, in comparison to the traditional physician-led care approach. Our objective was to conduct a thorough assessment of the effectiveness and safety of nurse-led sedation protocols in mechanically ventilated adults in ICUs. This was achieved through a systematic review and meta-analysis of 10 relevant randomized controlled trials (RCTs),18, 19, 20, 21, 22, 23, 24, 25, 26, 27 selected according to established inclusion and exclusion criteria, focusing on the impact of nurse-led sedation protocols on various clinical outcomes in ICUs. By synthesizing the available evidence, this study aims to provide a comprehensive and up-to-date evaluation of the efficacy and safety of nurse-led sedation protocols, comparing outcomes with traditional physician-led care, and informing evidence-based practice and future research in sedation management for critically ill patients.
Materials and methods
Eligibility criteria
This study included randomized controlled trials (RCTs) that provided comparative data on the clinical effectiveness of nurse-led sedation protocols for mechanically ventilated adults in ICUs. No restrictions were applied regarding language or publication year. Studies were included if they met the following criteria: 1) RCT design; 2) involved adult ICU patients requiring mechanical ventilation; 3) participants aged 18 years or older; 4) reported outcomes such as ICU mortality, length of hospital stay, duration of mechanical ventilation, incidence of self-extubation, and occurrence of delirium; and 5) full-text articles with sufficient data for constructing a 2 × 2 table.
The following studies were excluded from the evaluation process: 1) studies other than RCTs (e.g., case series, case-control studies, and cohort studies); 2) expert opinions, animal studies, experimental trials, and descriptive reports; 3) studies that did not include ICU patients requiring mechanical ventilation; and 4) bibliographic sources that were anecdotal, methodologically weak, or based solely on expert opinion.
Information sources
This study adhered to the guidelines set forth by AMSTAR (Assessing the Methodological Quality of Systematic Reviews)28 and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses),29 and it has been registered in PROSPERO (CRD42025631472). Employing established inclusion and exclusion criteria for the selection of studies, we undertook a systematic review of relevant RCTs that assessed the efficacy and safety of nurse-led sedation protocols in mechanically ventilated adults within ICUs. An extensive search of prominent databases, including Embase, PubMed, Scopus, and Cochrane CENTRAL, was conducted by utilizing specific keywords and search terms, with the search extending up to September 30, 2024.
Search strategy
A comprehensive literature search was conducted across multiple databases to identify relevant studies. The search terms included: “Nurse-led sedation protocols”, “Sedation”, “Mechanical ventilation”, “Intensive care unit”, “ICU”, “Physician-led usual care”, “Non-protocol-directed sedation”, “Duration of mechanical ventilation”, “Length of stay in ICU”, “Length of hospital stay”, “ICU mortality”, “Incidence of self-extubation”, “Incidence of delirium”, “Systematic review”, “Systematic review and meta-analysis”, “Meta-analysis”, “RCT”, and “Randomized controlled trial”. No language restrictions were applied. Studies published in languages other than English were included when sufficient data could be reliably extracted, and included only RCTs involving mechanically ventilated adults in ICUs, with nurse-led sedation protocols compared against physician-led or non-protocol-directed usual care. The PICO framework guided the selection process: “P” denoted the patient population (mechanically ventilated adults in ICUs), “I” the intervention (nurse-led sedation protocols), “C” the comparator (usual physician-led care or non-protocol-directed sedation), and “O” the outcomes assessed – ICU mortality, length of hospital stay, duration of mechanical ventilation, incidence of self-extubation, and incidence of delirium.30
Selection process
Two reviewers (J.L. and H.L.) conducted an independent evaluation of article titles, abstracts, and full texts to discern potential RCTs. When necessary, a senior researcher (X.H.) was engaged to facilitate the resolution of any discrepancies between the 2 reviewers via discourse. Table 1 provides a comprehensive outline of the search strategy employed.
Data collection process
Two researchers (J.L. and H.L.) independently extracted the demographic information and event data from the selected RCTs using a predefined data collection form. The extracted information included study identification and year, country of origin, sample size, nurse-to-patient ratio, classification of ICU environments, participants’ age (mean ± standard deviation (SD)), gender distribution (percentage of male and female patients), intervention specifics, control conditions, and reported outcomes. When data were incomplete or unclear, the original study authors were contacted for clarification or additional details.
Risk of bias assessment of included studies
A standardized questionnaire was utilized to assess the potential for bias in the included RCTs. Two authors (X.H. and J.Z.) conducted independent evaluations of bias potential in individual studies employing the Cochrane risk-of-bias instrument v. 2.31 This instrument consisted of 5 components: bias resulting from discrepancies in intended interventions, bias originating from randomization, bias due to inadequate outcome data, bias during the assessment of outcomes, and bias in the selection of reported outcomes. Two researchers (X.H. and J.Z.) conducted an evaluation to analyze the possibility of bias. Another reviewer took on the position of an adjudicator to address any outstanding disputes. We assessed potential bias and categorized it as “uncertain risk”, “high risk”, or “low risk”. Publication bias and small-study effects were measured through a comparison-adjusted funnel plot32 and applied Begg’s test33 using MedCalc v. 20.218 (MedCalc Software Ltd., Ostend, Belgium)34 to assess the presence of publication bias and small-study effects, with statistical significance determined at a threshold of p < 0.05.
Effect measures
The Review Manager (RevMan) v. 5.435 (Nordic Cochrane Centre, Copenhagen, Denmark) was employed to assess and scrutinize the impact of various continuous and dichotomous outcomes. The standard mean differences (SMDs), risk ratios (RRs), and 95% confidence intervals (95% CIs) were calculated for each study to evaluate the binary outcomes.36
Statistical analyses
The DerSimonian–Laird method method was employed to compute RR using a 2 × 2 contingency table containing event data. Forest plots were utilized to visually assess the impact of various outcome measures. A fixed-effect model was applied when the relative treatment effect was assumed to be consistent across all included studies, while a random-effects model was used when some variability between studies was anticipated. To evaluate heterogeneity among studies, statistical parameters such as the I2 statistic, χ2 test value, Z-test statistic, and p-value were used. A result was considered statistically significant when p < 0.05. Subgroup analyses were conducted to evaluate the effectiveness of nurse-led sedation protocols in mechanically ventilated ICU patients, focusing on outcomes including the duration of mechanical ventilation, ICU mortality, length of ICU stay, and overall hospital stay. Additionally, RRs were calculated to determine the risk of AEs associated with the nurse-led sedation protocols.37, 38, 39, 40, 41, 42, 43, 44, 45
Results
Study selection outcomes
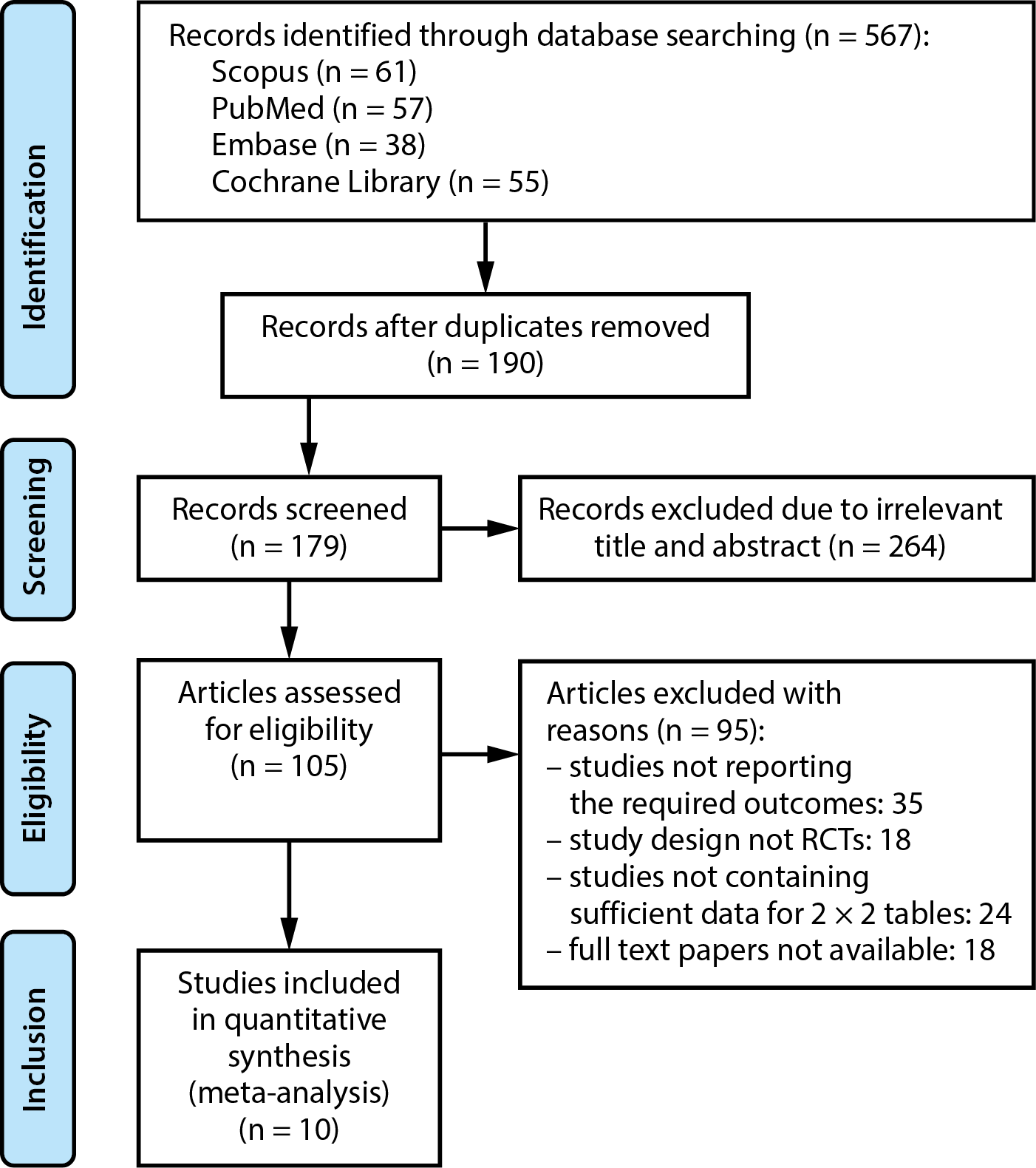
Examination of multiple databases was conducted for this investigation, resulting in the identification of 211 papers that fulfilled the inclusion criteria specified in the PICO framework. A total of 190 publications were selected for examination, while 21 papers were removed owing to redundancy. After additional screening, the titles and those articles abstracts of 74 publications were deemed irrelevant and were therefore eliminated. The remaining 105 articles underwent further assessment. However, 95 studies were considered ineligible and were consequently excluded following the application of the inclusion-exclusion criteria. This was primarily due to the lack of full-text papers, inadequate data to create 2 × 2 tables, or the absence of necessary outcomes. This meta-analysis included 10 RCTs that met the established inclusion-exclusion criteria, as illustrated in the study flow diagram per PRISMA standards (Figure 1). This investigation involves a total of 1,151 mechanically ventilated ICU patients that are above the age of 18. Table 2 presents a succinct characteristics and participant demographics of the RCTs included and analyzed in this meta-analysis. Additionally, event data for the 2 × 2 table were acquired from the participating RCTs to do a meta-analysis. Supplementary Table 1 presents the assessment based on the AMSTAR-2 criteria.46
Evaluation of potential bias in the selected RCTs
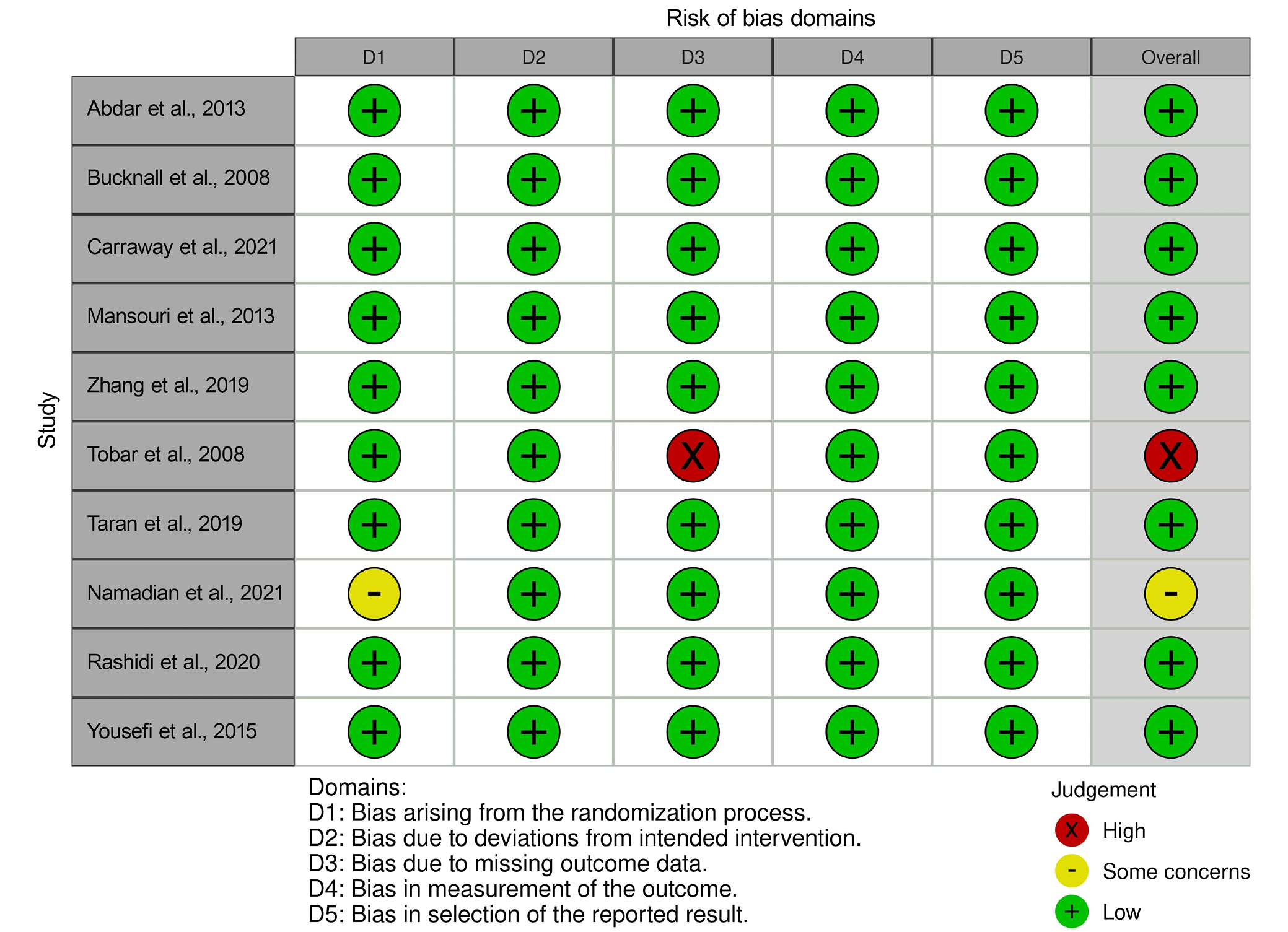
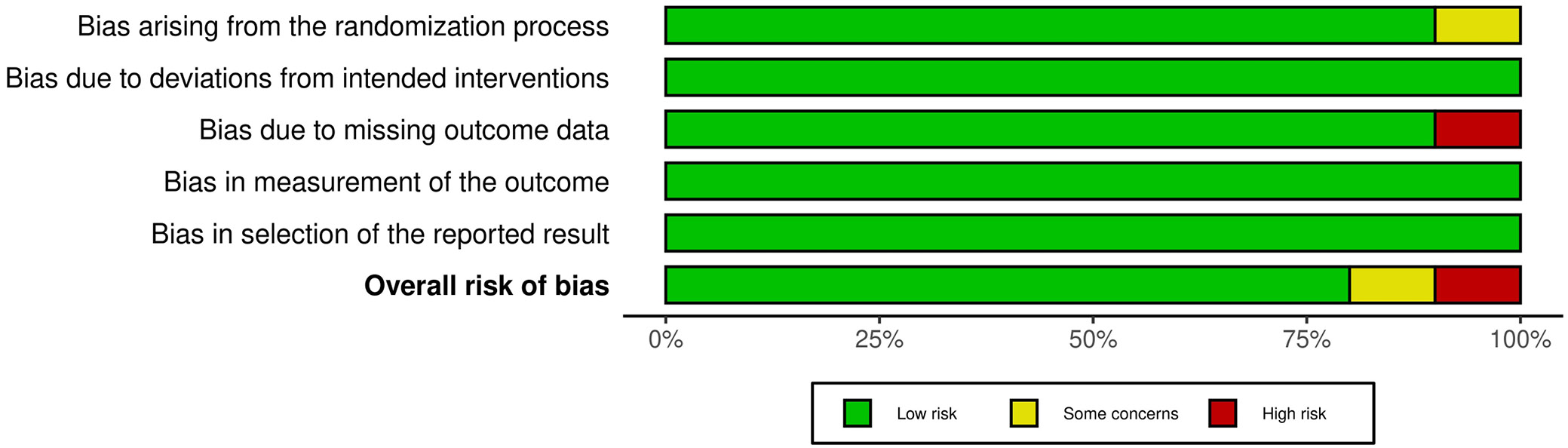
An extensive evaluation of bias risk was undertaken to assess the quality of the studies included in the analysis. The findings of this evaluation, employing a predetermined questionnaire, are delineated in Table 3 for each of the 10 RCTs incorporated in the meta-analysis. The results of this evaluation, as depicted in the traffic light plot (Figure 2) and summary plot (Figure 3), suggest a minimal probability of bias among the studies analyzed. Notably, 8 out of the 10 RCTs were assessed to possess a low risk of bias, indicating a commendable level of methodological rigor. Nevertheless, 1 RCT (Namadian and Taran25) exhibited a moderate risk of bias, chiefly attributable to issues surrounding the randomization process. Furthermore, another RCT (Tobar et al.23) was recognized as exhibiting a significant risk of bias, chiefly attributable to concerns regarding absent outcome data.
This study assessed the effectiveness and safety of nurse-led sedation protocols for mechanically ventilated adults in the ICU, drawing from 10 RCTs. The analysis of the clinical outcomes within the subgroups produced the results discussed below.
Analysis of subgroups to assess mortality rates in the ICU
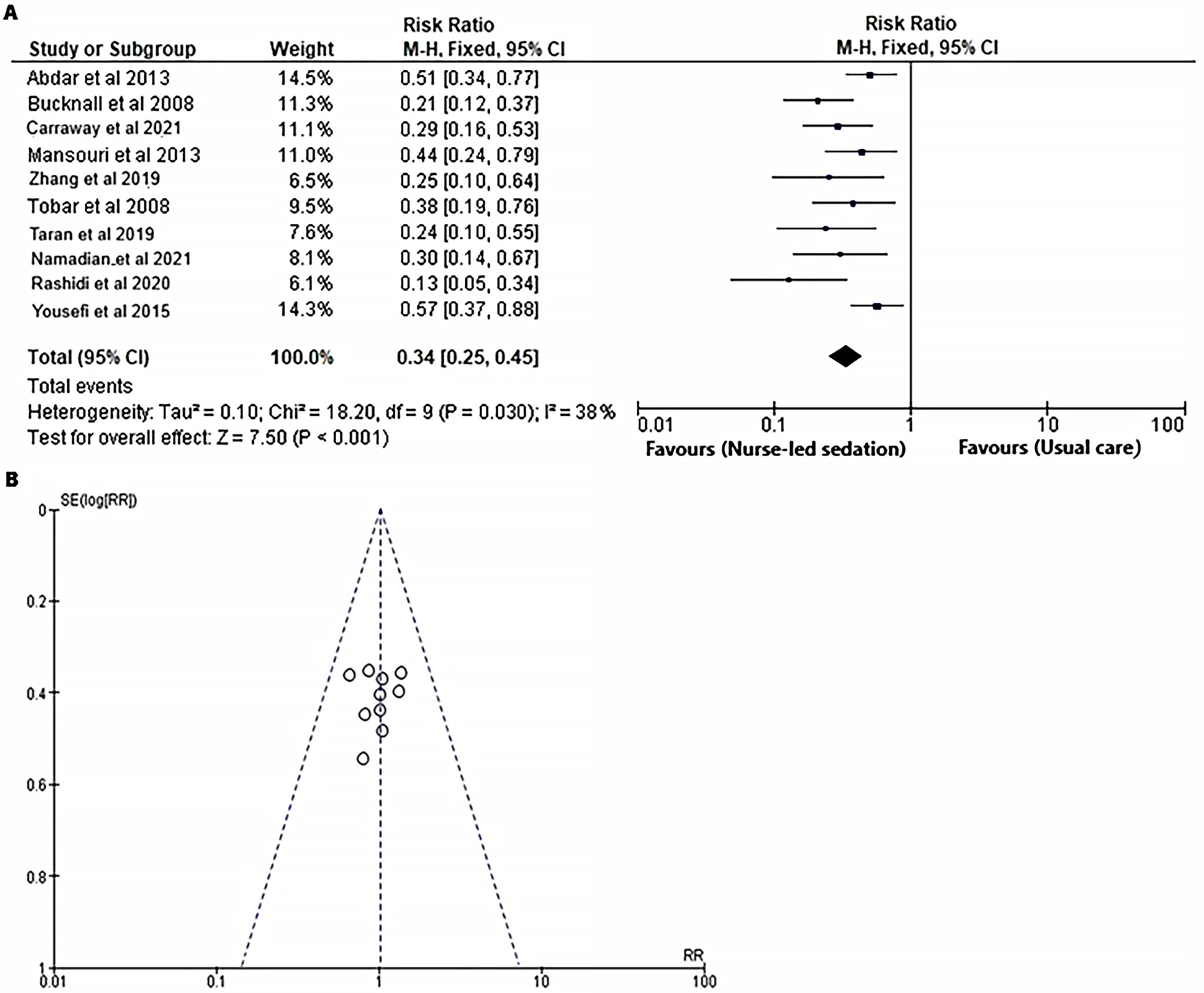
To evaluate the influence of the nurse-led sedation protocol on mortality rates in mechanically ventilated adults within the ICU, a comparison was made against standard care. The RR was calculated for both the intervention and control groups, utilizing event data obtained from the selected RCTs,18, 19, 20, 21, 22, 23, 24, 25, 26, 27 as depicted in Figure 4. The forest plot (Figure 4A) demonstrates that the nurse-led sedation protocol significantly reduces the risk of ICU mortality when juxtaposed with usual care (RR = 0.34 (95% CI: 0.25 to 0.45); χ2 = 18.20, degrees of freedom (df) = 9, Z = 7.50, I2 = 38%, and p < 0.001). Furthermore, the symmetrical funnel plot (Figure 4B) and the statistically nonsignificant p-value for Begg’s test (p = 0.134), which surpasses the established significance threshold of 0.05, suggest a minimal likelihood of publication bias.
Analysis of subgroups to assess the duration of ICU admission
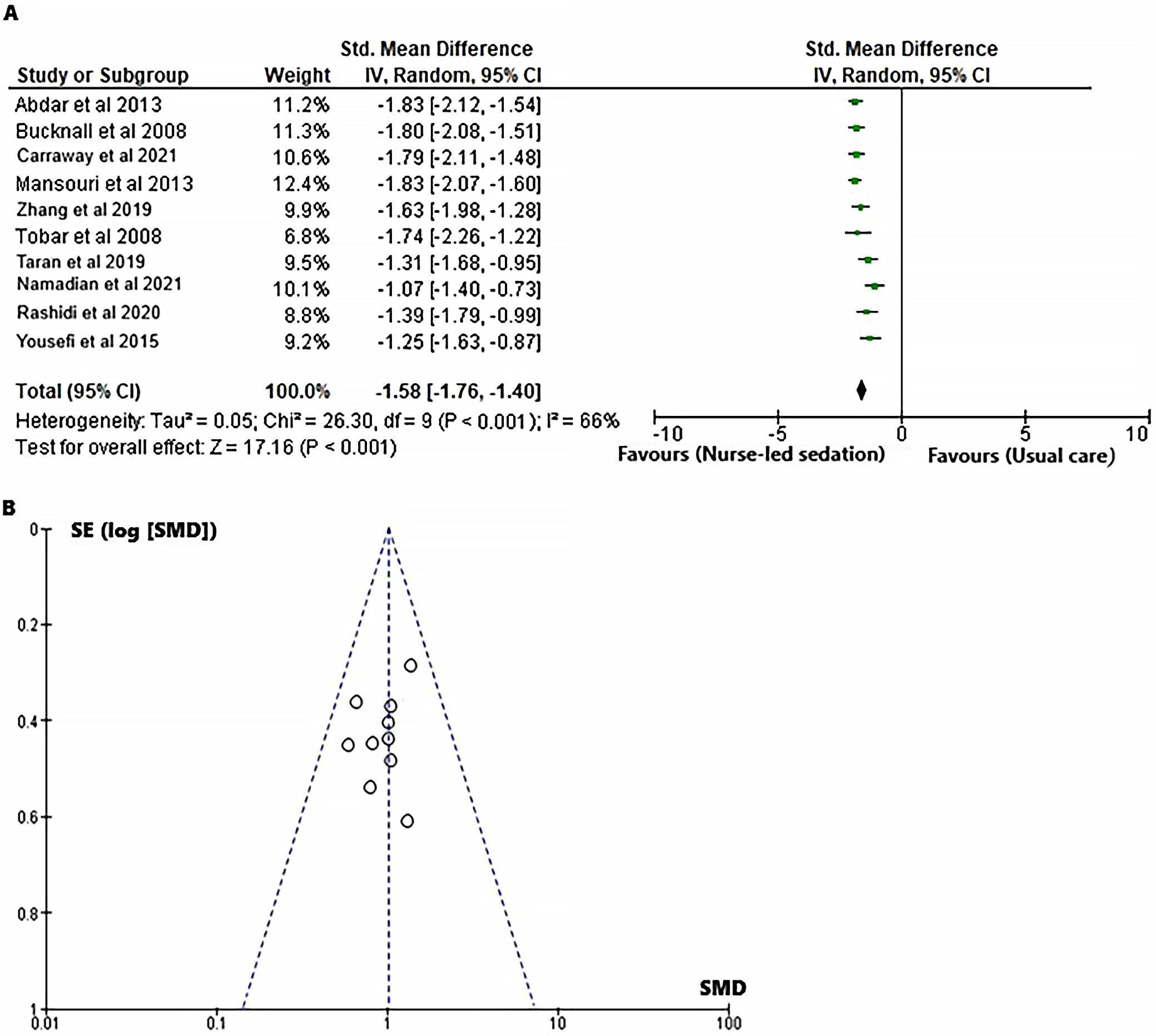
In order to assess the impact of the nurse-led sedation protocol on the length of ICU stay for mechanically ventilated adults in comparison to standard care, the SMD was calculated for both the intervention and control groups, utilizing event data sourced from the included RCTs,18, 19, 20, 21, 22, 23, 24, 25, 26, 27 as illustrated in Figure 5. The forest plot (Figure 5A) illustrates that the nurse-led sedation strategy yields a reduced length of stay in ICUs when contrasted with standard care (SMD = −1.58 (95% CI: −1.76 to −1.40); χ2= 26.30, df = 9, Z = 17.16, I2 = 66%, and p < 0.001). The symmetrical funnel plot (Figure 5B) and the nonsignificant p-value for Begg’s test (p = 0.176), which exceeds the established significance threshold of 0.05, indicate a minimal probability of publication bias.
Analysis of subgroups to assess the duration of hospitalization
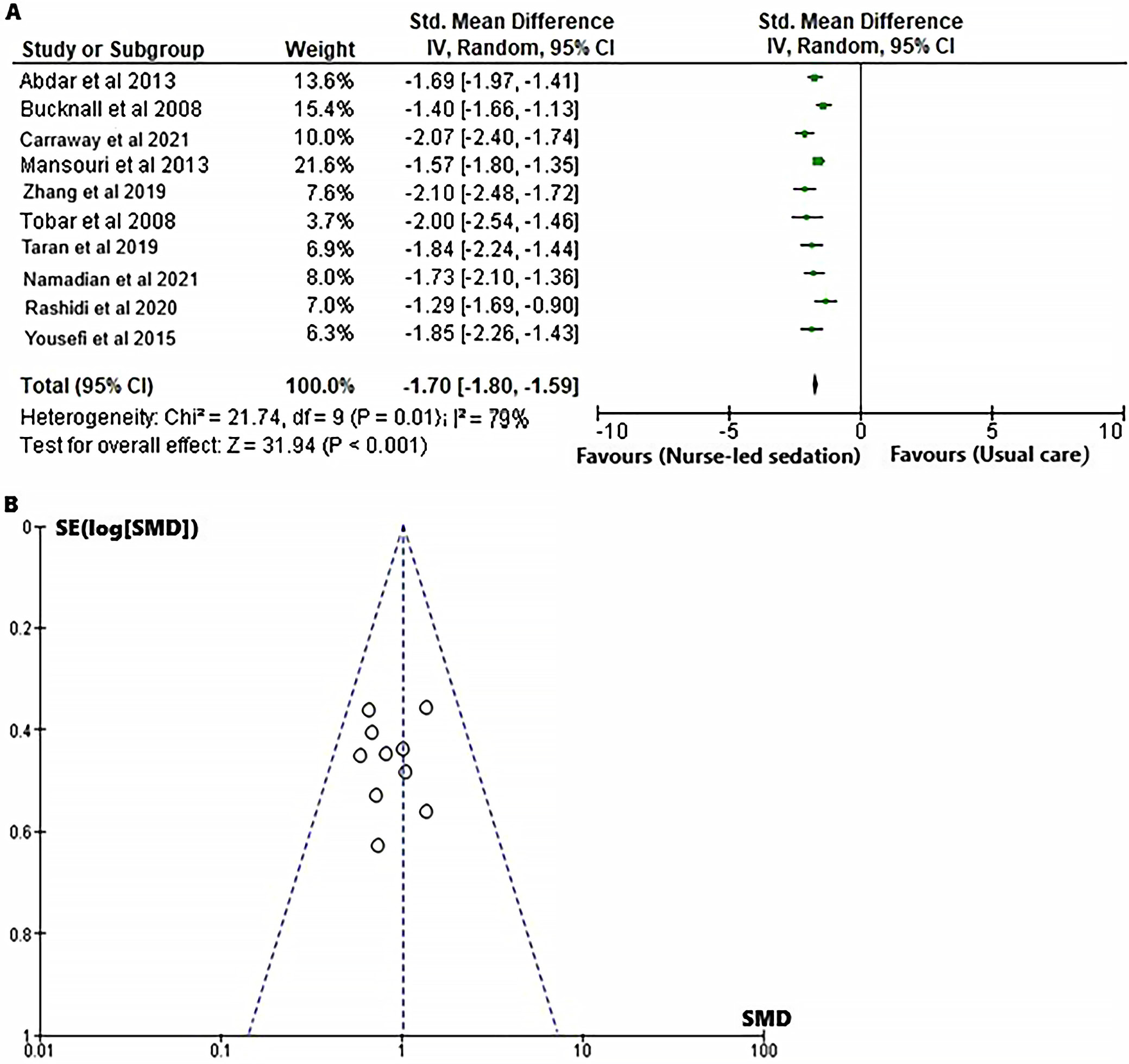
In order to assess the influence of the nurse-led sedation protocol on the duration of hospital stay for mechanically ventilated adults in the ICU, a SMD was calculated for both the intervention and control groups, utilizing event data obtained from the relevant RCTs,18, 19, 20, 21, 22, 23, 24, 25, 26, 27 as illustrated in Figure 6. The forest plot (Figure 6A) illustrates that the nurse-led sedation protocol is associated with a reduced duration of hospital stay when contrasted with standard care (SMD = −1.70 (95% CI: –1.80 to –1.59); χ2= 21.74, df = 9, Z = 31.94, I2 = 79%, and p < 0.001). Moreover, the symmetrical funnel plot (Figure 6B) and the statistically insignificant p-value for Begg’s test (p = 0.185), which surpasses the designated significance threshold of 0.05, suggest a minimal probability of publication bias.
Analysis of subgroups to assess the length of mechanical ventilation
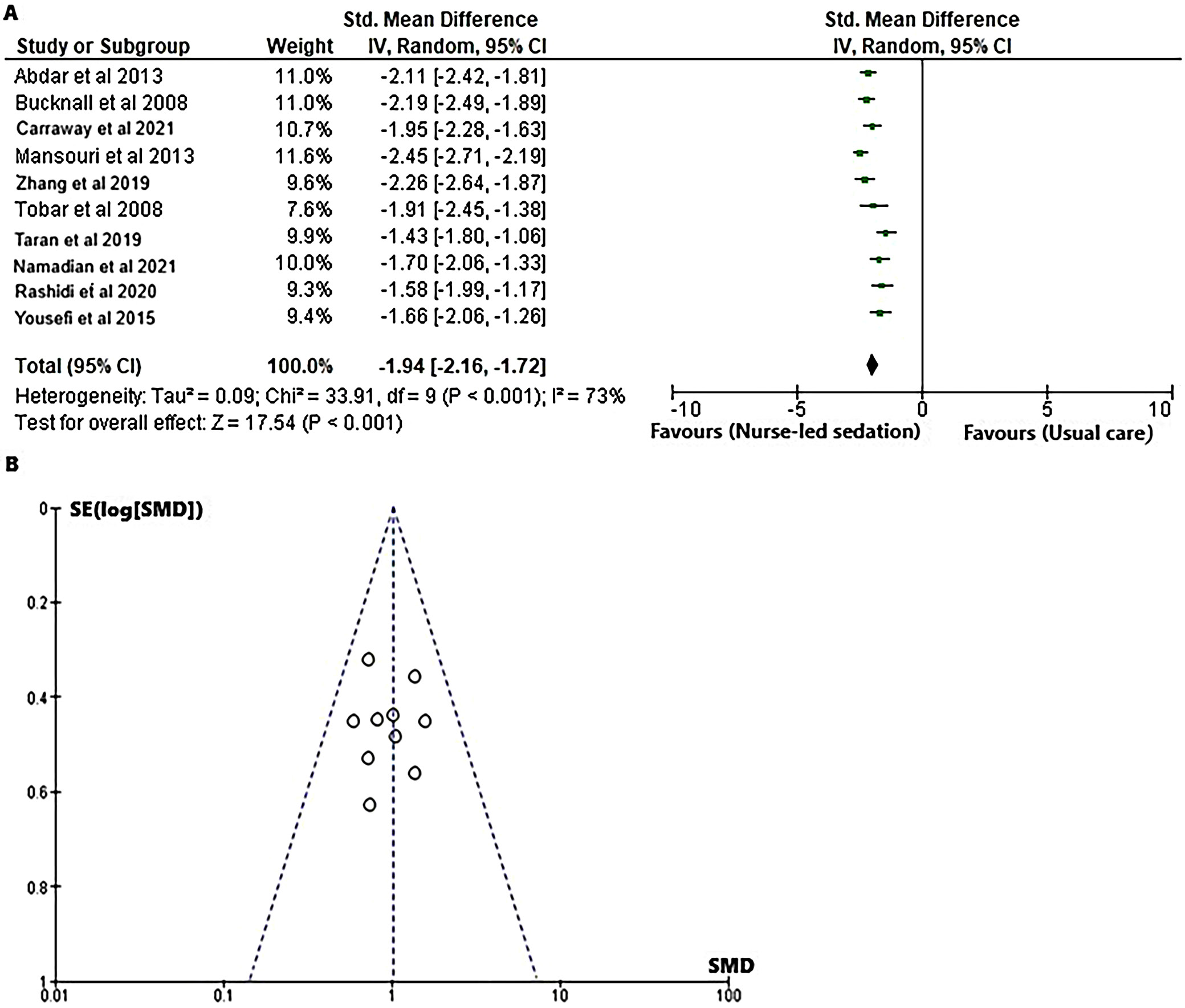
In order to evaluate the effect of the nurse-led sedation protocol on the duration of mechanical ventilation in adults receiving mechanical ventilation in the ICU, the SMD was calculated for both the intervention and control groups, utilizing event data obtained from the relevant RCTs,18, 19, 20, 21, 22, 23, 24, 25, 26, 27 as illustrated in Figure 7. The forest plot (Figure 7A) illustrates that the nurse-led sedation protocol led to a reduction in the duration of mechanical ventilation when contrasted with standard care practices as evidenced by a SMD of −1.94 (95% CI: −2.16 to −1.72); tau2 = 0.09, χ2= 33.91, df = 9, Z = 17.54, I2 = 73%, and p < 0.001). Moreover, the symmetrical funnel plot (Figure 7B), along with the statistically insignificant p-value for Begg’s test (p = 0.105), exceeding the established significance threshold of 0.05, indicates a minimal likelihood of publication bias.
Analysis of subgroups to evaluate the occurrence of self-extubation
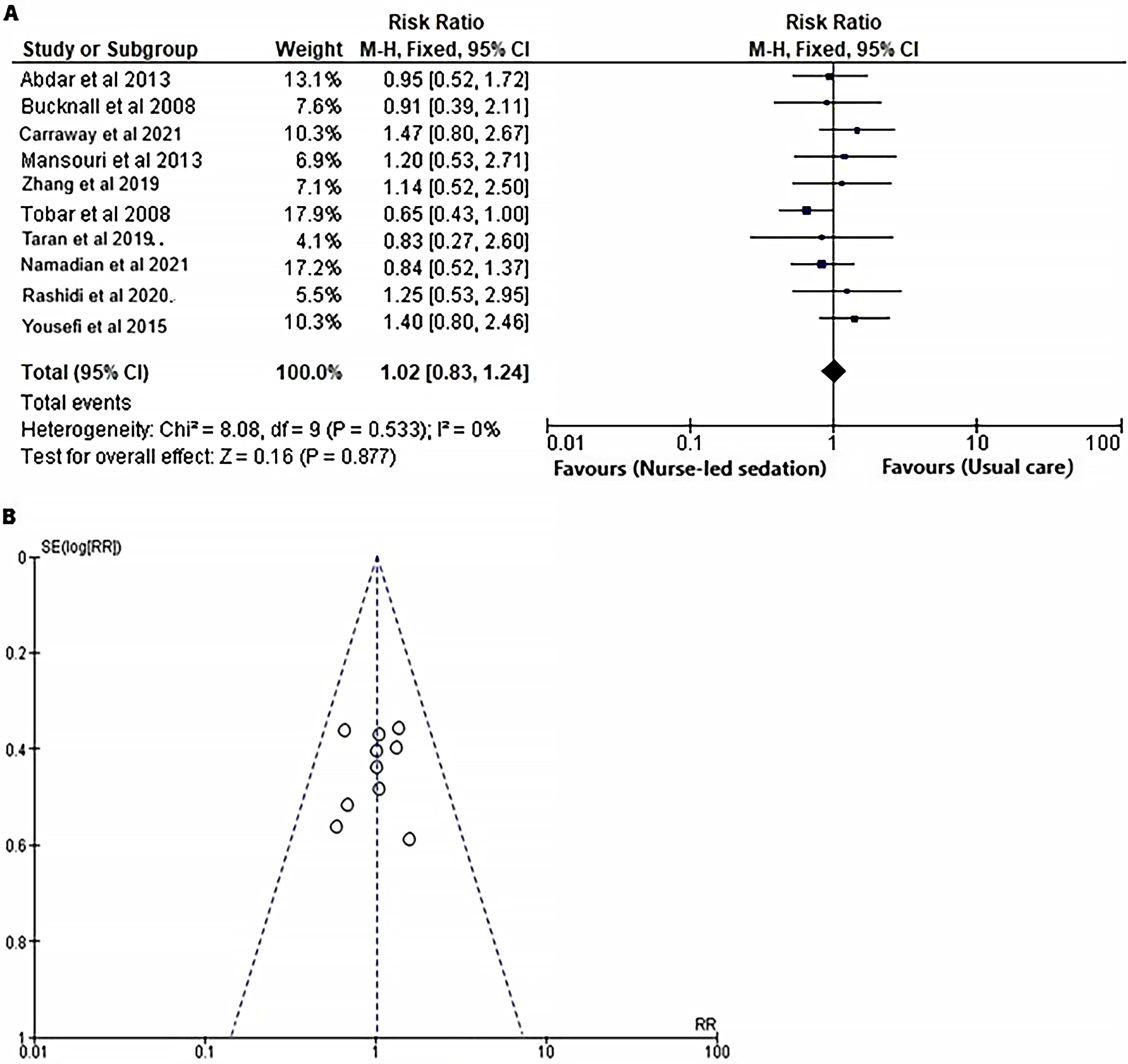
A meta-analysis was performed to evaluate the impact of nurse-led sedation protocols on the occurrence of self-extubation among mechanically ventilated adults in ICUs, utilizing data from 10 RCTs.18, 19, 20, 21, 22, 23, 24, 25, 26, 27 The RR was computed for both the intervention and control groups, as illustrated in Figure 8. The forest plot (Figure 8A) indicates that there was no statistically significant difference in the incidence of self-extubation between the 2 groups, as evidenced by a RR of 1.02 (95% CI: 0.25 to 4.45, χ2 = 8.08, df = 9, Z = 0.16, I2 = 0%, and p = 0.877). Moreover, the symmetrical funnel plot (Figure 8B), along with the nonsignificant p-value for Begg’s test (p = 0.166), indicates a minimal probability of publication bias, given that the p-value surpasses the established significance threshold of 0.05.
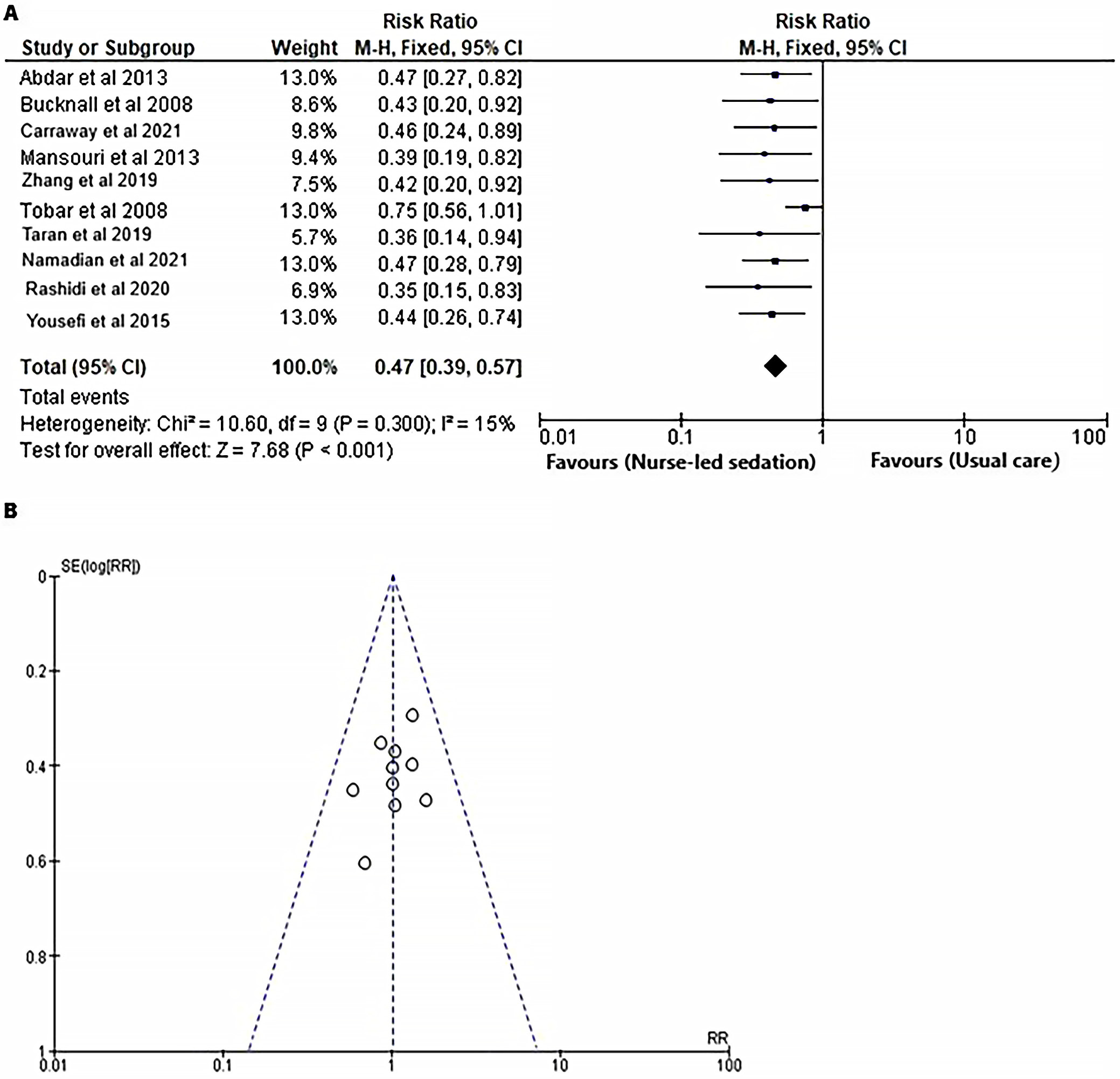
Analysis of subgroups to evaluate the occurrence of delirium
To assess the impact of nurse-led sedation protocols on the incidence of delirium in mechanically ventilated adults in ICUs, the RR was calculated using event data extracted from 10 RCTs, as illustrated in Figure 9. The results presented in Figure 9A indicate that the RR for delirium was significantly lower in the nurse-led sedation protocol group compared to the usual care group, with an RR of 0.47 (95% CI: 0.39–0.57; χ2 = 10.60; df = 9; Z = 7.68; I2 = 15%; p < 0.001). Furthermore, the funnel plot (Figure 9B) demonstrates symmetry, and Begg’s test for publication bias yielded a nonsignificant p-value (p = 0.190), suggesting that the results are unlikely to be influenced by publication bias.
Discussion
This systematic review and meta-analysis of 10 RCTs aimed to provide a comprehensive overview of the current evidence on nurse-led sedation protocols. The results of this analysis demonstrate that nurse-led sedation protocols can significantly improve patient safety outcomes. In ICUs where physicians are not consistently present at the bedside, effective communication between nurses and physicians is essential for ensuring timely treatment modifications and facilitating timely modifications to treatment instructions.47, 48 However, this communication often results in delayed implementation of treatment instructions, which can compromise patient care.49 To address this challenge, the implementation of a nurse-led sedation protocol can empower ICU nurses to adjust sedation doses in real-time based on patients’ sedation scores, without requiring physician input. This approach can prevent complications arising from excessive or inadequate sedation, such as respiratory depression, cardiac instability, and prolonged mechanical ventilation.50, 51, 52 By delegating sedation management to nurses, nurse-led sedation protocols can expedite clinical decision-making, reduce delays in treatment, and ensure standardized medical management. This is particularly crucial in ICUs, where timely and effective management of sedation is essential to prevent complications and improve patient outcomes. The nurse-to-patient ratio in ICUs is a critical determinant of nursing workload, particularly in the management of mechanically ventilated patients.53, 54 Nurse-led sedation protocols in mechanically ventilated patients in ICUs involve a multidisciplinary approach to optimize sedation management. Nurses regularly assess patients’ sedation levels using standardized scales, such as the RASS or SAS, and adjust sedation medications accordingly. Vital signs and pain levels are continuously monitored, and sedation medications are titrated to maintain optimal sedation levels. Daily sedation interruptions and SATs are performed to assess patients’ ability to breathe spontaneously and reduce sedation-related AEs. Nurses also implement pain management strategies, such as administering analgesics or using non-pharmacological interventions. Collaboration with physicians, respiratory therapists, and other healthcare professionals ensures consistent sedation management and clear communication with patients and families promotes informed care. Regular review and updates of sedation protocols ensure consistency with current evidence-based practices, and quality metrics monitoring evaluates protocol effectiveness and identifies areas for improvement. A 2016 survey revealed that approx. 1/3 of nurse respondents perceived that optimal nurse-to-patient ratios (1:1 or 1:2) significantly impacted sedation practices,55 while 45% of respondents reported administering sedative medications to facilitate completion of other nursing tasks. Notably, ICUs with higher nurse-to-patient ratios tend to exhibit more standardized and efficient sedation management for mechanically ventilated patients, which may contribute to improved patient outcomes, including shorter durations of mechanical ventilation and ICU lengths of stay. Furthermore, nursing behavior is a pivotal factor in sedation management, and increased nursing workload can compromise adherence to nurse-led sedation protocols.56, 57, 58 Conversely, the implementation of nurse-led sedation protocols has been shown to enhance patient safety, as evidenced by reduced ICU mortality rates, which can be attributed to improved sedation management and practice, thereby mitigating the risk of AEs related to excessive sedation, such as nosocomial infections and delirium.59 Hernandez et al.60 presented findings from their study, which revealed that protocolized sedation, whether implemented through algorithmic approaches or daily interruptions, is a safe and effective strategy compared to standard management in ventilated ICU patients. The results demonstrated that protocolized sedation is associated with a reduced RR for mortality (0.80 and a 95% CI of 0.68 to 0.93). Additionally, protocolized sedation resulted in a decrease in ventilation days, with a SMD of −1.12 days (95% CI: −2.11 to −0.14), and a notable reduction in ICU stay with a SMD of −2.24 days (95% CI: −3.59 to −0.89). However, the incidence of self-extubation did not exhibit a significant difference, with an RR of 1.20 and a 95% CI of 0.49 to 2.94. The findings from this study provide valuable insights to inform evidence-based practices in sedation management for critically ill patients in ICUs. Minhas et al.61 conducted a systematic review and meta-analysis of RCTs to evaluate the effects of protocolized sedation, utilizing either algorithms or daily interruptions, in comparison to standard care without protocolized sedation, on clinical outcomes in mechanically ventilated adult patients in ICUs. The findings of the present meta-analysis indicate that, in mechanically ventilated adults treated in closed, non-specialized ICUs, the implementation of protocolized sedation is associated with a significant reduction in overall mortality (15%), as well as decreased lengths of stay in both the ICU (1.73 days) and hospital (3.55 days), and a lower incidence of tracheostomy (31%), when compared to standard care without protocolized sedation. Our findings indicate that nurse-led sedation protocols are capable of reducing the duration of mechanical ventilation and the length of stay in the ICU when compared to standard care practices. Nonetheless, the variability of these outcomes was considerable, aligning with the results of earlier meta-analyses. Our findings elucidate that these protocols are associated with a significant reduction in ICU mortality (RR = 0.34 (95% CI: 0.25 to 0.45); I2 = 38%, and p < 0.001), duration of mechanical ventilation (SMD = −1.94 (95% CI: −2.16 to −1.72); I2 = 73%, and p < 0.001), length of hospital stay (SMD = −1.70 (95% CI: −1.80 to −1.59); I2 = 79%, and p < 0.001), length of ICU stay [SMD = −1.58 (95% CI: −1.76 to −1.40); I2 = 66%, and p < 0.001), and incidence of delirium (RR = 0.47 (95% CI: 0.39 to 0.57); I2 = 15%, and p <0.001). Nevertheless, the examination revealed no notable disparity in the occurrence of self-extubation (RR = 1.02 (95% CI: 0.83 to 1.24); I2 = 0% and p = 0.87) when comparing the nurse-led sedation protocol to standard care. The subgroup analysis of RCTs demonstrated ongoing heterogeneity, potentially stemming from differences in protocol quality, patient demographics, and sedation methodologies across various ICUs. A multitude of factors could have played a role in the observed heterogeneity, encompassing disparities in sedation protocols and assessment scales, variations in the sedative agents utilized along with their dosages, and differing modalities of mechanical ventilation employed in ICUs.
Additionally, the quality of the sedation protocols, the experience and training of the nurses, and the availability of resources and equipment may have also influenced the outcomes. Therefore, future studies should aim to standardize sedation protocols, minimize variability in sedation practices, and control for potential confounding factors to provide more generalizable findings.
Limitations
However, it is essential to acknowledge the study’s limitations. Selection bias may exist because we excluded studies that did not meet the inclusion criteria. Second, this meta-analysis includes only 10 RCTs with small sample sizes, limiting precise comparisons. Third, the included trials varied in patient populations and usual care practices. Lastly, the evaluated outcomes are based on subjective data only. Consequently, future long-term follow-up RCTs with larger sample sizes, varied patient demographics, and standardized usual care interventions are essential to validate the enduring efficacy and safety of nurse-led sedation protocols on clinical outcomes in mechanically ventilated adults in ICUs, with the objective of enhancing patient care.
Conclusions
This systematic review and meta-analysis provide compelling evidence that nurse-led sedation protocols can safely enhance clinical outcomes for mechanically ventilated adults in ICUs. Implementation of these protocols was associated with significant reductions in ICU mortality, duration of mechanical ventilation, length of ICU and hospital stays, and the incidence of sedation-related AEs. Despite these promising results, further research is necessary to confirm the long-term efficacy and generalizability of nurse-led sedation protocols, particularly in light of the methodological limitations and relatively small sample sizes of the included studies. Future investigations employing rigorous designs and larger cohorts will be critical to advancing evidence-based practice, optimizing ICU management, and improving patient outcomes.
Supplementary data
The supplementary materials are available at https://doi.org/10.5281/zenodo.15655332. The package contains the following files:
Supplementary Table 1. Quality assessment based on the AMSTAR-2 criteria.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.