Abstract
Background. The conservative treatment of idiopathic scoliosis (IS) may be enhanced through a combination of specialized physiotherapy, bracing, and the utilization of assistive devices.
Objectives. This study aims to evaluate the efficacy of the GraviSpine device in supporting the conservative treatment of IS in children.
Materials and methods. A cohort of 142 patients, aged 10–17 years with an average age of 12.76 ±1.75 years, undergoing treatment for IS with specific physiotherapy and bracing, received additional treatment with the GraviSpine device. The participants, selected based on inclusion and exclusion criteria, were divided into 2 age groups: group A (10–12 years) and group B (13–17 years). The mean follow-up period was 28.71 ±10.98 months. The assessment involved changes in post-treatment trunk rotation angles (ATR), Cobb angles, and functional lower limb length discrepancies (FLLDs) concerning age groups and scoliosis location.
Results. The proportion of patients showing improvement and stabilization was high in both groups A and B, at 71% and 90%, respectively. In group B, a significant reduction in the mean Cobb angle of –1.83° ±6.88°, p < 0.002, was observed. Furthermore, a significant decrease in the incidence of FLLDs was noted in thoracic and lumbar scoliosis locations, p < 0.002.
Conclusions. To enhance the effectiveness of conservative treatment for IS, the utilization of an assistive device such as GraviSpine may be considered, particularly when the child presents functional inequality of the lower limbs.
Key words: body posture, scoliosis, physiotherapeutic exercises specific to scoliosis, conservative treatment of scoliosis
Background
Idiopathic scoliosis (IS), characterized by a three-dimensional (3D) deformity of the spine, manifest in seemingly healthy children and can progress during periods of rapid growth.1, 2, 3 The etiology of IS remains elusive, with reports suggesting that scoliosis formation and progression may stem from the combined influence of various factors.2 Factors implicated in curvature progression include disturbances in central control of spinal posture4, 5, 6 and pelvic asymmetries.7, 8, 9, 10 Research indicates that the body schema, a stable yet adaptable representation of the central nervous system, can be influenced by sensory experiences.6 Children with IS may lack clear awareness of trunk misalignment, leading to gradual adaptation of their body pattern to the scoliotic state without recognizing the deformity.11, 12
In the construction of a body diagram, particularly in children at risk for the development of IS, the pelvic aspect and functional length of the lower limbs are crucial.13, 14, 15, 16, 17, 18, 19, 20 Numerous studies underscore the impact of functional leg length discrepancies (FLLDs) during childhood on the internal stresses within pelvic structures, potentially resulting in structural adaptive changes and pelvic asymmetries.21, 22, 23 Pelvic asymmetry, in turn, may contribute to spinal developmental disorders.7, 8, 9, 10, 14, 16 Grivas et al.14 suggest that FLLD affects 3–15% of the population and may stem from muscle contractures, biomechanical issues of pelvic joints, and dysfunction in other lower limb joints. Therefore, early detection and correction of FLLDs are reported to not only benefit IS but also aid in correcting lower limb deformities.24, 25, 26
The aforementioned findings and years of clinical observations inspired Dr. Marek Kluszczyński, a co-author of this study, to develop the innovative GraviSpine device (Technomex Sp z o.o., Gliwice, Poland). This device resembles an inversion table on which the child lies on their back and is suspended upside down at an angle of approx. 20–30°, held in place by 1 or both lower limbs (Figure 1).
GraviSpine features movable side pads mounted on rails at right angles to the child’s torso. Upon placing the child on the device, the physiotherapist positions the corrective pad’s arm on top of the curvature, applies a pad to the torso, and adjusts the sliding lever of the pad, resulting in compression of the torso from the back and side to the front and center, thus actively correcting the scoliotic curve. During the GraviSpine procedure, the patient concurrently performs derotational breathing exercises, which are facilitated by passive pad correction (Figure 2).
Properly constructed rotating head pads enable simultaneous correction of the spine in the frontal plane and derotation of the spine in the transverse plane by applying pressure to the trunk at the correct angle (Figure 2). GraviSpine leverages a reverse gravity phenomenon and passive 3D correction to stretch the contracted support structures, including the ligaments, tendons, muscle attachments, joint capsules, and intervertebral discs on the concave side of the curvature.
The arrangement of the articular surfaces in the facet joints of the spine in a standing position favors spine stabilization, posing challenges for correcting the deformed spine in scoliosis. Conversely, relieving spinal joints in the antigravity position causes the articular surfaces to move apart (Figure 3A).
Relaxation of the intervertebral joints and supporting tissues reduces the pressure required from the corrective pad to correct the curvature27 (Figure 3B).
If a child with scoliosis exhibited FLLDs during the examination, they were positioned on the GraviSpine with 1 (the functionally shorter) lower limb behind, aiming to increase tensile forces on the pelvic connections of the lumbosacral spine and pelvic internal ligaments (Figure 4). The distribution of force vectors on the GraviSpine is illustrated in Figure 5.
When the patient’s lower limbs are secured on an inclined plane, a frictional force (T) acts along the surface of the plane, preventing the body from sliding downward. Additionally, gravitational forces (Fg) and reaction forces (R) act on the body, along with the pressure exerted by the body on the plane. The contact force equals the component of the weight normal to the surface (F2).
The sliding force (F1) is the force that could potentially cause the person to slide off the plane, representing the tensile force of the pelvic structures on the shortened side of the lower limb. It is a component of the gravitational force acting parallel to the plane, according to the formula:
F1=|Fg| × sin(α),
where α – angle between the force and the direction in which the gravitational force acts.
The decision to utilize GraviSpine to influence the hip girdle system in compensating for FLLDs stemmed from the authors’ prior experience with the inversion table, practical insights in manual therapy, and literature reports confirming the positive impact of FLLD alignment on scoliosis.7, 15
Contraindications for the use of GraviSpine include:
• Post-surgical treatment of scoliosis;
• Infectious diseases affecting bodily functions;
• Congenital malformations of the osteoarticular system, especially of the spine and lower limbs, pose a risk of spinal cord injury during the procedure;
• Congenital osteogenesis imperfecta;
• Neurological conditions predisposing the child to procedural complications (e.g., epilepsy); and
• Cardiovascular disorders (after consultation with a cardiologist).
Other assistive devices are currently employed in the conservative treatment of IS globally. One such device utilizes the method referred to as fixation in space, elongation, derotation (FED), developed by Ferdinand Sastre. This device’s structure and function resemble GraviSpine, but the child is positioned in the standing position (Figure 6A).
The device operates by passively correcting curvatures using hydraulic pads with vertical traction of the spine fixed under the armpits.28, 29 The goal of FED is to equalize pressure on the facet joints of the vertebrae, which differs on the concave and convex sides of the curvature, a factor perceived by the author as contributing to IS development.
Another device, “SKOL-AS,” devised by Andrzej Stolarz,30 employs active-passive correction of curvatures in a seated position, coupled with asymmetrical breathing controlled by measuring pressure in cushions on the concave side of the curvature. To enhance efficacy, biofeedback, and visualization of pressure are utilized. According to the author, exercises on the SKOL-AS device serve as a form of postural re-education, combining 3D active-passive correction with proprioceptive stimulation techniques to program a new pattern of correct posture in the central nervous system (Figure 6B).
Another assistive device, “Delfin,” designed by Tomasz Szurmik, Józef Sitarz, and Marek Segiet, utilizes the Klapp position for passive-active self-correction of scoliosis by compressing the rib hump and lumbar shaft using properly positioned pads in an exercise known as “cat’s back” (Figure 6C).
The GraviSpine device utilized in this study is distinguished by its ability to not only provide active-passive curvature correction but also affect the hip girdle system using the antigravity phenomenon.
Objectives
This study aimed to assess the effectiveness of GraviSpine in supporting Physiotherapeutic Specific Scoliosis Exercises (PSSE) and bracing in the treatment of IS, as well as in eliminating functional inequalities in the lower limbs.
Materials and methods
The study received approval from the Jan Dlugosz University Ethical Committee under resolution KE-U/10/2021, dated September 28, 2021, and adhered to the principles of the Declaration of Helsinki. All parents of the participants were briefed on the study’s objectives and procedures, and their written consent was obtained prior to commencement. Individuals depicted in photographs provided written consent for the publication of their images.
Conducted at the “Tronina” Medical Rehabilitation Center, the study utilized data from patients treated between 2017 and 2021. Patients and their parents/caregivers were informed by physicians about the methods and procedures involved and provided written consent for treatment. Qualifications for treatment were based on X-ray examinations in accordance with the criteria outlined by the Society on Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT),31 specifically Cobb scoliosis ≥10° combined with vertebral rotation.
The study group received outpatient treatment following a standardized protocol, comprising weekly sessions lasting 90 min each. Treatment included 40 min of individual exercises based on selected schemes from the PSSE methods by Dobomed and Schroth, 2 sessions of 20 min each of derotational breathing exercises on the GraviSpine device,32 and 10 min devoted to learning correct posture during daily activities.
For each child, the physiotherapist recommended 2–3 exercises to be performed at home between sessions. If a FLLD was detected during clinical assessment, the GraviSpine suspension was adjusted to accommodate the shorter limb and correct the FLLD. A difference of 0.5 to 1.9 cm was considered indicative of a FLLD, while a difference exceeding 2 cm prompted additional examination with a tape measure to assess for structural limb shortening, which was an exclusion criterion. Although each child followed the same treatment model, exercises varied based on individual factors such as the type of IS, orthopedic deficits (e.g., muscle contractures, valgus knees, or tarsus), and sensorimotor deficits (e.g., posture, balance, and coordination disorders).
In the study group, 32% of children underwent combined therapy with PSSE, GraviSpine, and a Cheneau brace, in accordance with SOSORT criteria. This combination was recommended when the Cobb angle of the greatest scoliosis curvature was ≥20° and a Risser stage between 0–3.31 Despite the recommendation of wearing the brace for 23 h a day, actual usage, as reported by parents, ranged between 6 and 12 h daily. The duration of brace treatment varied from 6 to 38 months. Every 3 months, treatment progress was assessed by a physician through evaluation of the trunk rotation angle (ATR) using the Bunnell scoliometer, anteroposterior spinal curvature angles using a Saunders inclinometer, and brace fit. Functional lower limb length discrepancies were evaluated based on the level of heels when lying supine, following methods described by Cooperstein,33 modified by Travella et al.,34 and Friberg et al.35 Cobb angles were analyzed from initial and final X-rays. X-rays were measured twice using standard computer radiography software (RSR2LITE) by a specialist radiologist with 21 years of experience, who was blinded to patient data, and the results were averaged. In cases involving brace treatment, correction was consulted with an orthopedic technician. The treatment was conducted by a team consisting of 2 doctors, 8 physiotherapists, and 2 orthopedic technicians, working closely together. The mean follow-up period was 28.71 ±10.98 months.
Participants
Inclusion criteria included newly diagnosed children meeting the SOSORT criteria for IS,31 attending weekly visits for a minimum of 2 treatment cycles consisting of 10 sessions each, having a Risser stage between 0–4, and undergoing at least 1 year of follow-up. Exclusion criteria encompassed the presence of secondary scoliosis (congenital, neurological, metabolic, post-traumatic, etc.), mental retardation, respiratory disease, and prior treatment of IS using other methods.
The study group meeting these criteria included 142 children out of a total of 228 treated at the center, aged between 10 and 17 years, with an average age of 12.76 ±1.75 years. Women predominated, constituting 121 (85.2%) of the participants, with a mean age of 11.85 ±3.2 years, while 21 men (14.8%) with a mean age of 12.54 ±3.05 years were included. Patients were categorized into 2 age groups: group A (10–12 years old, n = 66) and group B (13–17 years old, n = 76), based on center protocols and established literature.31
Data analysis
Initial and final X-rays were used to analyze Cobb angles. Improvement in the curve (Cobb angle decrease ≥5°), stability (Cobb angle change ±5°), and progression (Cobb angle increase ≥5°) were compared.31 Similarly, initial and final measurements were utilized to analyze ATR values, with improvements (ATR angle decrease ≥2°), stability (ATR angle change ±2°), and progression (ATR angle increase ≥2°) assessed.31
Statistics
Due to the non-parametric distribution of data (verified via Q–Q plots), differences between pre- and post-treatment results were assessed using the Wilcoxon signed-rank test. The discrepancy in the functional length of the lower limbs was evaluated based on heel level in the supine position, assuming a difference of ≥5 mm.13 Fisher’s test was employed to analyze relationships between categorical variables.
Results
The mean follow-up was 28.71 ±10.98 months. The Cobb angles ranged from 10° to 46° within the group, with an average of 24.36° ±11.82°. The range of ATR was from 3° to 16°, with an average of 6.99° ±2.95°. Double-curved scoliosis predominated, with over 33% of children exhibiting a FLLD. The mean Risser score values for groups A and B were 1.38° ±1.4° and 2.33° ±1.1°, respectively (Table 1).
In group B, a statistically significant mean reduction in the Cobb angles after treatment was observed, amounting to 2.33° ±1.1°, with p = 0.002. Conversely, in group A, the post-treatment mean Cobb angle also decreased, but not significantly, by 1.38° ±1.4°. The percentage of positive treatment effects was high and increased with age, with the most frequent occurrences of improvement and stabilization found in group B (25% and 65%, respectively), while worsening was observed in only 10% of patients. Group A exhibited slightly lower frequencies, with improvement and stabilization at 18% and 53%, respectively (Table 2, Table 3).
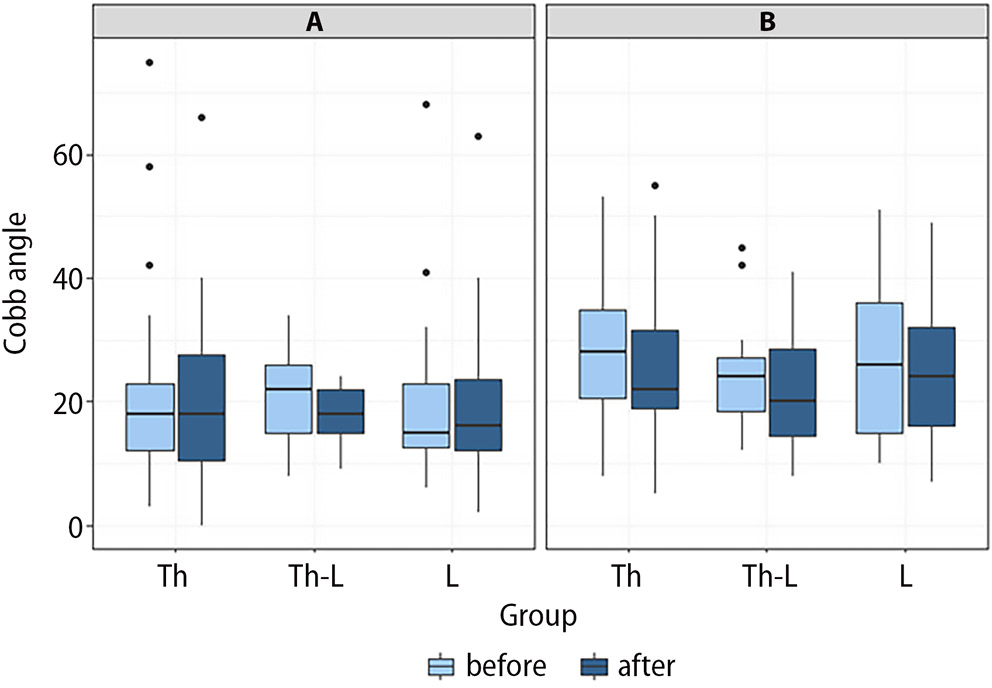
Significant differences in changes in the Cobb angle were observed depending on the location of the curvature. In the thoracic spine, group B reported significant reductions of –2.2° ±7.54° (10.17%), with improvement and stabilization in 23% and 67% of cases, respectively, and deterioration in 10% of patients. Group A showed slightly poorer results, with the mean Cobb angle decreasing by –1.62° ±9.36°, predominantly exhibiting stabilization in 54% of cases, while improvement and deterioration were equally present in 23% (Figure 7). In Figure 7, the upper and lower whiskers represent scores outside the middle 50% (i.e., the lower 25% of scores and the upper 25% of scores). The median marks the midpoint of the data and is shown by the line that divides the box into 2 parts. Points represent outliers.
In the thoracolumbar spine, the most significant reduction in Cobb angles was observed in group B, where 87% exhibited stabilization and 13% showed progression, with a mean Cobb angle decrease of –2.2° ±6.58° (6.36%). Group A had slightly inferior outcomes, with 62% experiencing stabilization, 15% improvement, and 23% deterioration, resulting in a mean Cobb angle reduction of –1.62° ±7.07° (–3.24%, Figure 7). In the lumbar spine, group B also achieved better results, with a 39% improvement and 51% stabilization, compared to group A’s 15% improvement and 45% stabilization (Figure 7).
A statistically significant reduction in mean post-treatment ATR was noted for the entire group, decreasing from a baseline ATR of 6.99° ±2.95° to 6.14° ±2.71° (p < 0.001). The most significant reductions in ATR were observed in the lumbar section, decreasing from 6.52 ±2.51 to 5.45 ±2.19 (p < 0.001), and thoracolumbar section, decreasing from 8 ±2.96 to 6.29 ±2.4 (p < 0.002, Table 4).
Following treatment, a significant reduction in FLLD was observed in both the thoracic (p = 0.002) and lumbar (p = 0.002) sections. The pre-treatment rate of FLLD ranged from 14.3% to 24.4%, while post-treatment rates ranged from 1.8% to 7.1% (Table 5).
Discussion
The study assessed the efficacy of GraviSpine-assisted PSSE and bracing therapy in children with IS, focusing on changes in Cobb, ATR, and FLLD angles post-treatment. While the use of devices in the conservative management of IS is well established, there are few reports evaluating their effectiveness. The treatment model employed in this study involved weekly treatment sessions and daily PSSE exercises at home under parental supervision, a regimen also recommended in other PSSE methods such as Schroth.36, 37
The risk of IS progression in the study group ranged from 40% to 75% according to the Lonstein and Corlson curve,38 prompting 32% of children to require orthopedic bracing in accordance with SOSORT guidelines.31
Results of the treatment model demonstrated high efficacy, particularly in group B, where a total of 90% exhibited improvement and stabilization, with a significant mean Cobb angle reduction of –2.33° ±1.1 (p < 0.002, Table 2, Table 3). Slightly less favorable outcomes were observed in the younger group A, possibly attributed to the longer study duration encompassing puberty, typically associated with the risk of scoliosis progression.39
A significant decrease in mean ATR was observed across the entire group, declining from a baseline of 6.99° ±2.95° to 6.14° ±2.71° (p < 0.001), with the most notable reductions in the lumbar (p < 0.001) and thoracolumbar (p < 0.002) locations (Table 4). Comparisons with device-assisted IS treatment studies revealed a study by Trzcińska et al.,40 where a significant reduction in the mean ATR angle was found in a group treated with FITS and the Dr. Sastre FED device.28, 29 However, the comparison was challenged by short follow-up times and a lack of X-ray evaluation. Another study by Kamelska-Sadowska et al.41 reported reductions in mean ATR angles following treatment with PSSE assisted by the SKOL-AS device.30 Nonetheless, this study also lacked an evaluation of Cobb angle changes.
Comparing the results of our study with reports evaluating the effectiveness of conservative IS treatment using PSSE and bracing without assistive devices, most publications focus on the Schroth method combined with bracing.42, 43
The study by Kwan et al.44 stands out for its longest follow-up period (18 ±6.2 months), where they achieved an improvement in 17% of patients, stabilization in 62%, and progression in 21% of patients. Similarly, Schreiber et al.37 reported comparable results, albeit with a shorter follow-up period of 6 months, noting a decrease in the Cobb angle of –0.4° and a significant decrease in the Cobb angle of the largest curve from –3.5° to –5.9° (p = 0.006). In another study focusing on the Schroth method, Kuru et al.36 obtained a reduction in the study group’s Cobb angle by –2.53° (p < 0.001).
The presented results of treatment using the Schroth method are similar to those obtained in our study, however, direct comparison is difficult due to the wide variety of studies.
When comparing our study’s results to those of the SEAS method, another longstanding approach in Europe, Negrini et al.45 showed slightly less favorable outcomes, with improvement in 23.5%, stabilization in 64.7%, and deterioration in 11.8% of treated patients. The most promising results were seen in a randomized controlled trial (RCT) evaluating the effectiveness of the SEAS method presented by Monticone et al.,46 demonstrating a reduction of the mean Cobb angle in the study group by –5.3° (p = 0.001). The majority of reports describing the effectiveness of PSSE methods highlight the significant benefits of combined therapy, namely PSSE with bracing.39, 42, 45, 46
In a study by Weinstein et al.,47 the success rate of brace treatment was 72%, compared to 48% after follow-up. In our study, 32% of the children were also treated with a brace, but the actual bracing time averaged only 6–12 h, which, according to Weinstein et al.,47 may yield an efficacy of only 40–70%.
In our study, we observed a significantly higher efficacy (80–90% combined improvement and stabilization in both groups A and B) than anticipated, given the short bracing duration. We suspect that we achieved this noteworthy effectiveness through combination therapy using the GraviSpine assist device. It is worth emphasizing that GraviSpine, like no other method, has an innovative effect on the correction of scoliosis in conditions of reduced gravity and elimination of limb length disproportions. Regarding FLLDs, our study demonstrated the effectiveness of combined PSSE and GraviSpine therapy in compensating for functional lower limb shortening, evidenced by a significant reduction in FLLDs in the thoracic and lumbar scoliosis locations. Reports by Brady et al. and Landauer et al.16, 22 underscore the critical impact of FLLDs on spinal deformities when occurring in childhood. Conversely, studies by D’Amico et al.7 and Moseley et al.15 affirm that aligning FLLDs during IS treatment, along with the posterior superior iliac spine planes of SIPS, is a favorable aspect in scoliosis management.
Numerous studies emphasize the importance of interventions aimed at compensating for functional lower limb shortening in treatment protocols.5, 7, 8, 9, 10 These interventions aim to enhance neuromotor postural control and spinal stability by achieving neutral sacrum alignment. Researchers suggest that improving neurological control of the postural pattern, particularly during scoliosis formative stages, can potentially mitigate scoliosis progression.5, 6, 48, 49, 50, 51 In scoliosis deformities, the constricted ligaments, muscle tendons, and joint capsules, due to their specific elasticity, can lead to secondary mutual interactions, exacerbating vertebral deformities. This imbalance contributes to a vicious cycle of force responses between the vertebrae and 3-dimensional anatomical abnormalities.52, 53 Meanwhile, during the GraviSpine treatment, the perivertebral structures on the concave side of the curve are stretched, which helps prevent the progression of deformation and breaks the vicious circle.
Antigravity alignment of the spine on the GraviSpine induces relaxation of connections between vertebrae, facilitating correction of the deformity. Studies by Torell et al.27 and Little et al.54 have demonstrated that relieving the spinal joints significantly reduces the corrective force required for scoliosis correction.
Derotational breathing exercises performed on the GraviSpine combine 2 corrective factors: internal, involving active derotational breathing by the child, and external, involving passive correction of curves in the frontal and transverse planes through pad action.55 This beneficial combination enhances the efficacy of scoliosis correction during treatment.
Therefore, the GraviSpine assistive device presented in this study may yield beneficial effects in the combined therapy of IS in children and adolescents, influencing various factors in the pathologically altered spine. It is worth noting that the treatment was well tolerated by the children, with a thorough analysis of possible side effects revealing no early or late risks. Data analysis on potential adverse events did not reveal any serious incidents up to the time the manuscript was sent, aside from a few instances of mild, short-term dizziness, particularly in tall, thin girls. These symptoms were effectively addressed by introducing a 1-min adaptation in a sitting position after transitioning from the head-down position, followed by dismounting from the device.
Limitations
Limitations of the study include its single-center nature and the absence of a control group for the presented treatment model. Additionally, the assessment of treatment effectiveness was compared only with the risk of progression using the Lonstein–Corlson curve in the discussion. It is important to acknowledge that the inventor of the GraviSpine method and device (Dr. M. Kluszczyński) is also the coordinator for the “Tronina” Medical Rehabilitation Center, where the GraviSpine device was evaluated. Further research with larger sample sizes and controlled designs would provide additional insights into the efficacy and safety of GraviSpine-assisted therapy.
Conclusions
To enhance the effectiveness of conservative treatment of IS, consideration may be given to incorporating an assistive device like GraviSpine, especially in cases where functional inequality of the lower limbs is diagnosed.