
















Abstract
Background. The red blood cell distribution width (RDW) is related to the mortality of patients with malignant tumors, but the relationship between RDW and the prognosis of cancer patients in the intensive care unit (ICU) has not been fully clarified.
Objectives. To investigate the role of RDW in predicting the prognosis of critically ill cancer patients.
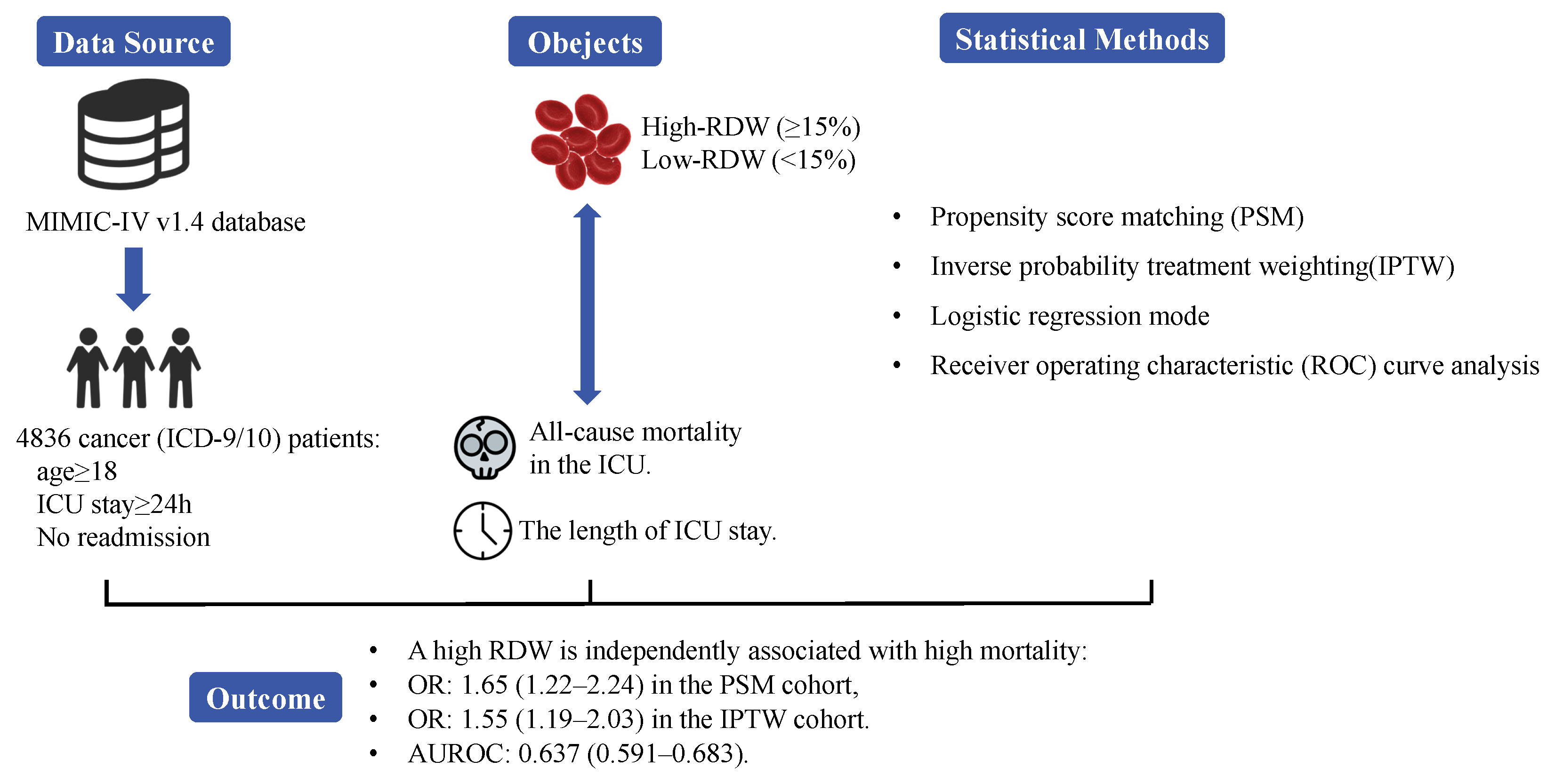
Materials and methods. A propensity score matching (PSM) study was conducted using data from adult patients with cancer, admitted to the ICU from the Intensive Care Medical Information Market IV (MIMIC-IV, v. 1.4) database. The correlation between RDW and ICU all-cause mortality was evaluated using a logistic regression model; stratification factors were considered. Additionally, a receiver operating characteristic (ROC) curve analysis was performed to compare the prognostic values of various blood biomarkers.
Results. Overall, 4836 cancer patients were included. The optimal critical RDW value was 15%. The RDW levels were independently correlated with ICU mortality in critically ill cancer patients, with odds ratios (ORs) of 1.56 (1.12–2.18) in the original cohort, 1.64 (1.27–2.12) in the imputation cohort, 1.65 (1.22–2.24) in the matched cohort, and 1.55 (1.19–2.03) in the weighted cohort. The forecasted performance of RDW is better than other blood biomarkers with an area under the ROC curve (AUC) of 0.637 (0.591–0.683).
Conclusions. The RDW has a prognostic value in critically ill cancer patients and a high RDW is independently associated with high mortality.
Key words: cancer, intensive care unit, red blood cell distribution width
Background
Due to high incidence and mortality rates,1 cancer has become an inevitable burden worldwide. Recently, cancer-related mortality rates have declined due to the advances in the strength of treatments. However, because of cancer-related complications and the side effects of cancer treatments, the number of patients with cancer being admitted to the intensive care unit (ICU) is increasing.2, 3 Approximately 1 in 20 cancer patients are transferred to the ICU within 2 years of their cancer diagnosis.4 Moreover, nearly 1 in 7 patients in the ICU have malignant tumors.5 Notably, the mortality rate of cancer patients is 30–77%, and the mortality rate for cancer patients requiring mechanical ventilation in the ICU exceeds 45%.6
Although the ICU provides life support and organ protection, it creates a heavy cost burden for treatment. Therefore, studies aimed at identifying effective prognostic indicators to identify a reasonable expectation of survival after treatment are urgently needed.7
Red blood cell distribution width (RDW) is a reflection of the volume dispersion of red blood cells, typically expressed as the coefficient of variation in red blood cell volumes. Recently, RDW was reported to be an independent predictor of mortality in cardiovascular disease (CVD)8 and various types of cancer.9, 10, 11, 12 Additionally, RDW is independently related to mortality in critically ill patients admitted to the ICU due to various etiologies.13, 14, 15 Although the mechanism between the association of RDW and mortality has not been elucidated, it may be involved in oxidative stress and inflammation.16 However, the relationship between RDW and the prognosis of cancer patients admitted to the ICU is unclear. Therefore, studies evaluating the correlation between RDW and the prognosis of critically ill cancer patients may help in predicting their survival and optimizing the clinical management of these patients. We hypothesized that RDW can predict ICU mortality in critically ill cancer patients.
Objectives
To investigate the role of RDW in predicting the prognosis of critically ill cancer patients.
Materials and methods
Data source
The data were retrieved from the Intensive Care Medical Information Market IV MIMIC-IV v. 1.4,17 a large, free, public, single-center database (https://mimic.mit.edu/). This database contains clinical information on 53,150 distinct patients admitted to the ICU at the Beth Israel Deaconess Medical Center in Boston, USA, from 2008 to 2019. The data include demographic characteristics, vital signs, laboratory data, treatment, drug use, and survival information. To protect the patients’ privacy, all identifiable patient information was removed. One of the investigators (LF) completed the collaborative institutional training program course required for ethical approval (record ID: 36309108).
Study cohort
Malignancies were identified using the International Classification of Diseases, version 9/10 (ICD-9/10): digestive system (140–159/C00–C26, C48), respiratory system and thoracic cancer (160–165/C30–C39), connective tissue (170–171, 176/C40–C41, C45–C46, C49), genitourinary system (179–189/C51–C68), nervous system (190–192/C47, C69–C72), hematological and lymphatic system (200–208/C81–C96), connective tissue (170–171, 176/C40–C41, C45–C46, C49), other (172–175, 193–195, 2090–2093/C43–C44, C50, C73–C76, C97), and metastatic (196–199, 2097/C77–C80).
The inclusion criteria (Figure 1) included: 1) age ≥18 years and 2) duration of ICU stay ≥24 h. Patients with hematological tumors or those repeatedly admitted to the ICU were excluded.
Data collection
Structured Query Language (SQL) in Navicat Premium (v. 12.0.18; PremiumSoft CyberTech Limited, Hong Kong, China) was applied to extract data from the MIMIC-IV within 24 h of ICU admission for a given patient. For laboratory measurements, the mean values ((maximum+minimum)/2) were selected. Data included demographic information (age, sex, race), type of care unit, type of cancer, comorbidities (congestive heart disease (CHD), chronic kidney disease (CKD), anemia, atrial fibrillation (AFib), coronary atherosclerotic heart disease (CAD), stroke, chronic obstructive pulmonary disease (COPD), and liver disease), use of mechanical ventilation, vasopressors and continuous renal replacement therapy (CRRT), laboratory data (RDW, red blood cell count (RBC), white blood cell count (WBC), platelet count (PLT), hemoglobin (Hb), blood urea nitrogen (BUN), creatinine, glucose (GLU), neutrophil/lymphocyte ratio (NLR), monocyte/lymphocyte ratio (MLR), and platelet/lymphocyte ratio (PLR)), and scoring systems (sequential organ failure assessment (SOFA) and simplified acute physiology score II (SAPSII)).
The diagnosis of acute respiratory distress syndrome (ARDS), acute kidney injury (AKI) and sepsis was based on the Berlin Definition, Kidney Disease: Improving Global Outcome guidelines18 and The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3),19 respectively.
Outcomes
The primary outcome of this study was all-cause mortality in the ICU. The secondary outcome was the length of ICU stay.
Statistical analyses
The random forest model was used to impute missing values and missing data (Figure 2). After imputation, the largest Youden’s index of the receiver operating characteristic (ROC) curves were used to determine the best RDW cutoff value based on ICU mortality. Then, the imputation dataset was stratified by RDW into a high-RDW group and a low-RDW group.
Propensity score matching (PSM) and inverse probability treatment weighting (IPTW)20 were applied to construct 2 models for controlling confounding factors. The patients were matched using the nearest neighbor algorithm of 1:1 according to propensity scores estimated using the following covariates: sex, age, race, care unit, type of cancer, comorbidities, use of ventilation, vasopressor, CRRT, ARDS, AKI, sepsis, SOFA, and SAPSII.
Baseline characteristics of all cohorts were reported. Continuous variables were represented by median (1st quartile (Q1), 3rd quartile (Q3)), while categorical variables were represented by frequency (percentage). The Kruskal–Wallis test was used to determine the statistical relevance of the study outcomes for continuous variables, while the Fisher’s exact test or χ2 test was used for categorical variables, as appropriate. The standardized mean difference (SMD), difference quotient between 2 means, and pooled standard deviation (SD) were also calculated to assess the balance between the high-RDW group and the low-RDW group.
A univariate logistic regression model was applied to determine the correlation between RDW and ICU mortality. Additionally, to assess the independent effects of RDW on ICU mortality, 2 multivariate logistic regression models were developed. In model I, we only adjusted for demographic information (age, sex and race). In model II, demographic information, type of cancer, comorbidities, use of mechanical ventilation, vasopressors, CRRT, acute diseases (ARDS, AKI and sepsis), and laboratory data (RBC, WBC, PLT, Hb, BUN, creatinine, and GLU) were included. Then, we conducted a sensitivity analysis on the original, imputed, PSM, and IPTW cohorts to evaluate the robustness of the results. The secondary outcome was evaluated by means of multivariate linear regression using model II.
All analyses and figures were carried out using the R v. 4.0.1 (packages: missForest, ggplot2, Matching, tableone, mice, and pROC; R Foundation for Statistical Computing, Vienna, Austria). A bilateral p-value <0.05 was considered statistically significant and a SMD < 0.1 was considered balanced.
Additional analyses
Stratified analysis was performed on the imputation cohort according to age, sex, race, type of cancer, comorbidities, and scoring system to evaluate the impact of RDW on ICU mortality among the different subgroups. The likelihood ratio test was used to estimate the effects between the stratified factors and RDW.
Finally, the ROC curves were drawn to compare the prognostic values of RDW, NLR, PLR, and MLR. Since the missing values for NLR, MLR and PLR were not imputed, the ROC curves were only drawn using the original dataset.
Results
Characteristics of subjects
We enrolled 4836 subjects who met the inclusion criteria. The baseline patient characteristics of the original cohort are shown in Table 1. The median age of all patients was 67.00 (59.00, 76.00) years, and the median RDW was 14.95% (13.75, 16.70). Among all the patients, malignant tumors of the digestive system were the most common (33.8%), followed by tumors of the respiratory system (22.3%), genitourinary system (16.2%), other tumor sites (6.8%), nervous system (5.9%), and connective tissues (2.0%). Metastatic tumors were present in 2560 (52.9%) patients. The prevalence of AKI and sepsis was 63.8% and 38.3% (3085 and 1851 patients), respectively. During the first 24 h following ICU admission, 1261 patients (26.1%) were placed on mechanical ventilation and 1314 patients (27.2%) required vasopressors. Patients were divided into high-RDW (≥15%) and low-RDW (<15%) groups consisting of 2483 and 2353 patients, respectively (Table 2). Patients with a high RDW were more likely to have digestive tumors (40.8% compared to 26.3%), distant metastases (60.0% compared to 45.5%), AKI (69.7% compared to 57.6%), and sepsis (46.6% compared to 29.5%), all with a SMD > 0.1. Additionally, patients in the high-RDW group had higher SOFA scores (4.00 (2.00, 6.00) compared to 2.00 (1.00, 4.00) in the low-RDW group) and higher SAPSII scores (40.00 (32.00, 48.00) compared to 34.00 (28.00, 41.00) in the low-RDW group), both with a SMD > 0.1.
Association between RDW
and primary outcomes
After matching and weighting, the baseline characteristics of the 2 groups tended to be balanced (Figure 3). The characteristics of the imputation, matched and weighted cohorts are shown in Table 2. The high-RDW group showed higher ICU mortality (13.9% compared to 5.4%) in comparison to the low-RDW group. In line with these results, the logistic regression analysis showed that high RDW levels were associated with ICU mortality in the IPTW cohort for the unadjusted cohort (1.56 (1.22–2.00), p < 0.001), model I (1.57 (1.23–2.01), p < 0.001) and model II (1.55 (1.19–2.03), p = 0.003) (Table 3). All variables in model II had variance inflation factors <10, which indicates an absence of multicollinearity. The Durbin–Watson test verified the independence of errors (value = 1.958). For evaluating the robustness of the results, a sensitivity analysis was conducted. The same trend was observed in the high-RDW group using model II in the origin cohort (1.56 (1.12–2.18), p = 0.002), imputation cohort (1.64 (1.27–2.12), p < 0.001) and PSM cohort (1.65 (1.22–2.24), p = 0.003) (Table 3).
Association between RDW
and secondary outcomes
There was no difference in the duration of ICU stays between the high-RDW group and the low-RDW group (2.40 (1.70, 4.10) compared to 2.30 (1.60, 4.00), with a SMD < 0.1). As shown in Table 4, the RDW had no effect on the length of ICU stay for the origin cohort (R2 = 0.15, p = 0.270), imputation cohort (R2 = 0.14, p = 0.140) and PSM cohort (R2 = 0.16, p = 0.050).
Additional analyses
The results of subgroup analysis for the imputation cohort are shown in Figure 2. Interactions were observed only in subgroups with respect to age (p = 0.014), respiratory and thoracic tumors (p = 0.028), AFib (p = 0.021), CHF (p = 0.026), and no differences were found in associations between RDW and the primary outcomes in the remaining subgroups. In patients with connective tissue tumors, RDW was not related to outcomes. RDW has higher predictive significance in patients with higher SOFA scores, which was the opposite for SAPSII. Additionally, patients with liver disease showed a significantly higher RDW-associated ICU risk of death (3.85 (1.8–9.53)). A high RDW was also associated with prognosis in both men and women. Notably, the relationship between a high RDW and mortality was weaker in older adults (age ≥60 years).
In the 1347 patients without any missing values for RDW, NLR, PLR, and MLR, we calculated the areas under the ROC curve (AUCs) to compare the predictive value of RDW, NLR, PLR, and MLR on ICU mortality (Figure 4). The AUC for RDW, NLR, PLR, and MLR in the context of ICU mortality in critically ill cancer patients were 0.637 (0.591–0.683), p < 0.001; 0.559 (0.510–0.608), p = 0.014; 0.485 (0.438–0.532), p = 0.530; and 0.501 (0.454–0.547), p = 0.982, respectively. The ROC analysis suggested that RDW is superior to NLR, PLR and MLR for predicting the prognosis of critically ill cancer patients.
Discussion
Our results suggest that a higher RDW is related to an increased risk of death in cancer patients admitted to the ICU. However, considering that the effects of blood cell parameters were evaluated, cases involving hematological and lymphatic malignancies were excluded from the final cohort. Importantly, similar trends were observed in the 2 models adjusted for different variables. This suggests that RDW is an independent predictor of the prognosis in critically ill cancer patients. The mean lifespan of a red blood cell is 120 days, and its homeostasis can be affected by many chronic diseases. To exclude bias introduced by chronic diseases, we conducted subgroup analyses in patients with common comorbidities. A forest plot indicated that there were interactions between AFib and CHF and RDW. This can be explained by the fact that risk factors related to the incidence of AFib and CHF are also the factors associated with increased RDW values, such as endothelial dysfunction, genetic susceptibility, aging, and others.21, 22
Many studies have confirmed RDW to have prognostic value in various cancers such as gastric,10 ovarian11 and lung cancer.12 For established cancers, there is growing evidence showing that local immune responses and systemic inflammation play a role in tumor progression and the overall survival (OS) rate in patients with cancer.23 The RDW is also a laboratory indicator for many chronic diseases and thus can be regarded as a nonspecific but outcome-related chronic disease marker.24 Cancer is often associated with chronic consumption and cachexia.25
Besides, plenty of studies have shown RDW to be a good prognostic predictor in ICU patients on account of acute overall inflammation,26, 27, 28 oxidative stress29 and arterial underfilling.30 The RDW is a risk factor for a severe prognosis in diseases such as sepsis,31 acute heart failure,32 autoimmune diseases, and liver diseases.33 However, during subgroup analysis, bias caused by comorbidities and acute ICU diseases (sepsis, AKI and ARDS) was not detected.
The exact biological mechanisms between RDW and cancer in ICU patients remain unclear. The underlying mechanism based on the available literature is that an altered myeloid lineage, abnormal iron metabolism and diminished response to erythropoietin34, 35 occurs in the setting of chronic and acute systemic inflammation, leading to reduced erythrocyte survival and an increased entry of premature erythrocytes into the circulation.36 Therefore, the lower survival in patients with a high RDW might be secondary to inflammation itself. Given the increasing number of cancer patients admitted to the ICU,2, 3 these patients might to some extent be considered as a separate subtype of ICU patients. Additionally, the exact indications for the use of RDW in such a background are unclear, although a high RDW was a risk factor in the vast majority of subgroups (Figure 5). All in all, the potential mechanisms and indications for the application of RDW in critically ill cancer patients need further exploration.
In addition to RDW, several prognostic parameters based on systemic inflammation have been proposed in cancer patients, including NLR,37 PLR38 and MLR.39 In this study, the performance of RDW was compared to these biochemical indicators. Importantly, the ROC curve analysis suggested that RDW had the best prognostic ability among these indicators.
Limitations
This study had some limitations. First, the data were obtained from the MIMIC-IV database. Although the large sample size was an advantage in this study, the data contained in this database cover a long period (2008–2019). Therefore, some information may be obsolete or missing, such as iron, B12 and other factors necessary for hematopoiesis. This, coupled with chemotherapy that can affect hematopoiesis, may influence the RDW in cancer patients. Second, this was a single-center retrospective study with incomplete numerical records and outliers in the database, which may have led to deviations. Third, we only selected the RDW measurement performed in the first 24 h after the admission to the ICU and did not monitor the dynamic trends in RDW levels. In an environment like the ICU, with numerous operations and treatments, such as blood transfusions, anti-inflammatory drugs, anticoagulant drugs, etc., the measured value of RDW can be greatly affected and should be interpreted carefully.
Conclusions
We showed that a high RDW in critically ill cancer patients is independently associated with ICU mortality. As a simple, inexpensive and routine laboratory index, RDW levels can indicate disease severity to a certain extent in cancer patients transferred to the ICU and guide the monitoring of these patients. However, large multi-center prospective studies are needed to confirm our results. The biological mechanisms underlying why RDW has a statistical significance among various clinical parameters are uncertain. Therefore, it is necessary to further explore the relationship between the dynamic changes of RDW and the prognostic and biological mechanisms to obtain a better clinical interpretation.




