Abstract
Background. The use of selective dorsal neurectomy (SDN) as a surgical treatment of premature ejaculation (PE) has increased for many years in Asian countries.
Objectives. To investigate the correlation between age and curative effects of SDN in primary premature ejaculation (PPE) in mainland China.
Materials and methods. From September 2016 to September 2020, 65 patients with PPE treated with SDN were selected for study. All of the patients were followed up from 12 to 56 (30.07 ±13.48) months. They were divided into 3 groups according to age: group A (22–30 years, n = 23), group B (31–37 years, n = 20) and group C (38–45 years, n = 22). The 5-item version of the International Index of Erectile Function (IIEF-5) and Premature Ejaculation Diagnostic Tool (PEDT) results, erectile rigidity grade, intravaginal ejaculation latency time (IELT), ejaculation control abilities (ECA) scores, and sexual intercourse satisfaction (SIS) scores were assessed in the 3 groups before and after operation to evaluate the clinical efficacy of surgery.
Results. Fifty-nine patients were finally followed up. The IIEF-5 scores and erectile rigidity grade of group A was significantly higher than that of groups B and C, both before and after surgery. The change of PEDT scores in group A was significantly higher than in groups B and C; the difference was statistically significant (p < 0.05). The IELT, ECA and SIS scores in group A were significantly higher than in groups B and C (p < 0.05). Operational efficiency ratio in groups B and C (65%, 70%) was significantly lower than in group A (95.24%).
Conclusions. The SDN as a treatment of PPE in different age groups allowed to achieve certain results. The highest surgical efficiency (95.24%) was observed in the 22–30 years age group and the lowest (65%) in the 38–45 years age group. Therefore, we believe that the best time for surgery is between 22 and 30 years of age.
Key words: curative effect, age, primary premature ejaculation, selective dorsal neurectomy
Background
Premature ejaculation (PE) is among the most common sexual disorders in adult males, affecting approx. 8–30% of adult males worldwide.1 It is generally accepted that PE is divided into primary premature ejaculation (PPE) and acquired premature ejaculation (APE).2 According to the International Society for Sexual Medicine (ISSM) definition, PE has the following characteristics: 1) ejaculation that always or nearly always occurs before or within 1 min of vaginal penetration (primary PE), or a clinically significant and bothersome reduction in latency time, often to about 3 min or less (acquired PE); 2) the inability to delay ejaculation in all or nearly all vaginal penetrations; 3) negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy.3 Premature ejaculation treatment methods include psychological, behavioral, medication,4, 5, 6 surgical and Chinese medicine treatment, among others.7 The abovementioned therapies can be used alone or in combination, and the relevant literature reports specific clinical curative effects. However, there are still problems such as high recurrence rate, side effects and uncertain long-term efficacy.8, 9 In the course of our clinical work, we found that an increasing number of patients with PPE still cannot be treated with conservative therapies, and some patients even voluntarily give up nonsurgical therapies and seek surgical treatment. A representative surgical procedure for PE is selective dorsal neurectomy (SDN), and the clinical application of SDN has opened up new avenues for the treatment of PPE. Although ISSM guidelines disregard surgical treatment of PE arguing that SDN may lead to permanent loss of sexual function, no literature supports its view.10 On the contrary, over the years, in Asian countries, an increasing number of studies have found significant curative effects of the procedure. Still, varying levels of efficiency in different studies may be related to the inclusion criteria of surgical cases, selection of surgical modalities and standards of efficacy assessment. Also, in our regular follow-up, we found that the improvement in intravaginal ejaculatory latency time (IELT), ejaculation control abilities (ECA) score and sexual intercourse satisfaction (SIS) score was more pronounced in younger patients (22–30 years) after the procedure. We conducted a controlled study to investigate the correlation between SDN curative effects and age. This study encompassed 65 patients with PPE treated with SDN in our hospital from September 2016 to September 2020, in order to compare the postoperative efficacy of SDN in PPE patients of different ages, and investigate the correlation between age and curative effects of SDN.
The study followed the ethical principles for clinical research based on the Declaration of Helsinki. Patients in the study agreed and volunteered to participate in the study, and all patients received informed consent and the confidentiality of their personal data was has been ensured. The Ethics Committee of our hospital – an independent body composed of medical and nonmedical staff – approved the study (approval No. KY2021-340).
Objectives
To investigate the correlation between age and curative effects of SDN in PPE in mainland China.
Materials and methods
General information
Sixty-five patients were included in this study and divided into 3 groups according to age: 23 in group A (22–30 years); 20 in group B (31–37 years); and 22 in group C (38–45 years). All patients had normal erectile function (IIEF-5 ≥ 22) and varying degrees of symptoms of premature ejaculation (PEDT ≥ 11). The development of external genitalia was normal, and there were no abnormalities in the testes, epididymis and spermatic cord examination. The measurement of blood glucose, blood pressure and thyroid hormone (T3 and T4) tests were not abnormal.
Selection criteria
The inclusion criteria were as follows: 1) good psychological state; 2) normal erectile hardness during sexual intercourse; 3) sensitive penile glans; 4) quality of sex life seriously affecting the relationship between couples; 5) strong desire for surgery; 6) voluntary abandonment of nonsurgical treatments. Based on Clinical Characteristics Consistent with Primary Premature Ejaculation,11 patients who had a regular sexual partner and had regular sex for at least 6 months and met the above criteria were enrolled in this study.
The exclusion criteria were as follows: 1) patients younger than 22 and older than 45 years; 2) patients with poor psychological status; 3) patients with concomitant prostatitis; 4) patients with hyperthyroidism; 5) patients addicted to drugs; 6) patients with insertion disorders; 7) patients with APE, etc.
Surgical method
Following proper anesthesia, the surgeon made a circular incision at 0.6–0.8 cm from the coronal sulcus (circumcision first if the foreskin is redundant; if circumcision has been done, the cut ran along the original incision; Figure 1A). Then, the surgeon cut the skin and subcutaneous tissue layer by layer, and separated the penile fascia tissue at a distance of about 0.8–1.5 cm from the coronal sulcus. After separating about 3–4 layers of penile fascial tissue, the dorsal penile nerve could be seen above the anatomical level of the deep dorsal penile vein and dorsal penile artery. It is yellowish, elastic and rich in trophoblastic vessels, with about 0.2–1.5 mm transverse diameter. Centering on the 12 o’clock in the middle of the dorsal side of the penis, the surgeon used fine tip forceps and microscopic mosquito-type separator forceps to reveal the dorsal penile nerve by separating both sides, reached the urethral corpus cavernosum ventrally to the penis, and used silk thread to gently lift and mark the separated dorsal penile nerve (Figure 1B). Depending on the patient’s specific condition, one nerve at each of the 3, 9 and 12 o’clock of the penile head was preserved. In principle, approx. 3–4 dorsal penile nerves were preserved, and the rest of the dorsal penile nerves were severed and a length of 3–4 cm was removed (Figure 1C). If the retained dorsal penile nerve was >1.5 mm in transverse diameter, the surgeon continued to separate dorsal penile nerves distally until approaching the head of the penis, and then the operative area was sutured in 2 layers (Figure 1D). We performed the indwelling of the catheter at the end of the procedure.
Observation items and method
Observation items
The following measurement tools were used: 5-item version of the International Index of Erectile Function (IIEF-5) score, erectile hardness grade, Premature Ejaculation Diagnostic Tool (PEDT) score, IELT, ECA score, and SIS scores for patients and partners. The efficiency of surgery and the incidence of adverse reactions were also recorded.
Survey data
The patients resumed normal sexual life 1 month after surgery.12 All patiens were requested to measure and recorde IELT (in seconds) for each sexual intercourse with a stopwatch, for 4 occurrences of sexual intercourse over 2 weeks. The geometric mean IELT calculated for each patient.13 The following items were calvulated from the data and statistics prepared by the physicians: ECA scores (PEDT 1, 2, 3 items), SIS scores of patients (IIEF6, 7 and 8 items), SIS scores of partners (IIEF 10, 13, 14 items), and the occurrence of postoperative adverse effects.
Evaluation of the curative effect
According to the expert consensus on SDN in China, patients in whom surgery was judged to be effective had the following characteristics: 1) IELT ≥ 2 min after surgery; 2) increased ejaculatory control; 3) improved sexual satisfaction of patients and spouses. These 3 items are essential indicators for assessing the treatment effect of PE after surgery, and meeting any of them is considered adequate.14
Statistical analyses
The IBM SPSS v. 26.0 (IBM Corp., Armonk, USA) and GraphPad Prism v. 8.3.0 (GraphPad Software, San Diego, USA) software were used for statistical analysis and graphical plotting. All the data were analyzed with the Shapiro–Wilk test for normal distribution (Table 1). The variables not distributed normally (age, duration of PE, number of DN, follow-up time, IELT, ECA, SIS, IIEF-5, and PEDT) were described using median and quartiles (M (Q1, Q3)), the comparison between groups (IELT, ECA, SIS, IIEF-5, and PEDT) was performed with the Kruskal–Wallis test and the intra-group comparisons (IELT, ECA, SIS, IIEF-5, and PEDT) was performed with the Friedman’s test. Numeric data (marital status) were expressed as n (%); the erectile hardness grade of the penis was compared using nonparametric rank-sum test; the exact Fisher’s test was used for comparison between groups, for efficiency of surgery and incidence of adverse reactions; the Cochran–Armitage χ2 test15 was used to determine the relationship between age and efficiency of surgery. A value of p < 0.05 was considered statistically significant.
Results
Clinical data
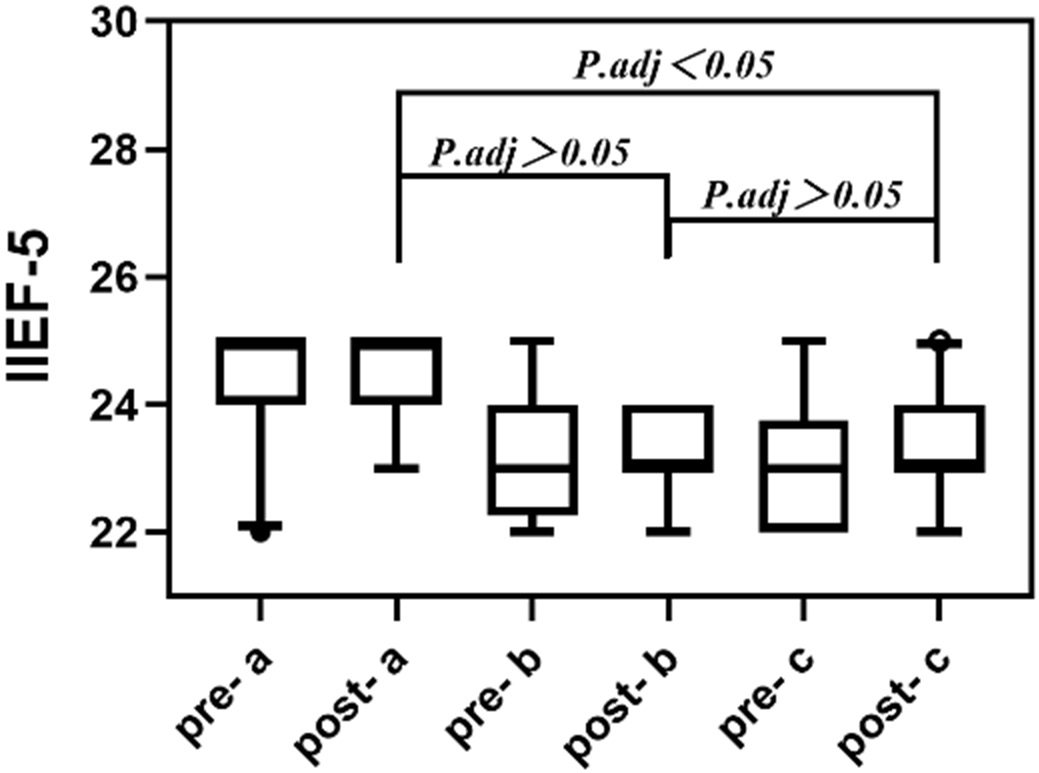
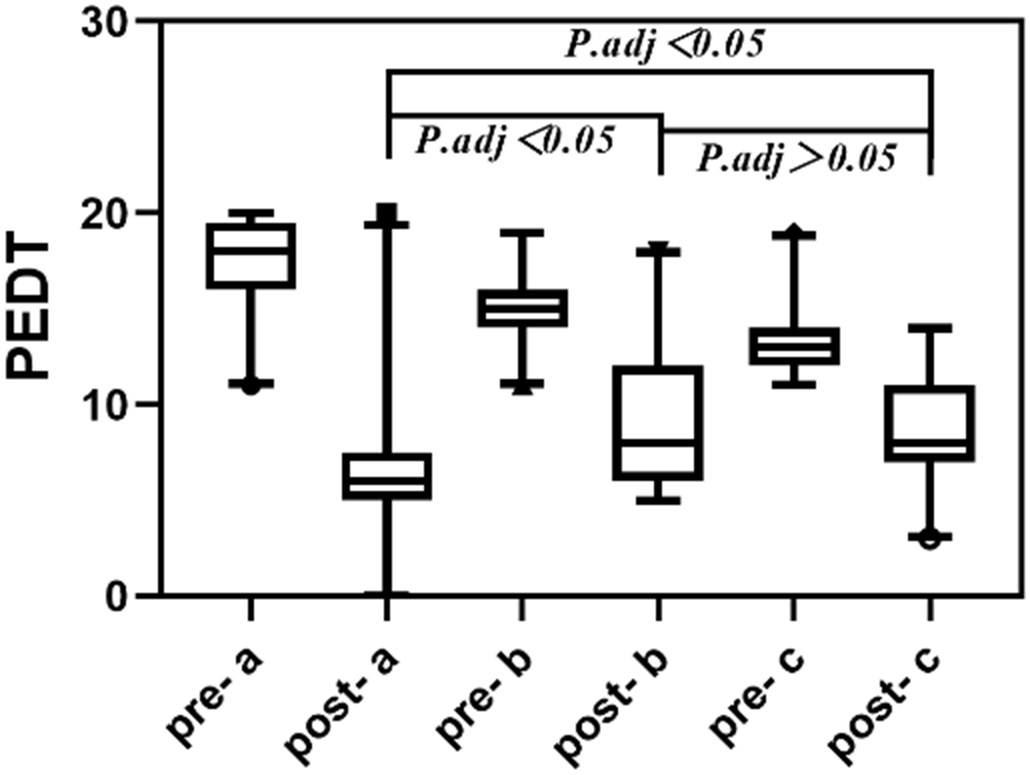
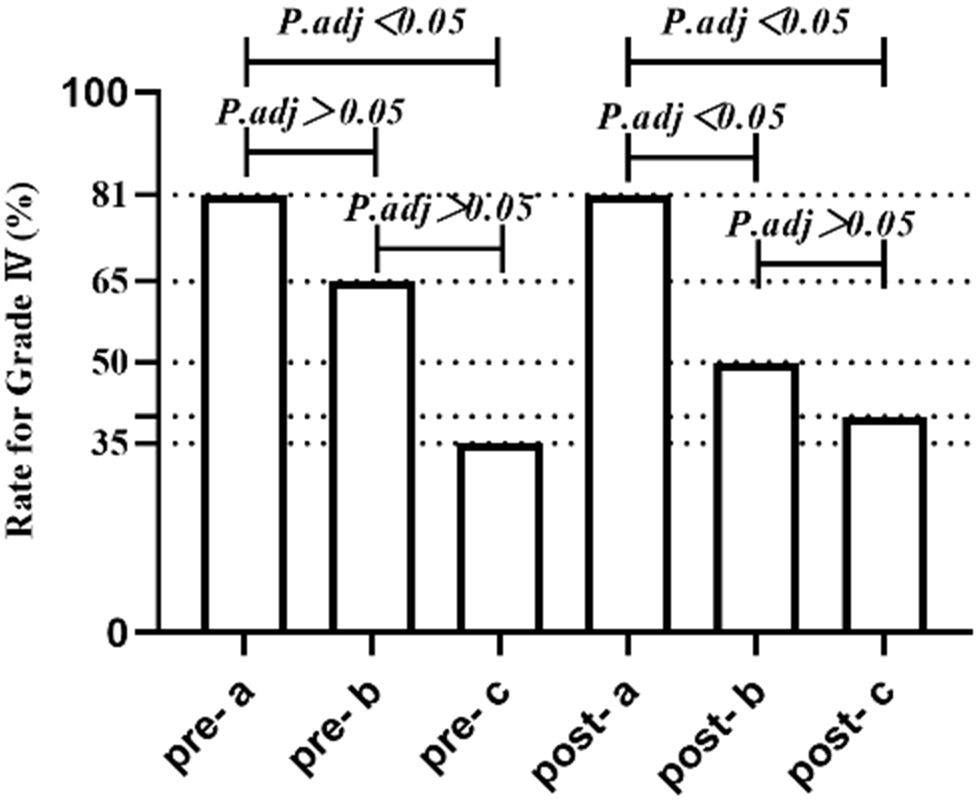
Two patients in the group A and 1 patient in group C refused to be followed up, while 1 patient in group C was lost to follow-up due to a change of personal information; the remaining 61 patients completed the follow-up (Table 2). There was no statistically significant difference regarding the IIEF-5 score between the 3 groups before and after surgery; we observed a statistically significant difference between groups A and C and groups A and B (p < 0.05), and no statistically significant difference between groups B and C (Figure 2). No statistically significant difference regarding PEDT between the 3 groups before and after surgery was observed; a statistically significant difference between groups A and C and groups B and C (p < 0.05) could be seen, while no statistically significant difference between groups A and B (Figure 3) was visible. There was no statistically significant difference regarding erectile rigidity grade between the 3 groups before and after surgery. Before the surgery, the difference between groups A and B (Z = −1.763, p = 0.078) was not statistically significant, while the difference between groups A and C (Z = –2.949, p = 0.003) was statistically significant, and the difference between groups B and C (Z = −1.255, p = 0.209) was not statistically significant (Figure 4). After the surgery, the difference between groups A and B (Z = −2.063, p = 0.039) was statistically significant, the difference between groups A and C (Z = −2.654, p = 0.008) was statistically significant, and the difference between groups B and C (Z = −0.628, p = 0.53) was not statistically significant (Figure 5).
There were statistically significant differences in IELT, ECA scores, SIS scores of patients, and SIS scores of partners for intragroup comparisons before and after surgery in the 3 groups (p < 0.05). Before the surgery, there were no statistically significant differences in IELT, ECA scores, SIS scores of patients, and SIS scores of partners between the 3 groups (p > 0.05). After the surgery, there were statistically significant differences between groups A and C and A and B in IELT and ECA scores (p < 0.05). While we observed statistically significant differences between groups A and C in SIS scores of patients and SIS scores of partners (p < 0.05), the remaining groups showed no statistically significant differences between them regarding these scores (Table 3).
Clinical efficacy
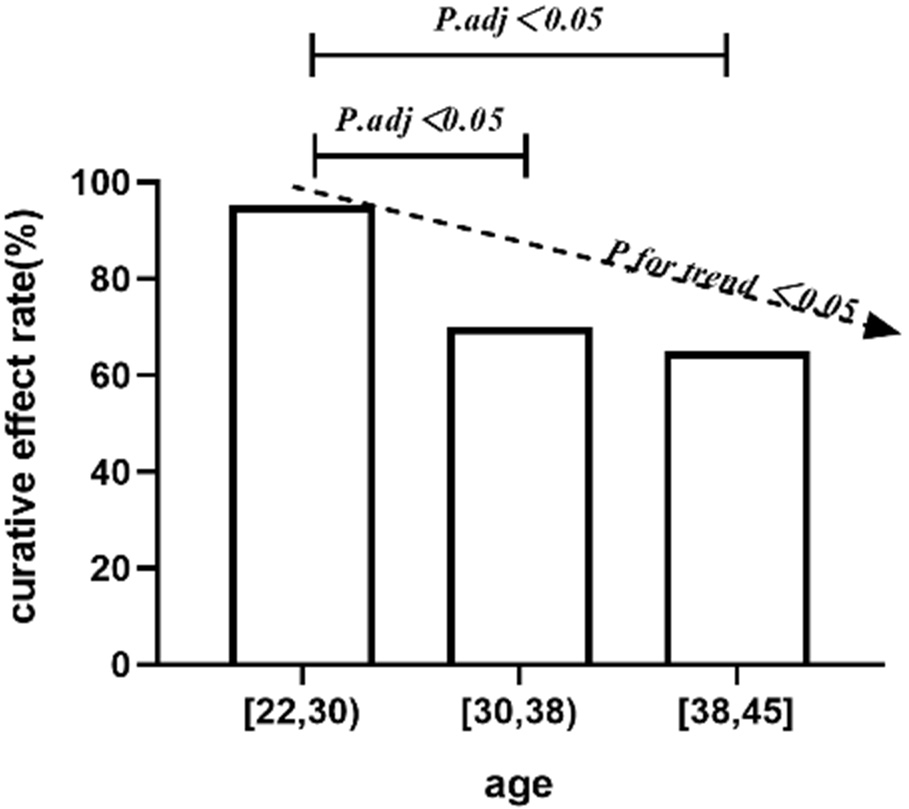
The results of postoperative efficacy assessment were as follows: (n = 21): 20 cases of valid and 1 case of invalid; group B (n = 20): 14 cases of good and 6 instances of invalid; group C (n = 20): 13 cases of valid and 7 instances of invalid. The effective rate of patients in group A (95.24%) was significantly higher than those in groups B and C (70% and 65%, respectively); the difference was statistically significant (p < 0.05) and the gradual decrease in curative effect rate with age was also statistically significant (Figure 5).
Adverse reactions
In group A, 1 case of local pain and 1 case of tethered edema was observed, while in group B, 2 cases of local pain, 2 cases of tethered edema and 1 case of subcutaneous hard nodes were recorded. As for group C, 1 case of tethered edema and 1 case of poor appearance occurred, with no statistically significant difference (p > 0.05). None of the patients in the 3 groups had any complications such as abnormal penile erection or erectile dysfunction.
Discussion
The causes and mechanisms of PE are not fully understood. It is currently believed that PPE is a sexual dysfunction caused by psychological,16 behavioral and neurobiological factors. The neurobiological causes include penile sensory hypersensitivity,17, 18, 19 ejaculatory reflex hyperactivity, enhanced sexual arousal, possible endocrine diseases, genetic susceptibility, and central 5-HT receptor dysfunction.20, 21 Factors such as penile sensory hypersensitivity or increased penile sensory nerve excitability play an essential role in PPE.22 Zhang et al. found that patients with PPE have more dorsal penile nerves compared to normal subjects, which may be one of the reasons for their penile sensory hypersensitivity or increased penile sensory excitability.23 Rosen et al. suggested that the cause of PE may be closely related to a decrease in penile sensory threshold and increased neural excitability.24 However, the current view is that penile head hypersensitivity and ejaculatory reflex hyperactivity are the leading causes of PE. The main idea of clinical surgery for PPE includes selectively removing the dorsal penile nerve endings, which can reduce nerve impulse transmission, thus reducing the sensitivity of the penile head and prolonging the ejaculatory latency.14 Some studies have shown that SDN is effective in delaying ejaculation and does not affect erectile function. Zhang et al. found that at a 6-month follow-up the efficacy rate in 128 patients was 87.5%, with satisfactory clinical outcomes and no severe complications such as erectile dysfunction.25 Zhang et al. conducted a randomized controlled clinical study on 78 patients with a 2-year postoperative follow-up, and the patients showed significant improvement in IELT and ejaculatory control compared with the preoperative period, as well as no complications such as erectile and ejaculatory dysfunction.26 In a nationwide study of 286 patients with PE treated with SDN in Korea, Yang et al. found that 96.6% of the patients felt that the symptoms of PE had subsided and only 0.4% of the patients had erectile dysfunction.27 Zhou et al. treated 78 cases of PPE with microscopic SDN. They showed significant improvement in IELT and patient and partner SIS scores at 3-month postoperative follow-up compared with the pre-treatment period, as well as no complications such as penile head numbness, abnormal penile erection and erectile dysfunction (ED).28
Liu et al. found that patients in the surgical treatment group presented significant improvements in IELT and ejaculatory control compared with the sham-operated group at 6-month follow-up. There were no severe complications such as ED.29 Genov et al. reported a patient with PPE in whom the conservative treatment had failed, who underwent microscopic SDN and who were followed up for 12 months after surgery – and found a 6-fold increase in IELT compared to preoperative measurements. The patient was free of symptoms of PE at the last follow-up, with no severe complications.30 Alyaev and Akhvlediani observed that the efficiency of the surgical group was 88% higher than that of the sham-operated group (10.2%), and no erectile dysfunction occurred after surgery.31 It is important to note that pharmacological treatment as the first-line treatment for PE is still widely accepted worldwide, and SDN is not mainstream treatment for PE, but a complementary rather than a substitute for non-surgical treatment.
This study showed that most patients treated with SDN showed significant improvement compared with those before treatment. However, the curative effects of some patients have not yet reached the clinical ideal. According to the efficacy assessment criteria, the curative effect in group A was significantly higher than in groups B and C. There was a correlation between curative effect and age. According to the IIEF-5 score and nocturnal penile tumescence test (NPT), the erectile function and erectile hardness in patients in the group A were significantly better than in the other 2 groups before and after surgery. In addition, the PEDT scores of patients in group A were significantly higher than in groups B and C before surgery.
In contrast, the PEDT scores of patients in group A were substantially lower than in groups B and C after surgery. The patients in group A had a better erectile function and erectile rigidity, and more significant improvement in PEDT scores before and after surgery. At the same time, it has been pointed out that there is a tendency for the values of each point of the penile biosensor threshold test to increase gradually with age in patients with PPE, and the sensitivity of the penile head was reduced to varying degrees.32, 33 It can be seen that PPE treatment with SDN should be performed as early as possible – optimally at the age of 22–30. It may be due to the patients’ higher penile sensitivity and better erectile function that the degree of postoperative improvement is relatively more apparent and the efficacy tends to be better. Postoperative complications were also analyzed, and the incidence of local pain, tethered edema, subcutaneous sclerosis, or poor appearance of penile foreskin in the 3 groups was not statistically significant. No complications such as abnormal penile erection or erectile dysfunction occurred in any patient, indicating that increasing age does not affect treatment safety. Thus, it can be seen that the efficacy of SDN in the treatment of PPE is remarkable, with few adverse effects. Moreover, the effectiveness of patients is closely related to their age, and the clinic should clarify the diagnosis early.
Limitations
There are several limitations to this study. First, the minimum age to be enrolled in the study was 22, since the legal age of marriage for men in China is 22, but in fact, most of the patients presented PE symptoms before they reached such age. At the same time, the number of patients over 45 years attending our clinic is low. In the future, we can further expand the age span in the study group in order to study the relationship between efficacy and age. Second, there is no uniform standard for the assessment of ejaculatory control, and the 3 questions we used (PEDT items 1, 2 and 3) for review may cause some inaccuracies. Third, the number of cases included in this study is limited, and the results of multicenter studies are lacking; further expansion of the sample size is needed in the future to reduce errors. Fourth, there is no unified surgical efficacy assessment standard. The Chinese guidelines for diagnosing and treating PE and the expert consensus criteria may be appropriate only for the Asian population. Future multi-geographic and multi-institutional studies are needed to clarify them further. Fifth, our patients did not have complications such as glans numbness, probably due to the appropriate number of dorsal penile nerves preserved during the procedure. Still, we did not determine how many dorsal nerves should be selectively resected in each patient to achieve optimal IELT prolongation.
Conclusions
The SDN as surgical treatment of PPE in different age groups has achieved certain results. The highest surgical efficiency (95.24%) was achieved in the 22–30 age group and the lowest (65%) in the 38–45 age group. Therefore, we believe that the best time for a such surgery is between 22 and 30 years of age.