















Abstract
Orthognathic surgery causes functional and aesthetic changes, which could affect patients’ quality of life (QOL). The current analysis assessed the impact of orthodontic-surgical treatment on the parameters affecting the QOL using different scoring systems. The criteria for inclusion were studies written in various languages that compared the effects of the intervention on patients’ QOL before surgery and at various periods after surgery (3 weeks to several months), which resulted in including 19 studies into this meta-analysis. The outcomes of these studies underwent random-effect modeling to calculate the mean difference (MD) and 95% confidence intervals (95% CIs) of the impact of different surgical techniques on clinical parameters, and publication bias was analyzed with Begg’s test. According to the total score of the Orthognathic Quality of Life Questionnaire (OQLQ), surgery significantly affected patients’ QOL after 2 months or less (p = 0.049), up to 6 months (p < 0.001), and when comparing 2 months or less with up to 6 months (2–6 months) (p < 0.001). In addition, the total Oral Health Impact Profile-14 (OHIP-14) score showed a significant difference in the QOL after 6 months (p = 0.003) and up to 12 months (p = 0.002) after surgery. Therefore, orthodontic-surgical treatment significantly improves patients’ QOL after surgery compared to before surgery.
Key words: quality of life, OHIP-14, oral function, orthodontic surgery, OQLQ
Introduction
Orthodontic surgery consisting of a combination of orthognathic surgery and orthodontic treatment is the optimal method for correcting dentofacial deformities,1, 2, 3 and results in the harmonization of the facial skeletal structure and anatomical–functional adjustments by rearranging the maxillary bones.4 Therefore, such treatment addresses biological, functional and aesthetic considerations.5 The treatment consists of several phases, including the initial planning, orthodontic preparation, orthognathic surgical repositioning of the facial skeleton, postsurgical orthodontic refinement, and the containment phase that follows the removal of the fixed orthodontic appliance.3, 6
The World Health Organization (WHO) defines the quality of life (QOL) as “the individual’s perception of his or her position in life in the context of the culture and value system in which he lives and in relation to his goals, expectations, standards, and concerns.”7 However, this is a broad and comprehensive concept that is affected in a complex way by physical health, psychological state, social relationships, and environment.7 The assessment of QOL is a rapidly expanding research area in the fields of medicine and dentistry,8 which have widely investigated the impact of various conditions on patients.9 Orthognathic surgery, by altering facial aesthetics, can affect personal attitudes, social attitudes and behaviors as it involves changes in the patients’ functional and aesthetic aspects.10, 11 These alterations may be associated with patient-reported changes in QOL levels.9
Dental problems can affect several factors, such as personal characteristics, personality traits12, 13 and QOL.14, 15, 16, 17 For instance, malocclusion detrimentally affects QOL, social interaction, interpersonal relationships, and psychological health.14 In addition, malocclusion had an increased detrimental effect on social wellbeing.15 Furthermore, one study found a correlation between skeletal malocclusion and myofascial pain, major depression, and chronic pain.16 Moreover, those with malocclusion may experience low self-esteem and social stigma.17
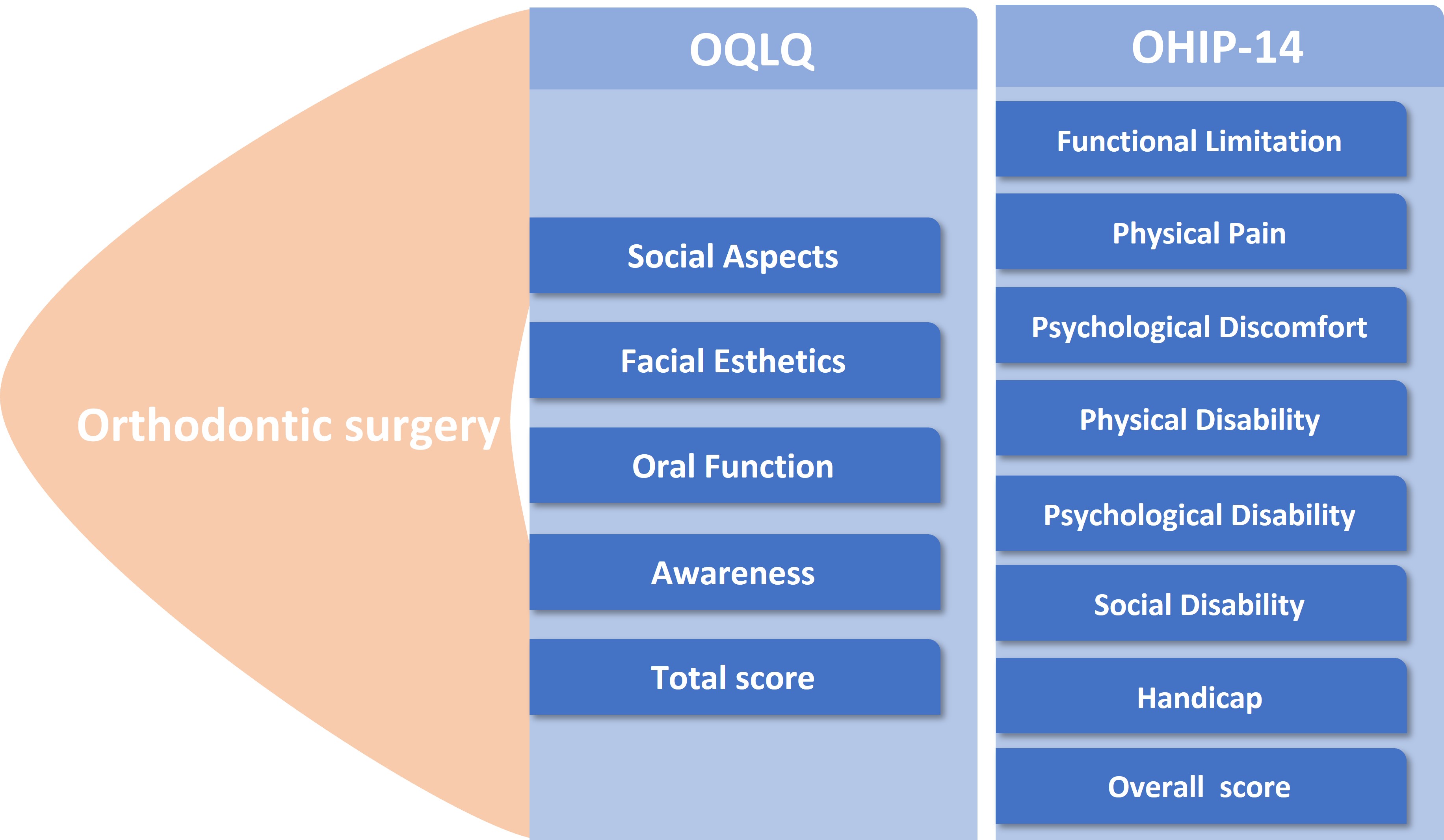
The term “body image” refers to a multi-faceted concept encompassing how a person perceives and conceptualizes their physical form.18 Dissatisfaction with personal physical appearance often stems from an inaccurate self-perception of physical characteristics. Among the validated numerical questionnaires assessing QOL is the Orthognathic Quality of Life Questionnaire (OQLQ) and Oral Health Impact Profile-14 (OHIP-14). The OQLQ has 22 questions on a 5-point Likert scale ranging from “does not bother me at all” (score 0) to “bothers me a lot” (score 4). The possible total range of points is 0–88, with a lower score preferable.19 Meanwhile, the responses for the OHIP-14 questionnaire use a 5-point Likert scale including 0 – never, 1 – hardly ever, 2 – occasionally, 3 – fairly often, and 4 – very often/every day. Higher OHIP-14 scores indicate a worse QOL, and lower scores indicate a better QOL.20
Objectives
The current study aimed to assess the impact of orthodontic surgery on a patient’s QOL compared to pre-surgery using numerical scores from validated questionnaires (OHIP-14 and OQLQ).
Materials and methods
Study design
This meta-analysis of clinical trials was included in the epidemiological declaration and followed a predetermined study design. Data collection and analysis encompassed the following databases: OVID, PubMed, Cochrane Library, Embase, and Google Scholar.
Data pooling
Studying the consequences and outcomes of surgery required the analysis of clinical investigations concentrating on assessing the influence of orthodontic surgery on QOL indicators using validated numerical scoring systems to compare post-surgery and pre-surgery scores. Only human-related studies were included, regardless of language and sample size. However, noninterventional research, such as reviews, editorials and letters, was excluded. Figure 1 depicts the entire study identification process.
Eligibility and inclusion criteria
A summary was created by analyzing the impact of orthodontic surgery treatments on postoperative outcomes and QOL scores compared to preoperative scores.
Only studies describing the impact of interventions on the parameters related to oral function, social impact, physical pain, and awareness, and those which used validated questionnaires were included in the sensitivity analysis.
The following criteria had to be met for an article to be considered for inclusion in the meta-analysis:
1. Studies in which patients with dentofacial abnormalities underwent orthodontic-surgical treatment;
2. Studies that used validated questionnaires to assess the QOL of patients before and after surgery or compared such patients to a control group free from any dentofacial deformity;
3. No restrictions were placed on the type of malocclusion, gender, age, ethnicity, study language, or publication date;
4. The intervention regimen compared postoperative outcomes with preoperative QOL parameters using different scoring systems.
The exclusion criteria were:
1. Studies that failed to use a numerical score to assess QOL based on different parameters;
2. Studies on subjects suffering from syndromes, such as dentofacial malformations or orofacial neoplasia, and those with cleft palates or exclusively affected on the lip or palate;
3. Studies on patients who did not undergo orthognathic surgery;
4. Studies not reporting QOL-related parameters after surgery compared to before surgery.
Identification
The Population, Intervention, Comparison, Outcome, and Study Design (PICOS) principle was used to outline a protocol of search strategies for: P (population) – orthodontic surgery subjects; I (intervention/exposure) – orthodontic surgery; and C (comparison) – various QOL parameters scored numerically using questionnaires (OHIP-14 and OQLQ). Oral function, social, body and psychological aspects, and awareness-related features are all study outcomes. Research design refers to whether or not clinical investigations were random.
A thorough search of the Cochrane Library, PubMed, OVID, Embase, and Google Scholar databases up until July 2022 was conducted using the keywords and related terms provided in Table 1. The titles and abstracts of all publications collated into a reference managing program were reviewed. Any research that did not establish a connection between orthodontic surgeries and their impact on quality of life was excluded from the study. Two authors (XL and XZ) served as reviewers to find relevant papers.
Screening
The following criteria were used to narrow down the data: study-related features in a standard format, the surname of the first author, the duration of the study, the year of publication, the country of the study, the design of the study, the population type recruited, the total number of subjects, demographic information, clinical and treatment characteristics, the information source, and the outcome. Each study was checked for bias, and the methodological quality of the chosen studies was rated by 2 authors (WZ and YZ) in a blinded manner.
Statistical analyses
Data analysis employed Jamovi 2.3 software (https://www.jamovi.org/download.html).21 The analysis utilized the standardized mean difference (MD) to measure outcomes by subtracting preoperative values from postoperative values and subtracting scores at 2 months from scores at 6 months post-surgery. Lower values indicated better QOL for both scoring systems. A random-effects model was fitted to the data, and the constrained maximum likelihood estimator calculated the level of heterogeneity (τ2). In addition to the τ2 estimate, the Q-test for heterogeneity and the I2 statistic are provided. Any level of heterogeneity identified (i.e., τ2 > 0 regardless of the Q-test findings) led to the calculation of a prediction interval for the true outcomes. Studentized residuals and Cook’s distances allowed to determine whether the studies may be outliers and their importance within the model. Studies with a studentized residual greater than 100 × (1 − 0.05/(2 × kth)) percentile of a standard normal distribution were regarded as potential outliers (using the Bonferroni correction with two-sided α = 0.05 for included studies). Studies considered influential had a Cook’s distance greater than the median plus 6 times the interquartile range (IQR) of Cook’s distances. Utilizing the standard error of the observed results as a predictor, the rank correlation test and the regression test examined the possibility of publication bias.
Results
After reviewing 902 relevant studies, 19 studies published between 2008 and 2022 fit the inclusion criteria.7, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39 Table 2 summarizes the review findings and includes study characteristics such as year, country, the total number of subjects, and the scoring system used.
Orthognathic Quality of Life Questionnaire
The analysis of studies assessing QOL with the OQLQ score involved 20 different subgroup analyses using 5 score parameters, with each parameter analyzed for 4 different comparisons. Most studies showed a significant impact of the intervention on QOL by demonstrating lower postoperative OQLQ scores compared to preoperative scores, and lower scores after 6 months compared to 2 months. However, social aspects (up to 12 months), facial aesthetics (up to 12 months), oral function (2 months or less and up to 12 months), awareness (2 months or less and up to 12 months), and the total score (up to 12 months) were not significantly impacted by surgery, as shown in Table 3 and Figure 2, Figure 3, Figure 4.
Oral Health Impact Profile-14
The evaluation of studies assessing QOL using the OHIP-14 score included the analysis of 16 different subgroups using 8 score parameters, with each parameter compared at 2 recovery periods, as shown in Table 3. All 16 subgroup analyses showed significantly lower OHIP-14 scores post-surgery and at 6 and 12 months, for all parameters (Figure 5, Figure 6).
The heterogeneity of different analyses is expressed in Table 3 as τ2, I2, Q-test, and Cook’s distances, the latter of which estimates the influence of a data point and indicates the number of studies that could be considered overly influential. Most models showed significant heterogeneity for both scoring systems (OHIP-14 and OQLQ), while only 5 analyses showed nonsignificant heterogeneity (Table 3). Variability of I2 values ranged from 7% to 99%.
Risk of bias
The risk of bias assessment used Egger’s regression and Begg’s test, as shown in Table 3. All parameters related to the OQLQ score, including social aspects, facial aesthetics, oral function, awareness, and the total score, and analyzed for differences at 2 months or less, 2–6 months, and up to 12 months showed nonsignificant publication bias ranging from p = 0.06 to p = 0.99. On the other hand, the analysis of 8 parameters related to OHIP-14 score and analyzed at up to 6 and 12 months post-surgery showed different results, with significant publication bias in 12 parameters (p < 0.05). This included functional limitation (up to 12 months), physical pain (up to 6 and 12 months), psychological discomfort (up to 6 months), physical disability (up to 12 months), psychological disability (up to 6 months), social disability (up to 6 months), handicap (up to 6 months), and the total OHIP-14 score itself (up to 6 and 12 months). The analysis of other OHIP-14-related parameters showed nonsignificant publication bias, as shown in Table 3.
Discussion
The current meta-analysis included 19 studies assessing the impact of orthodontic-surgical treatment on QOL using the OQLQ and OHIP-14 scoring systems. According to the total OQLQ score, patients’ QOL significantly improved after surgery within 2 months or less (p = 0.049), up to 6 months (p < 0.001), and when comparing 2 months or less with 2–6 months (p < 0.001). In addition, the OHIP-14 scores showed a significant difference in QOL post-surgery at 6 months (p = 0.003) and up to 12 months (p = 0.002).
Quality of life is a vital indicator at any stage of surgical orthodontic treatment and is crucial when addressing the patient’s mental health.24 Functional constraints, decreased masticatory efficiency, discomfort, edema, sensorineural abnormalities, and morbidities specific to the surgical process all contribute to a significant drop in QOL in the postoperative period, as reported by Choi et al.26 In contrast, research by Lee et al. demonstrated that 6 weeks after surgery, patients experienced a considerable improvement in QOL associated with cosmetic facial elements.33 The current study, which obtained data through meta-analytical estimation of QOL in patients 6 weeks after surgery using the OQLQ questionnaire, corroborates these findings by demonstrating that QOL for social aspects, functional aspects, awareness, and the total score did not change from the initial to final stages (without any treatment). The results also demonstrated that facial aesthetics significantly improved 6 weeks post-surgery compared to pre-treatment levels. If the OQLQ questionnaire is directly related to dentofacial experiences, these results make sense, given that orthodontic-surgical treatment corrects the dentofacial abnormality. Compared to questionnaires that take a more generalized approach to oral health, the level of specificity increases the sensitivity with which QOL changes can be detected, even in their earliest stages.33
Many studies show a link between dentofacial abnormalities and psychological issues,40, 41, 42 and when comparing patients with other types of malocclusion,40 those with class III malocclusion are more likely to experience feelings of insecurity, depression and psychological stress. Such issues arise due to the difficulty of hiding the skeletal discrepancy caused by the protrusion of the jaw and the concavity of the facial profile, both of which are viewed as unattractive. Patients with class III malocclusion have orthognathic surgery around 4 years earlier than patients with other abnormalities,40 suggesting that psychological factors play a role in the decision to undertake surgical treatment. Variations in emotional behavior, depression intensity and self-esteem are linked to gender, and there are more noticeable alterations to the female facial profile.22, 40, 43, 44 Moreover, as shown by Bortoluzzi et al., QOL has a greater effect on females and elicits diverse responses from patients of different ages who suffer from dentofacial deformities.22, 45
Bias regarding the type of deformities and the number of patients between groups may influence the results due to the cross-sectional design of research and the inclusion of multiple types of malocclusion in the same sample.46 Confounding factors such as gender, age, marital status, and type of malocclusion were taken into account in the review and data analysis in just 12 of the included studies. This could help account for the relatively high I2 value found in this meta-analysis. However, the direction of the impact in the individual results demonstrated the same effect tendency, even in meta-analyses that reported considerable heterogeneity.
Limitations
Age, gender, type of malocclusion, and patient expectations of orthodontic-surgical treatment are confounding factors that are intrinsic to the issue and may alter the estimations if not controlled by adequate sampling and randomization techniques. Since most of the studies were uncontrolled and observational, they could not control the exposure factor or use random allocation methods. Also, some studies had a small sample size of less than 20 subjects. In addition, not all studies measured the outcomes at the same time after surgery, and many studies were excluded due to not stating the exact timing of the results.
Conclusions
Orthodontic-surgical treatment resulted in a significant enhancement in patient QOL after surgery compared to before surgery. The OHIP-14 demonstrated significant improvement in all elements covered by this questionnaire, while the OQLQ showed varied findings that depended on the time after surgery. However, future multicenter clinical studies are required to make more definitive conclusions.





